Brachial plexus anatomy in detail with labelled diagram, various approaches of brachial plexus blocks with landmark technique with indications and complications,
Reading File
Finding Sources
Finding Sources
Searching the Web
brachial plexus anatomy labeled diagram nerve roots trunks divisions cords
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed to write a comprehensive, well-illustrated answer. Let me compile it:
Brachial Plexus - Complete Anatomy & Regional Block Guide
PART 1: ANATOMY OF THE BRACHIAL PLEXUS
Overview
The brachial plexus is a somatic nerve plexus formed by the anterior rami (roots) of C5-C8 and most of T1. It originates in the neck, passes laterally and inferiorly over the first rib, and enters the axilla. It provides ALL motor and sensory innervation to the upper limb.
Components (medial to lateral, proximal to distal):
Roots → Trunks → Divisions → Cords → Terminal branches (Mnemonic: "Randy Travis Drinks Cold Beer")
Labelled Diagrams
Diagram 1 - Anatomical course (Gray's Anatomy for Students):

Diagram 2 - Schematic of formation (Barash Clinical Anesthesia):
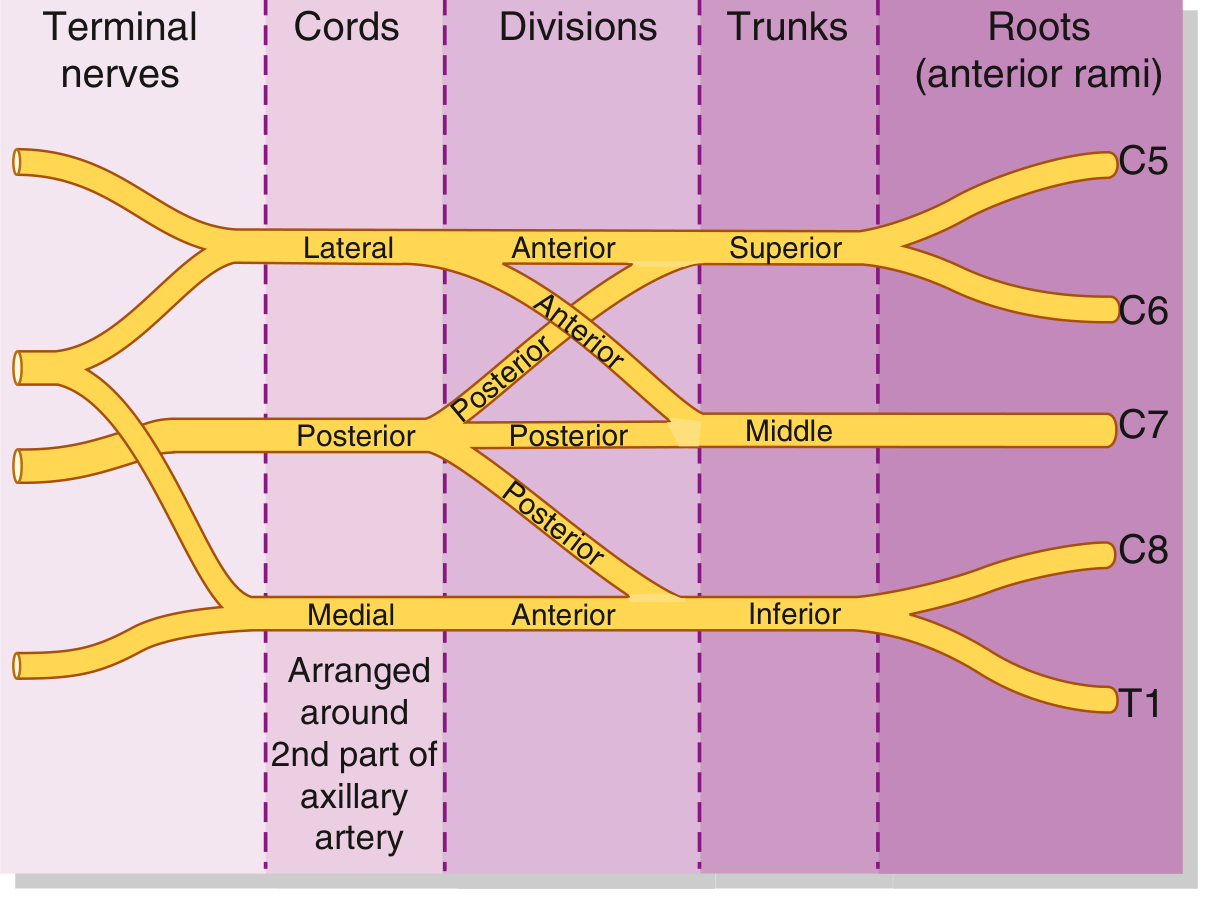
Diagram 3 - Full colour schematic (Barash Clinical Anesthesia, 9e):
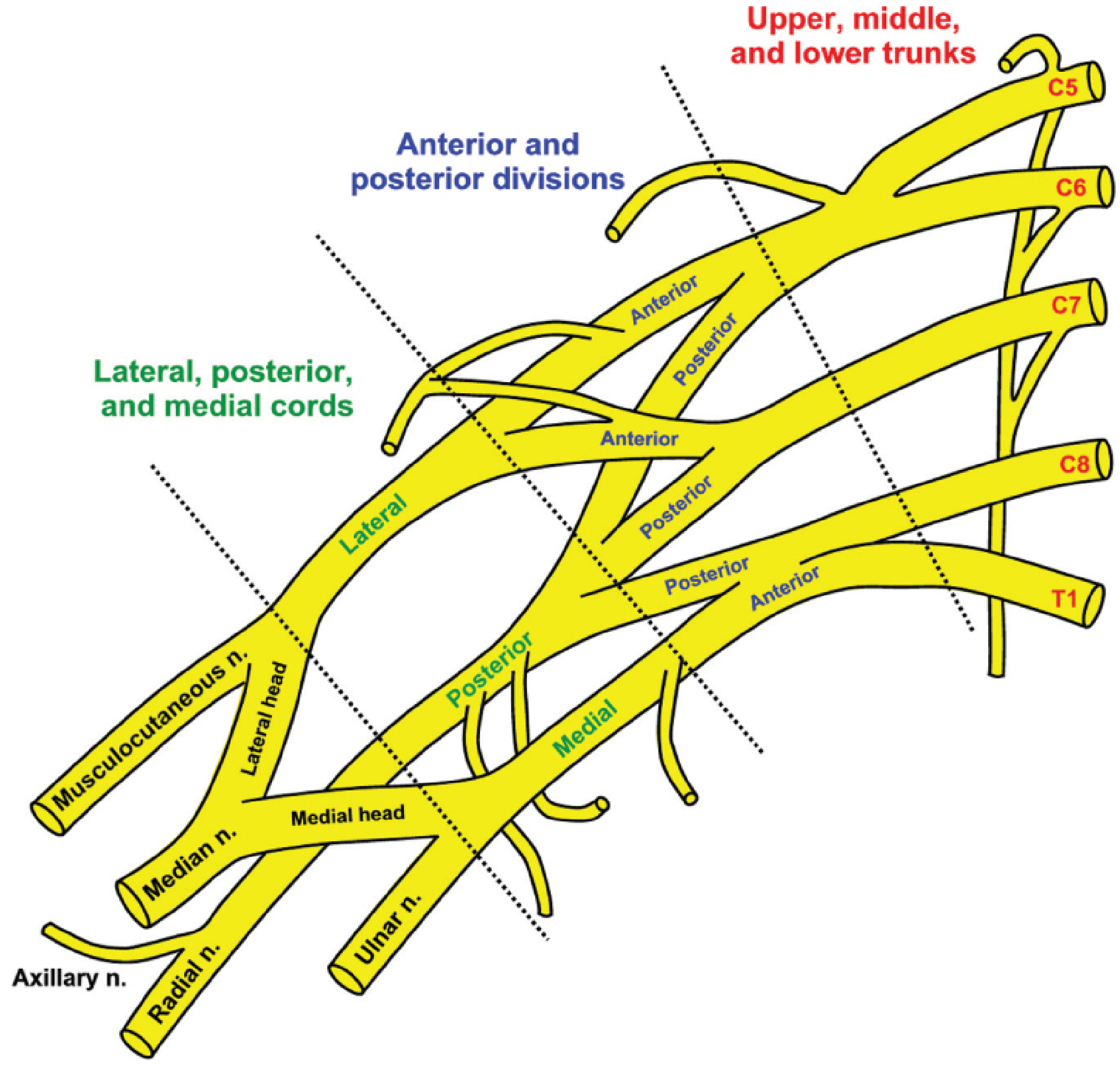
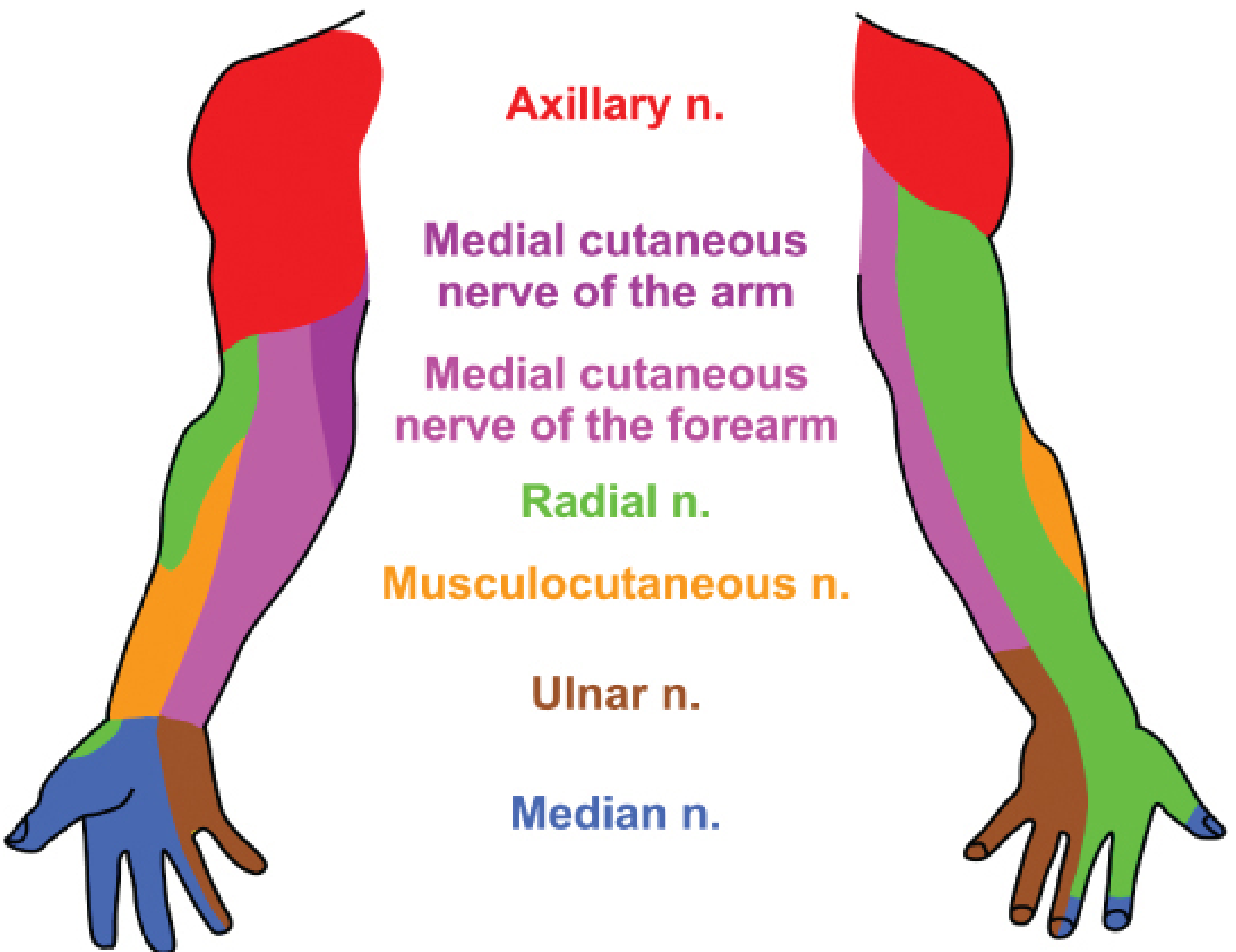
Diagram 4 - Cutaneous innervation of the upper limb:
Components in Detail
1. ROOTS (C5-T1)
- The anterior rami of C5, C6, C7, C8, and T1
- Emerge from their intervertebral foramina and travel in grooves between the anterior and posterior tubercles of the transverse processes
- Exit between the anterior scalene and middle scalene muscles, above and posterior to the subclavian artery
- Receive gray rami communicantes from the sympathetic trunk (carry postganglionic sympathetic fibres)
- Enclosed in the interscalene fascial sheath (an extension of prevertebral fascia)
Pre-fixed plexus: C4 contributes significantly (C4-C8 pattern)
Post-fixed plexus: T2 contributes significantly (C6-T2 pattern)
2. TRUNKS (3)
The three trunks pass over the first rib, crossing the base of the posterior triangle of the neck:
| Trunk | Formation | Position |
|---|---|---|
| Superior (Upper) | C5 + C6 | Above subclavian artery |
| Middle | C7 alone | Above subclavian artery |
| Inferior (Lower) | C8 + T1 | On rib I, posterior/below subclavian artery |
Branches from trunks:
- Superior trunk: Suprascapular nerve (C5, C6) - supplies supraspinatus and infraspinatus
- Superior trunk: Nerve to subclavius (C5, C6)
3. DIVISIONS (6 total - 2 per trunk)
Each trunk divides into an anterior and a posterior division at the lateral border of the first rib (approximately behind the clavicle):
- Anterior divisions supply flexor (anterior) compartment muscles
- Posterior divisions supply extensor (posterior) compartment muscles
- There are NO named branches from the divisions
4. CORDS (3) - Named for their relationship to the 2nd part of the axillary artery
| Cord | Formation | Position to artery |
|---|---|---|
| Lateral cord | Anterior divisions of superior + middle trunks (C5, C6, C7) | Superolateral |
| Medial cord | Anterior division of inferior trunk (C8, T1) | Inferomedial |
| Posterior cord | Posterior divisions of ALL three trunks (C5-T1) | Posterior |
Branches from cords:
Lateral cord:
- Lateral pectoral nerve (C5-C7) - pectoralis major
- Musculocutaneous nerve (C5-C7) - coracobrachialis, biceps, brachialis; lateral cutaneous nerve of forearm
- Lateral root of median nerve
Medial cord:
- Medial pectoral nerve (C8, T1) - pectoralis minor and major
- Medial cutaneous nerve of arm (C8, T1)
- Medial cutaneous nerve of forearm (C8, T1)
- Ulnar nerve (C7, C8, T1)
- Medial root of median nerve
Posterior cord:
- Upper subscapular nerve (C5, C6) - subscapularis
- Thoracodorsal nerve (C6-C8) - latissimus dorsi
- Lower subscapular nerve (C5, C6) - subscapularis and teres major
- Axillary nerve (C5, C6) - deltoid and teres minor
- Radial nerve (C5-C8, T1) - all posterior compartment muscles of arm and forearm
5. TERMINAL BRANCHES (5 major)
| Nerve | Root | Cord | Key Motor | Key Sensory |
|---|---|---|---|---|
| Musculocutaneous | C5-C7 | Lateral | Coracobrachialis, biceps, brachialis | Lateral forearm |
| Median | C5-T1 | Lateral + Medial | Forearm flexors (except FCU+medial FDP), thenar muscles, lumbricals 1&2 | Lateral 3.5 fingers (palm) |
| Ulnar | C7-T1 | Medial | FCU, medial FDP, hypothenar, most intrinsics | Medial 1.5 fingers |
| Radial | C5-T1 | Posterior | All posterior arm/forearm extensors | Posterior arm, forearm, lateral dorsum hand |
| Axillary | C5-C6 | Posterior | Deltoid, teres minor | Regimental badge area (lateral upper arm) |
Fascial Sheaths and Topography (Clinically Important)
The plexus is enclosed throughout its course:
- Interscalene fascial sheath - between scalene muscles (target for interscalene block)
- Axillary sheath - continuation in the axilla (target for axillary block)
The plexus passes in close relationship to:
- Subclavian/axillary artery - arteries are key landmarks for all blocks
- Phrenic nerve - runs anterior to scalenus anterior (vulnerable in interscalene and supraclavicular blocks)
- Pleural dome/lung apex - at risk in supraclavicular blocks
- Vertebral artery - at risk in deep interscalene injections
- Sympathetic chain - produces Horner syndrome if blocked
PART 2: APPROACHES TO BRACHIAL PLEXUS BLOCKS
Overview - Level of Block vs. Coverage
| Approach | Level Blocked | Ideal Surgery |
|---|---|---|
| Interscalene | Roots/upper trunks (C5-C7) | Shoulder, proximal humerus |
| Supraclavicular | Distal trunks/divisions | Elbow, forearm, hand ("spinal of the arm") |
| Infraclavicular | Cords | Elbow and distal; catheter placement |
| Axillary | Terminal branches | Forearm and hand (distal to elbow) |
1. INTERSCALENE BLOCK (ISB)
Level: Roots/upper trunks of the brachial plexus, between anterior and middle scalene muscles
Indications:
- Shoulder surgery (rotator cuff repair, shoulder arthroplasty)
- Proximal humerus surgery, clavicle fracture fixation
- Acute shoulder dislocation reduction
- Postoperative analgesia following shoulder surgery
- AC joint procedures
Contraindications (absolute/relative):
- Contralateral phrenic nerve palsy (ABSOLUTE - bilateral phrenic block = respiratory failure)
- Contralateral hemidiaphragm paralysis
- Severe COPD or pulmonary insufficiency (phrenic palsy will worsen)
- Contralateral vocal cord paralysis
- Local infection, severe coagulopathy, patient refusal
- Bilateral ISB is ABSOLUTELY CONTRAINDICATED
Landmark Technique:
- Patient supine, head rotated 30-45° away from the side to be blocked
- Ask patient to lift and rotate head against resistance to define the sternocleidomastoid (SCM)
- Identify the interscalene groove by rolling fingers posteriorly off the posterior border of the clavicular head of the SCM at the level of the cricoid cartilage (C6)
- The external jugular vein often crosses this groove at C6 level - useful landmark
- The groove lies between anterior scalene (anteriorly) and middle scalene (posteriorly)
- Insert needle at 45° caudally and slightly medially
- Endpoint: paresthesia to shoulder/arm OR motor response with nerve stimulator (deltoid twitch = axillary n., biceps = musculocutaneous n.)
- Inject 20-40 mL of local anesthetic
Complications:
- Ipsilateral phrenic nerve palsy (virtually 100% incidence with nerve stimulator technique; ~27% with low-volume ultrasound): reduces ipsilateral hemidiaphragm function by ~25% - relevant in pulmonary compromise
- Horner syndrome (ptosis, miosis, anhidrosis): proximal tracking to cervicothoracic ganglion - requires reassurance only
- Recurrent laryngeal nerve block: hoarseness - especially concerning with contralateral vocal cord palsy
- Vertebral artery injection: immediate seizure activity (as little as 1 mL causes seizure)
- Spinal/epidural spread: possible; intrathecal injection/cervical syrinx reported
- Pneumothorax: less common than supraclavicular, but possible given proximity to apical pleura
- C8-T1 (ulnar) sparing: inferior trunk not well-blocked; interscalene NOT suitable for hand/forearm surgery
2. SUPRACLAVICULAR BLOCK
Level: Distal trunks / proximal divisions - the most compact point of the brachial plexus ("spinal of the arm")
Indications:
- Surgery at or distal to the elbow: forearm and hand procedures
- Upper arm surgery (with intercostobrachial nerve supplement for tourniquet)
- Dense, rapid-onset surgical anesthesia needed
- NOT ideal for isolated shoulder surgery (suprascapular nerve not reliably blocked)
Landmark Technique:
- Patient supine, head turned 30° to contralateral side, arm adducted at side
- Identify the supraclavicular fossa (depression just above mid-clavicle)
- The subclavian artery is palpable at the lateral border of the anterior scalene
- Insert needle 1-2 cm above the clavicle at the posterior border of the SCM, directed caudally and medially at 45-60° to skin
- Endpoint: paresthesia to hand/forearm OR nerve stimulator response (finger/wrist movement)
- First rib acts as a natural barrier - needle should not penetrate beyond it
- Inject 25-40 mL of local anesthetic in divided doses
Complications:
- Pneumothorax (0.5-6%): most feared; risk is reduced but not eliminated with ultrasound; peak incidence 6-12 hours post-block
- Phrenic nerve block (40-60%): similar precautions to ISB regarding pulmonary reserve
- Horner syndrome: sympathetic chain proximity
- Subclavian artery puncture/hematoma
- Ulnar nerve sparing (~10%): lower trunk can be missed; requires careful technique to identify inferior trunk
- Perineural catheters are inferior at this site compared to infraclavicular approach
3. INFRACLAVICULAR BLOCK
Level: Cords of the brachial plexus (medial, lateral, posterior), surrounding the axillary artery
Indications:
- Surgery at or distal to the elbow; elbow, forearm, wrist, and hand
- Best approach for continuous perineural catheter (most stable catheter position; no arm manipulation needed)
- Patients who cannot abduct the arm (e.g., painful shoulder, frozen shoulder)
- When supraclavicular block is undesirable (e.g., compromised pulmonary reserve)
- Upper arm surgery when combined with intercostobrachial nerve block
Landmark Technique (Raj/Classic approach):
- Patient supine, arm slightly abducted; shoulder abduction to 90° facilitates visualization
- Identify the coracoid process (bony landmark just medial to glenohumeral joint) and the clavicle
- Insert needle 2 cm medial and 2 cm caudal to the coracoid process, directed perpendicular to the skin (or slightly caudal)
- Target is the posterior cord (posterior to axillary artery) - single injection here gives complete block
- Endpoint: nerve stimulator - hand extension/wrist extension (radial/posterior cord) OR paresthesia
- Inject 30-40 mL of local anesthetic posterior to the axillary artery
Complications:
- Pneumothorax: lower risk than supraclavicular but not zero (deeper needle path)
- Axillary artery/vein puncture: hematoma; axillary vein is medial/inferior
- Deep nature of block: needle tip visualization is difficult; steep needle angle worsens this
- Musculocutaneous nerve sparing is rare (branches proximally, but captured within infraclavicular fascial space)
- Lower risk of phrenic nerve palsy compared to ISB or supraclavicular
- Lower risk of pneumothorax than supraclavicular approach
- No Horner syndrome typically
4. AXILLARY BLOCK
Level: Terminal branches of the brachial plexus (median, ulnar, radial nerves) around the axillary artery in the axilla
Indications:
- Surgery distal to the elbow: forearm, wrist, hand procedures
- Safest approach - no risk of pneumothorax or phrenic nerve palsy
- Pediatric patients and outpatient procedures
- Patients with severe pulmonary disease (safe choice)
- Supplementation of incomplete proximal blocks
Contraindications:
- Axillary lymphadenopathy, infection in axilla
- Inability to abduct and externally rotate the arm
- Note: axillary nerve, musculocutaneous nerve, and medial brachial cutaneous nerve branch proximal to the injection site and are NOT blocked by the axillary approach
Landmark Technique:
- Patient supine with arm abducted 90° and elbow flexed 90° (hand behind head)
- Palpate the axillary artery pulse as high in the axilla as possible
- The brachial plexus terminal nerves lie in specific positions around the artery:
- Median nerve: anterosuperior to artery
- Ulnar nerve: posteroinferior to artery
- Radial nerve: posterior to artery
- Musculocutaneous nerve: has already left the sheath, lies within coracobrachialis muscle
- Transarterial technique: Advance needle through the artery; inject 20 mL posterior (for radial/ulnar) and 20 mL anterior (for median) after withdrawing to skin
- Perivascular (fascial click) technique: Insert needle at 45° to skin alongside artery until fascial click is felt; inject 30-40 mL
- Multiple injection technique (most reliable): Use nerve stimulator or ultrasound to localize each nerve individually (5-10 mL per nerve)
- Musculocutaneous nerve must be blocked separately: inject 5-10 mL into the body of the coracobrachialis muscle
Complications:
- Axillary artery/vein puncture: hematoma (most common)
- Local anesthetic systemic toxicity (LAST): axilla is highly vascular; small veins traumatized by needle placement increase absorption - aspirate frequently
- Infection: less common; axilla is not a sterile area
- Neuropathy: direct nerve trauma
- Incomplete block: most common problem - axillary, musculocutaneous, and intercostobrachial nerves require separate blocks
- No pneumothorax risk
- No phrenic nerve palsy risk
- No Horner syndrome
5. MIDHUMERAL BLOCK
An alternative to axillary block, performed at the mid-humerus level targeting the four terminal nerves individually. Less commonly used but useful when axilla is inaccessible.
Summary Comparison Table
| Feature | Interscalene | Supraclavicular | Infraclavicular | Axillary |
|---|---|---|---|---|
| Level | Roots/Trunks | Trunks/Divisions | Cords | Terminal branches |
| Best for | Shoulder | Elbow-hand | Elbow-hand/catheter | Forearm/hand |
| Pneumothorax | Rare | 0.5-6% | Low | None |
| Phrenic nerve | ~100% | 40-60% | Rare | None |
| Horner | Common | Yes | Rare | None |
| Volume | 10-20 mL | 15-30 mL | 30-40 mL | 30-40 mL |
| Ulnar sparing | Common | 10% | Rare | Rare |
| Catheter | Good | Suboptimal | Best | Suboptimal |
General Complications of All Brachial Plexus Blocks
- Local anesthetic systemic toxicity (LAST): seizures, cardiovascular collapse - have intralipid available
- Peripheral nerve injury: incidence ~1.7-3% transient; ~0.04% persistent; from direct trauma, intraneural injection, ischemia
- Infection: cellulitis, abscess, meningitis (epidural spread)
- Hematoma: especially in anticoagulated patients
- Allergic reaction: rare with amide local anesthetics
- Failed block / incomplete anesthesia: requires supplementation or GA conversion
Sources: Gray's Anatomy for Students (Elsevier), Barash Clinical Anesthesia 9e, Miller's Anesthesia 10e, Morgan & Mikhail's Clinical Anesthesiology 7e
Last in detail with management
Finding Sources
Finding Sources
Searching PubMed
"local anesthetic systemic toxicity" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading Article
PMID: 38705678
Reading File
Reading File
I now have all the authoritative content needed for a comprehensive LAST answer. Let me compile it:
Local Anesthetic Systemic Toxicity (LAST) - Complete Guide
Definition
LAST is the accumulation of local anesthetic in the systemic circulation - from either inadvertent intravascular injection or excessively rapid absorption - resulting in toxic plasma concentrations that primarily affect the CNS and cardiovascular system. It can follow any local anesthetic administered by any route.
Incidence
- Overall incidence: ~0.03% for peripheral nerve blocks (higher with multiple/large volume blocks)
- Cardiac arrest from LAST: ~1 in 25,000 peripheral nerve blocks
- Incidence has declined with ultrasound guidance but has NOT been eliminated
- LAST is underreported, especially delayed presentations
Pharmacology Basis: Why LAST Occurs
Local anesthetics work by blocking voltage-gated Na+ channels. At toxic plasma concentrations, this Na+ channel blockade occurs in NON-TARGET tissues - principally the brain and myocardium.
Factors affecting plasma concentration (and therefore LAST risk):
- Rate of absorption - highest to lowest vascularity of block site:
- Intercostal > caudal > epidural > brachial plexus > sciatic/femoral > subcutaneous
- Total dose administered (mg = concentration × volume)
- Use of epinephrine - reduces peak plasma concentration by 10-20% via vasoconstriction
- Drug metabolism - amide LAs (lidocaine, bupivacaine, ropivacaine) metabolized by liver; ester LAs (procaine, chloroprocaine) by plasma cholinesterase
- Protein binding - only free (unbound) drug is active; hypoalbuminemia increases risk
Risk Factors for LAST
(ASRA Third Practice Advisory, adapted from Barash Clinical Anesthesia 9e)
| Patient Factors | Drug Factors | Setting |
|---|---|---|
| Extremes of age (elderly, neonates) | Highly potent agents (bupivacaine > ropivacaine > lidocaine) | Non-hospital setting |
| Low muscle mass | Highly vascular block site | Non-anesthesiologist performing block |
| Female sex | High total dose | |
| Pre-existing arrhythmias or heart failure | Prolonged infusion | |
| Metabolic disease / diabetes | ||
| Hepatic insufficiency (reduced clearance) | ||
| CNS disease (lowered seizure threshold) | ||
| Low plasma protein binding | ||
| Hypercarbia, acidosis, hypoxemia (all potentiate toxicity) |
Toxic Dose Thresholds (Maximum Safe Doses)
| Agent | Without Epinephrine | With Epinephrine |
|---|---|---|
| Lidocaine | 3-4 mg/kg | 7 mg/kg |
| Bupivacaine | 2 mg/kg | 2.5 mg/kg |
| Ropivacaine | 3 mg/kg | 3.5 mg/kg |
| Mepivacaine | 4-5 mg/kg | 7 mg/kg |
| Levobupivacaine | 2.5 mg/kg | 3 mg/kg |
Note: Bupivacaine 0.75% is NEVER used for epidural anesthesia in obstetrics (accidental IV injection = cardiac arrest)
Pathophysiology
CNS Mechanism
LAs cross the blood-brain barrier readily. CNS effects are concentration-dependent:
- Low concentrations → CNS depression (sedation, analgesia)
- Moderate concentrations → CNS excitation (inhibitory neurons blocked first, paradoxical excitation)
- High concentrations → Global CNS depression (coma, respiratory arrest)
Cardiovascular Mechanism
CVS toxicity occurs at higher plasma concentrations than CNS toxicity (ratio ~7:1 for lidocaine, ~3:1 for bupivacaine - hence bupivacaine is more cardiodepressive).
Mechanisms of cardiotoxicity:
- Na+ channel blockade in cardiomyocytes → slows conduction (prolonged PR interval, wide QRS)
- K+ and Ca2+ channel blockade → impaired repolarization
- Mitochondrial dysfunction → impaired fatty acid oxidation in cardiac muscle
- Bupivacaine's unique danger: binds Na+ channels during the activated AND inactivated states with slow dissociation ("fast in, slow out") → accumulates with each cardiac cycle → refractory ventricular arrhythmias
- Pulmonary vasoconstriction: rising LA concentrations cause pulmonary artery hypertension even before significant cardiac depression
- CNS-mediated cardiovascular depression: bupivacaine disrupts brainstem baroreflex regulation
Relative CVS safety (least → most cardiotoxic):
Lidocaine < Ropivacaine < Levobupivacaine < Bupivacaine
(Animal models: dose to collapse - lidocaine 127 mg/kg, ropivacaine 42 mg/kg, levobupivacaine 27 mg/kg, bupivacaine 22 mg/kg)
Clinical Presentation
Typical Sequential Progression
CNS PRODROME ──────────────────────────────► CVS COLLAPSE
↓ ↓ ↓
Early excitatory CNS depression Cardiovascular
(inhibition of phase
inhibitory neurons)
CNS Manifestations (Dose-Dependent - Lidocaine Model)
| Plasma Concentration | Symptoms |
|---|---|
| 1-5 mcg/mL | Analgesia (therapeutic) |
| 5-10 mcg/mL | Circumoral/tongue numbness, metallic taste, tinnitus, dizziness, lightheadedness, visual disturbances |
| 10-15 mcg/mL | Slurred speech, muscle twitching, tremors → SEIZURES, unconsciousness |
| 15-25 mcg/mL | Coma, respiratory arrest |
| >25 mcg/mL | Cardiovascular depression |
CVS Manifestations
Early:
- Hypertension, tachycardia (adrenergic stimulation)
- ECG: PR prolongation, QRS widening
Progressive:
- Hypotension (vasodilation + myocardial depression)
- Bradycardia, heart block
- ECG: ST changes, bundle branch block
Severe:
- Ventricular arrhythmias (VT, VF, torsades de pointes)
- Complete heart block
- Asystole
- Cardiovascular collapse and cardiac arrest
IMPORTANT Atypical Presentations
- Pure CVS without CNS prodrome: Occurs when CNS signs are masked by concurrent sedation/GA. May be the first manifestation - especially dangerous.
- Delayed onset LAST: Symptoms may appear 1-60 minutes after injection (peak absorption from tissue depot). Always monitor 30 min post-block.
- Subtle CNS signs only: Agitation, confusion, or bizarre behavior in a sedated patient.
- Bupivacaine cardiac arrest: Can occur without any preceding CNS signs, especially with accidental IV injection.
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Vasovagal syncope | HR decreases, brief, resolves spontaneously |
| Anaphylaxis | Urticaria, bronchospasm, hypotension without dysrhythmia |
| Pneumothorax | Respiratory distress, absent breath sounds |
| High spinal/epidural | Hypotension + bradycardia + dyspnea |
| Hypoglycaemia | Low BGL, responds to glucose |
| Seizure (epileptic) | No antecedent block, known history |
| Pulmonary embolism | Acute hypoxia, raised JVP |
Prevention of LAST
- Aspirate before injection and before each subsequent 5 mL aliquot
- Incremental injection: inject in 5 mL aliquots, 15-30 seconds apart (allows CNS symptoms to manifest before full dose given)
- Epinephrine marker dose: epinephrine 5 mcg/mL (1:200,000) added to LA - if accidentally intravascular, causes HR rise >20 bpm and systolic BP rise >15 mmHg within 1 minute
- Adhere to maximum safe doses (calculate mg/kg before every block)
- Ultrasound guidance: visualize needle tip and LA spread; reduce doses
- Avoid highly vascular sites without aspiration
- Choose safer agents: prefer ropivacaine over bupivacaine when equivalent efficacy expected
- Pre-treatment: midazolam raises seizure threshold (but masks early CNS signs - two-edged sword)
- Correct modifiable factors: avoid acidosis, hypoxia, hypercarbia which potentiate LAST
Management of LAST - Step-by-Step
(Based on ASRA 3rd Practice Advisory 2017, from Barash Clinical Anesthesia 9e)
IMMEDIATE ACTIONS (First 60 seconds)
STEP 1 - CALL FOR HELP
- Activate emergency response immediately at first sign of LAST
- Call for resuscitation cart, lipid emulsion, and defibrillator
- Call for cardiopulmonary bypass capability alert if available
STEP 2 - AIRWAY MANAGEMENT (Simultaneous)
- 100% oxygen via facemask or intubation
- Ventilate to normocapnia (avoid hypercarbia which potentiates toxicity)
- If seizures → may require intubation to protect airway
- Correct: hypoxia, hypercarbia, acidosis (all worsen LAST significantly)
- If intubating: succinylcholine preferred (short-acting) to minimize prolonged acidosis from fasciculations
STEP 3 - SEIZURE MANAGEMENT
- Benzodiazepines first-line: midazolam 0.05-0.1 mg/kg IV; lorazepam 0.05 mg/kg IV; diazepam 0.1 mg/kg IV
- Propofol (small doses: 0.5-1 mg/kg) - alternative but caution as it causes cardiovascular depression; avoid if haemodynamically unstable
- Thiopentone (1-2 mg/kg) for refractory seizures
- Small dose succinylcholine to stop motor activity if seizures are intractable (prevents rhabdomyolysis, acidosis, hypoxia) - NOTE: this terminates motor activity only, NOT cerebral electrical activity
- AVOID: phenytoin (sodium channel blocker - worsens cardiac toxicity)
STEP 4 - LIPID EMULSION THERAPY (Intralipid 20%) ⭐ KEY TREATMENT
This is the definitive therapy for LAST, especially bupivacaine-induced cardiac toxicity.
Dosing Protocol (ASRA 2017):
| Step | Dose | Details |
|---|---|---|
| Initial bolus | 1.5 mL/kg lean body weight (= ~100 mL for a 70 kg patient) | IV over 2-3 minutes |
| Infusion | 0.25 mL/kg/min (~200-250 mL over 15-20 min for 70 kg) | Start immediately after bolus |
| Repeat bolus | 1.5 mL/kg | If cardiovascular instability persists after 5 min |
| Increase infusion | Up to 0.5 mL/kg/min | For persistent hypotension |
| Continue infusion | Minimum 10 minutes after circulatory stability achieved | |
| Maximum dose | ~10-12 mL/kg over initial 30 minutes | Upper limit for initial dosing |
Mechanisms of lipid emulsion:
- "Lipid shuttle" / lipid sink effect: creates a lipid phase in blood that sequesters lipid-soluble local anesthetic molecules, reducing free drug available to target tissues ("scavenger" effect)
- Direct metabolic support: provides fatty acid substrate to bupivacaine-poisoned myocardial mitochondria (rescues oxidative phosphorylation)
- Direct positive inotropic effect: reverses LA-induced calcium channel blockade
- Redistribution: carries LA from cardiac/CNS tissue back to peripheral depots (liver, adipose)
Intralipid 20% must be immediately available wherever local anesthetics are used.
STEP 5 - CARDIOVASCULAR RESUSCITATION (Modified ACLS)
For hypotension / bradycardia (without arrest):
- Epinephrine: LOW DOSE - initial bolus <1 mcg/kg (NOT standard ACLS 1 mg bolus)
- Rationale: high-dose epinephrine triggers VF in a bupivacaine-poisoned heart by increasing automaticity in an already irritable myocardium
- Small doses (10-100 mcg) correct hypotension without precipitating VF
- Phenylephrine or vasopressin for pure vasodilation without arrhythmia
- Calcium gluconate for direct inotropic support
- IV fluid bolus for volume resuscitation
For ventricular arrhythmias:
- Amiodarone - drug of choice for ventricular arrhythmias in LAST
- AVOID the following (all worsen LAST):
- Vasopressin (worsens cardiac depression)
- Calcium channel blockers (worsen myocardial depression)
- Beta blockers (worsen bradycardia and myocardial depression)
- Local anesthetics as antiarrhythmics (lidocaine, mexiletine - obviously worsen Na+ channel blockade)
- Class 1 antiarrhythmics (flecainide, procainamide - Na+ channel blockers)
For cardiac arrest:
- Begin CPR immediately - standard BLS/ACLS
- Lipid emulsion simultaneously (do not delay)
- Defibrillation for VF: standard energy (200 J biphasic)
- Reduce epinephrine dose to <1 mcg/kg per bolus (avoid standard 1 mg doses)
- Prolonged resuscitation may be needed - LA-poisoned hearts can recover with time + lipid therapy
STEP 6 - ESCALATION: CARDIOPULMONARY BYPASS (ECMO)
- If cardiac instability persists despite lipid emulsion + modified ACLS
- Alert the nearest facility with CPB/ECMO capability immediately - this is time-critical
- CPB allows the heart time to recover as plasma LA concentrations fall through redistribution and metabolism
- Extracorporeal membrane oxygenation (ECMO) is increasingly preferred (venoarterial ECMO for CVS collapse)
- Historical case reports of survival after 1+ hour of resuscitation via CPB
STEP 7 - POST-RESUSCITATION MONITORING
- Monitor in ICU/HDU for minimum 2-6 hours after resolution of symptoms
- Extended monitoring (up to 12 hours) for patients with significant cardiovascular morbidity
- Repeat ECG, ABG, electrolytes, CXR
- Reassess neurological status
- Watch for delayed recurrence of LAST (LA redistribution from tissues)
Management Summary - ASRA Algorithm
LAST SUSPECTED?
│
▼
1. CALL FOR HELP + Stop further LA injection
│
▼
2. AIRWAY → 100% O2, prevent hypercarbia/acidosis
│
▼
3. SEIZURES? → Benzodiazepines (avoid phenytoin)
│
▼
4. ★ LIPID EMULSION 20% (Intralipid)
• Bolus: 1.5 mL/kg over 2-3 min
• Infusion: 0.25 mL/kg/min
• Repeat bolus + increase infusion if unstable
│
▼
5. CARDIOVASCULAR:
• Epinephrine <1 mcg/kg boluses (NOT 1 mg)
• Amiodarone for VT/VF
• AVOID: vasopressin, Ca-blockers, β-blockers, class 1 antiarrhythmics
• CPR if arrest
│
▼
6. ESCALATE → Alert CPB/ECMO facility
│
▼
7. MONITOR 2-6 hours post-resolution
Special Populations
Paediatric LAST
- Calculate doses STRICTLY by weight (mg/kg); children at higher risk from overdose errors
- Lipid emulsion dose same: 1.5 mL/kg bolus; no specific neonatal dosing guidelines exist, but wide dose ranges appear safe
- Neonates: reduced protein binding and hepatic metabolism = lower threshold for toxicity
Obstetric LAST
- Bupivacaine 0.75% is CONTRAINDICATED for epidural in obstetrics
- Pregnant women: increased cardiac output + reduced protein binding → faster absorption
- Fetal acidosis can trap LA in fetus ("ion trapping")
- Lipid emulsion safe in pregnancy
Elderly LAST
- Reduced hepatic blood flow and protein binding
- Decreased cardiac reserve
- Use lower doses; careful monitoring
What to Have Ready (Before Every Block)
- Resuscitation cart with defibrillator
- 20% lipid emulsion (Intralipid) 500 mL - immediately at hand
- IV access established
- Pulse oximetry, ECG monitoring
- Airway equipment (facemask, laryngoscope, ETT)
- Benzodiazepine drawn up or available
- Printed ASRA LAST checklist (cognitive aid)
Key Take-Home Points
- Early recognition is everything - CNS prodrome (tinnitus, metallic taste, circumoral numbness) precedes cardiac arrest by precious minutes
- Lipid emulsion (Intralipid 20%) is the antidote - give early and boldly
- Modified ACLS - epinephrine doses must be LOW (<1 mcg/kg); avoid vasopressin, beta-blockers, Ca-channel blockers, and Class 1 antiarrhythmics
- Bupivacaine is the most dangerous - can cause cardiac arrest without CNS warning, especially if sedation masks CNS signs
- Prolonged resuscitation is justified - LA-poisoned hearts can recover with time + lipid rescue; do not give up
- Prevention: aspiration, incremental injection, epinephrine test dose, ultrasound guidance, dose limits
- Ultrasound reduces but does not eliminate LAST - vigilance is always required
Sources: Barash Clinical Anesthesia 9e, Miller's Anesthesia 10e, Morgan & Mikhail's Clinical Anesthesiology 7e, Tintinalli's Emergency Medicine, Lippincott Pharmacology; ASRA 3rd Practice Advisory on LAST (Neal JM et al., Reg Anesth Pain Med 2018;43:113-123); On'Gele et al., Anesthesiol Clin 2024
This is a shared conversation. Sign in to Orris to start your own chat.