Tendon transfer principles indications types usages requisites disadvantages and outcomes explain everything in detail with appropriate illustrative images and diagrams
Reading File
Finding Sources
Finding Sources
Searching the Web
tendon transfer surgery principles indications requisites outcomes orthopedic
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from authoritative textbooks. Let me compile the complete, detailed answer.
Tendon Transfer: A Complete Guide
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Rockwood & Green's Fractures in Adults 10th Ed 2025; Miller's Review of Orthopaedics 9th Ed
1. DEFINITION
A tendon transfer involves detaching a functioning muscle-tendon unit from its normal insertion and redirecting it to a new attachment site to replace the function of a paralyzed, ruptured, or otherwise non-functional muscle. The procedure does not create new muscle power - it redirects existing power to where it is needed most.
2. INDICATIONS
Tendon transfers are indicated when:
- Peripheral nerve injuries - when nerve repair is not possible or has failed (radial nerve palsy, ulnar nerve palsy, median nerve palsy, brachial plexus injuries)
- Irreparable tendon ruptures - e.g., rotator cuff tears that cannot be directly repaired, rheumatoid arthritis-related tendon rupture (Vaughan-Jackson syndrome)
- Poliomyelitis - to restore function after motor paralysis
- Cerebral palsy - to correct dynamic muscle imbalance
- Spinal cord injuries - partial cord lesions with selective muscle preservation
- Congenital anomalies - muscle absence (e.g., Poland syndrome)
- Spastic conditions - stroke, traumatic brain injury causing muscle imbalance
- Leprosy - with resultant intrinsic muscle paralysis
- Spina bifida / myelomeningocele - to balance foot/ankle
- Scapular winging - failure of serratus anterior or trapezius
The key question is whether a nerve repair or direct tendon repair is still possible. Tendon transfer is typically reserved for cases where neural recovery is not expected or has not occurred after 12-18 months.
3. PREREQUISITES (REQUISITES)
These are the conditions that must be met before performing a tendon transfer. Failure to satisfy these prerequisites is a major cause of failure.
Campbell's Key Principles (the "Seven Pillars"):
| Prerequisite | Details |
|---|---|
| 1. Expendability | The donor muscle must be redundant - its transfer must not create a new significant deficit. If two or more muscles share a function, one can be donated. |
| 2. Strength (MRC Grade ≥4) | Transfer causes a loss of approximately one grade of strength. Therefore the donor muscle must be grade 4 (Good) or 5 (Normal) before transfer. A grade 3 donor will yield only grade 2 function after transfer - often insufficient. |
| 3. Soft-Tissue Equilibrium | The bed through which the tendon will glide must be pliable, well-vascularized, and free of scar. Scarred tissue prevents tendon gliding and leads to adhesion. Flap reconstruction or tissue replacement may be required before transfer. |
| 4. Supple Joints / Passive Range of Motion | All joints on which the transfer will act must have full (or near-full) passive range of motion. A transferred tendon cannot overcome a fixed joint contracture. Splinting, serial casting, capsular release, or osteotomy must precede transfer. |
| 5. Excursion/Amplitude | The donor tendon's amplitude of excursion should be sufficient for the target function. The wrist tendons have ~33 mm, while the FDP has ~70 mm (see diagram below). |
| 6. Integrity (One Function Rule) | A single transferred tendon should ideally perform only one function. Splitting it to two insertions reduces efficiency, as the muscle acts primarily on the slip under greatest tension. |
| 7. Synergy | Transfers between muscles that normally function together (e.g., wrist flexors firing during finger extension) are easier for the patient to re-educate and rehabilitate. |
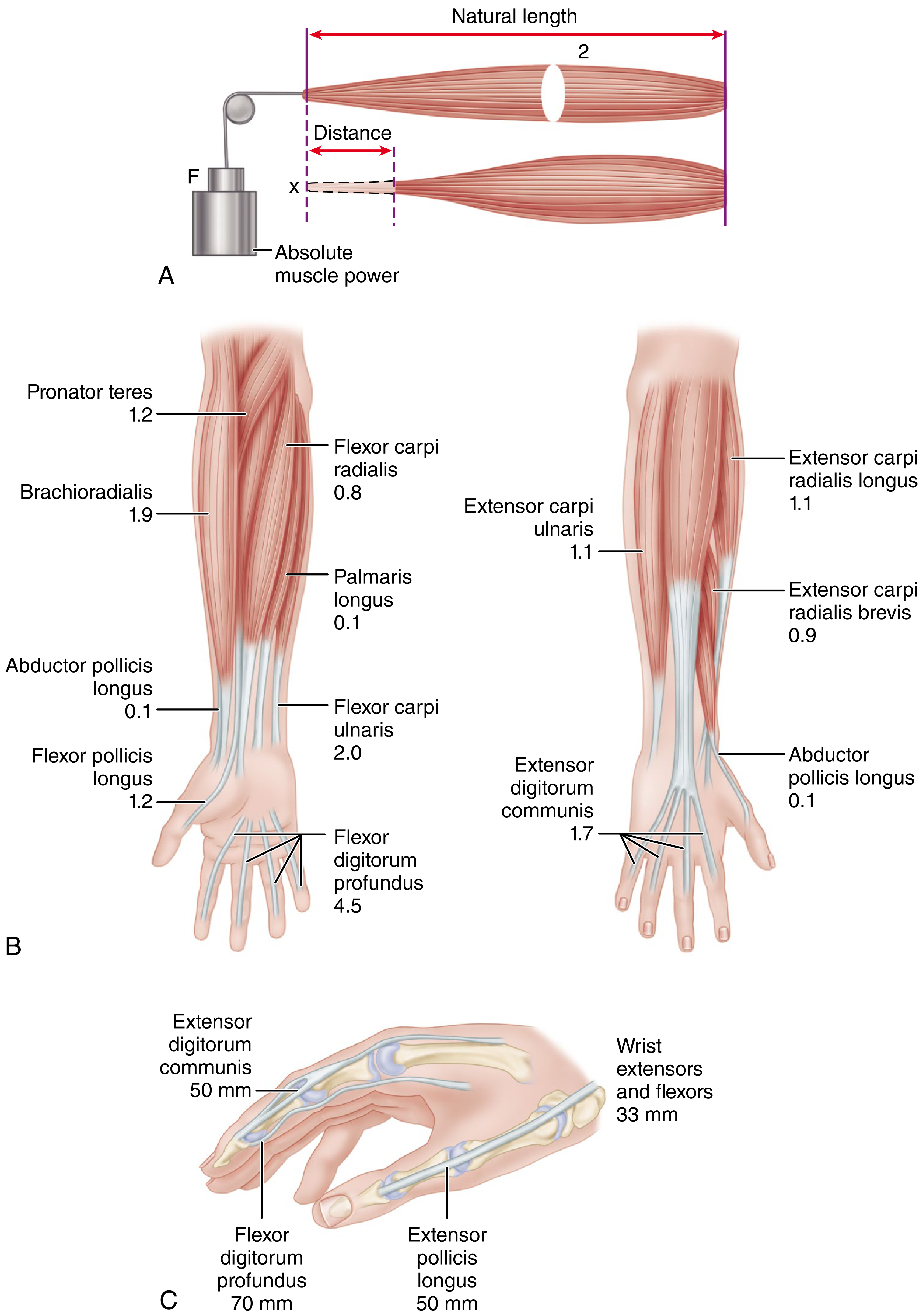
Amplitude of Excursion Reference Table (Curtis, 1974):
| Tendon | Amplitude |
|---|---|
| Wrist tendons | 33 mm |
| Extensor digitorum communis | 50 mm |
| Extensor pollicis longus | 58 mm |
| Flexor pollicis longus | 52 mm |
| Flexor sublimis | 64 mm |
| Flexor profundus | 70 mm |
4. TIMING OF TENDON TRANSFER
Timing is critical and must be individualized:
- Soft-tissue conditions: Transfer should not occur until scar tissue has matured and been replaced, or until a healthy soft-tissue bed (with fat) is available. Transferred tendons must be surrounded by fat to prevent adhesion to raw bone or subcutaneous scar.
- Passive joint motion: Must be restored before surgery - stiff joints cannot be corrected by transfer alone, and will cause the transferred tendon to adhere permanently.
- Bony alignment: Osteotomy and bone grafting must precede transfer.
- Sensory restoration: If sensory loss is present, procedures to restore sensibility should precede tendon transfer.
- Poliomyelitis: Wait at least 18 months post-acute phase before transfer, as recovery can continue for this duration. Any recovery after this is unlikely to exceed one grade.
- Nerve injury: Early "prophylactic" or "internal splint" transfers may be performed in some high-radial nerve injuries to maintain joint position while awaiting nerve recovery - these can be converted to permanent transfers if recovery fails.
5. PLANNING THE TENDON TRANSFER
The evaluation must define:
- Function lost - which muscles are paralyzed?
- Function retained - which muscles are working?
- Function possible - what reconstruction can achieve?
A useful approach is to list functions needed in one column and available donor muscles in another column (see diagram):

6. TECHNICAL CONSIDERATIONS
Intraoperative Assessment
- At surgery, the color of the donor muscle confirms suitability: a healthy donor is dark pink or red (indicating normal nutrition and muscle fibers). A pale pink, small muscle with reduced excursion at surgery is unsuitable.
- Muscles that do not contract with pinch or electrocautery stimulus are likely nonfunctional and should not be used.
Line of Pull
- The muscle-tendon unit must have as straight a line of action as possible between origin and new insertion. An acute angle reduces efficiency.
- If an angle is unavoidable, a pulley must be created (e.g., FCU loop in Bunnell opponensplasty), but friction at the pulley reduces efficiency.
Routing
- With few exceptions, transferred tendons should be routed subcutaneously. A tendon crossing raw bone, passing through tight fascia, or buried within scarred tissue will not glide and will form adhesions.
- When the tendon must cross fascia, the opening must be generously sized.
Tension at Suture
- If a muscle has been detached from its insertion for some time, it will develop a contracture; therefore anchor it under more tension than usual because it will stretch and regain some excursion postoperatively.
- A muscle that has been detached should be set with the wrist in neutral and the fingers/thumb in the desired functional position.
Fixation Technique
- Attachment is most commonly end-to-side (into the side of the recipient tendon) - important when there is a possibility of later nerve recovery restoring the original function.
- Weave or side-by-side suture techniques are preferred as they allow early mobilization.
- The attachment must be strong enough to withstand early rehabilitation forces.

7. TYPES AND SPECIFIC TRANSFERS
A. Upper Extremity
Radial Nerve / PIN Palsy
| Function to Restore | Donor (FROM) | Recipient (TO) |
|---|---|---|
| Wrist extension | Pronator teres (PT) | ECRB |
| Finger extension | FCU or FCR | EDC |
| Thumb extension | Palmaris longus (PL) or FDS | EPL |
- PT to ECRB is the gold standard for wrist extension restoration in radial nerve palsy.
- FCU to EDC is preferred by many surgeons as FCU is synergistic with finger extension.
Low Median Nerve Palsy (Opponensplasty)
The goal is to restore thumb opposition and abduction (lost when thenar intrinsics are paralyzed):
| Donor | Pulley/Route | Recipient |
|---|---|---|
| FDS ring finger (Bunnell's classic) | FCU loop at wrist | APB tendon |
| EIP | Around ulnar border of wrist | APB |
| Palmaris longus | FCR pulley | APB |
| ADM (Huber transfer) | None needed | APB (in children/congenital) |
High Median Nerve Palsy (adds FPL, FDP index/long)
- Brachioradialis (BR) to FPL for thumb IP flexion
- FDP index and middle fingers tethered side-to-side to the intact FDP of ring/little fingers (ulnar innervated)
Low Ulnar Nerve Palsy (claw deformity)
The ulnar two fingers develop intrinsic minus claw deformity (MP hyperextension, IP flexion):
| Function to Restore | Dynamic Procedure |
|---|---|
| Correct clawing (flex MPs, extend IPs) | FDS to lateral bands (Stiles-Bunnell); ECRL passed volar to transverse metacarpal ligament |
| Thumb adduction | FDS ring or ECRB to adductor pollicis |
| Index abduction | APL, ECRL, or EIP to 1st dorsal interosseous |
Shoulder: Irreparable Rotator Cuff Tears
- Latissimus dorsi transfer (Gerber technique): for irreparable posterosuperior cuff tears (supraspinatus + infraspinatus). Restores external rotation and abduction. Neurovascular pedicle must be preserved.
- Lower trapezius transfer: for external rotation deficit; rules - excursion and tension must match; one function per transfer.
- Pectoralis major transfer: for subscapularis replacement (anteroinferior cuff).
Scapular Winging
- Medial winging (serratus anterior palsy): split pectoralis major sternal head transfer to the inferior angle of the scapula.
- Lateral winging (trapezius palsy): modified Eden-Lange triple transfer (levator scapulae, rhomboid minor, rhomboid major moved laterally).
B. Lower Extremity
Foot Drop / Talipes Equinovarus (Poliomyelitis, CP)
- Anterior transfer of posterior tibial tendon (Barr procedure): through the interosseous membrane to the middle cuneiform. Removes varus deforming force and provides active dorsiflexion.
- Split posterior tibial tendon transfer (SPOTT): half to peroneus brevis insertion (cuboid) to balance varus without over-correcting to valgus. 78% poor results reported with full tendon transfer due to over-correction and calcaneus deformity. The split transfer acts as a dynamic sling balancing forces evenly across the foot.
Cerebral Palsy (Foot)
- Split transfers preferred over full transfers (lower complication rate).
- In CP foot-drop: split anterior tibial tendon transfer (SPLATT) to the peroneus brevis.
8. POSTOPERATIVE REHABILITATION
- Immobilization: Typically 3-4 weeks in a position that relaxes the transfer (protects the repair).
- Controlled mobilization: Begins after healing; the patient must learn to re-educate the transferred muscle to perform its new function.
- Synergistic transfers are easier to re-educate because the brain already fires the donor muscle in a pattern compatible with the new function.
- Non-synergistic transfers may require biofeedback, electrical stimulation, and intensive occupational therapy.
- Full functional recovery typically takes 3-12 months.
9. DISADVANTAGES AND LIMITATIONS
| Disadvantage | Details |
|---|---|
| Loss of donor function | Transfer always sacrifices the original function of the donor muscle. If donor selection is wrong, a new functional deficit is created. |
| Strength reduction | One MRC grade of strength is reliably lost after transfer. A grade 3 donor becomes grade 2 - often functionally inadequate. |
| Cannot overcome fixed deformity | A transferred tendon cannot stretch contracted capsule or joint structures. Joint releases or osteotomy must precede transfer. |
| Adhesion / tendon adherence | If soft-tissue bed is scarred or transfer crosses raw bone, the tendon adheres and loses excursion. |
| Amplitude mismatch | Transferred tendon with insufficient excursion gives limited range; using brachioradialis for finger flexion fails for this reason. |
| Re-education difficulty | Non-synergistic transfers require prolonged and intensive rehabilitation; some patients (especially with cognitive impairment or poor motivation) cannot achieve functional use. |
| Tendon rupture | The suture site or bone-tendon interface can fail, especially with early loading. In arthroscopic latissimus dorsi transfer, rupture occurred in 38% in one series. |
| Neurologic complications | Nerve injury during transfer: axillary and radial nerve injury in latissimus dorsi transfers; musculocutaneous nerve in pectoralis major transfers. |
| Wound complications | Infection and hematoma, especially when deltoid detachment or acromial osteotomy is required for shoulder transfers. |
| Overcorrection | Full tendon transfers (e.g., full posterior tibial tendon transfer to dorsum of foot) risk overcorrection and calcaneus deformity - now largely abandoned in favor of split transfers. |
| One-function limitation | Each transfer is designed for one function; restoring a complex multi-function loss requires multiple transfers, increasing operative burden. |
| Irreversibility | Transfer is difficult to reverse; the commitment to sacrifice the donor function is permanent. |
| Not a substitute for nerve repair | When nerve recovery is still possible, tendon transfer delays this window or may interfere. Nerve repair or grafting is preferred when feasible. |
10. OUTCOMES
General
- Results depend heavily on strict adherence to the prerequisites above.
- Patients can reliably expect approximately one MRC grade less than the donor's preoperative strength.
- When all prerequisites are met, tendon transfer provides durable, long-term functional improvement.
Upper Extremity
- Radial nerve palsy transfers (PT to ECRB; FCU to EDC): Generally excellent results - most patients regain functional wrist and finger extension. Grade 4 function commonly achieved.
- Opponensplasty for median nerve palsy: Good outcomes with FDS ring (Bunnell) or EIP transfer; patients regain opposition for pinch and precision grip.
- Ulnar claw correction: Dynamic transfers (FDS to lateral bands) provide better intrinsic function than static procedures (capsulodesis, tenodesis) but require more rehabilitation.
- Latissimus dorsi transfer for posterosuperior rotator cuff (Gerber): Satisfactory outcomes in pain relief and forward elevation in selected patients; external rotation gain is variable. EMG studies show the transferred latissimus functions synergistically in abduction/external rotation post-transfer.
Lower Extremity
- Split posterior tibial tendon transfer (CP): In one study of 37 transfers in 30 children (8-year follow-up): 30 excellent, 4 good, 3 poor results. Results did not deteriorate with time; most patients ambulatory without braces.
- Full posterior tibial tendon transfers: 78% poor results in one study - now largely abandoned.
Factors Predicting Success
- Strict donor selection (expendable, grade 4-5)
- Supple soft-tissue bed
- Full passive joint motion pre-operatively
- Synergistic transfer pair
- Motivated patient with good cognitive function (for re-education)
- Experienced rehabilitation team
11. SUMMARY TABLE
| Principle | Rule |
|---|---|
| Expendable donor | Must not create new major deficit |
| Donor strength | MRC 4 or 5 minimum |
| Soft-tissue equilibrium | Pliable, fat-containing bed; no scar |
| Passive ROM | Full before transfer |
| Amplitude | Match to function needed |
| One function | One transfer = one goal |
| Synergy | Same-phase transfers easier to retrain |
| Straight line of pull | Minimize pulley friction |
| Timing | After equilibrium; before contracture |
| Fixation | End-to-side weave; early mobilization |
Campbell's Operative Orthopaedics 15th Ed 2026, pp. 4307-4325 (Chapter 76); Rockwood & Green's Fractures in Adults 10th Ed 2025, p. 784; Miller's Review of Orthopaedics 9th Ed, p. 737
Wallerinan degeneration definition etiology process stages and outcomes explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
wallerian degeneration definition etiology stages process nerve regeneration mechanism
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have all the content and diagrams needed for a comprehensive response. Let me compile everything.
Wallerian Degeneration: A Complete Guide
Sources: Bradley & Daroff's Neurology in Clinical Practice; Adams & Victor's Principles of Neurology 12th Ed; Rockwood & Green's Fractures in Adults 10th Ed 2025; Bailey & Love's Short Practice of Surgery 28th Ed; Medical Physiology (Boron & Boulpaep); Neuroscience: Exploring the Brain 5th Ed; Histology: A Text and Atlas (Pawlina)
1. DEFINITION
Wallerian degeneration (WD) is an active, programmed process of anterograde (distal) degeneration of the portion of an axon that is separated from its cell body (soma) following nerve injury. It is named after the English physiologist Augustus Volney Waller, who first described it in 1850 after observing the degeneration of frog glossopharyngeal nerves he had sectioned.
The process involves:
- Fragmentation and dissolution of the axon distal to the injury site
- Breakdown of the myelin sheath into ovoids and debris
- Phagocytic clearance of debris by Schwann cells and macrophages
- A transition from degeneration to a regenerative environment
Although primarily an anterograde process, there is also a retrograde component affecting the proximal stump (back to the nearest node of Ranvier) and the cell body itself.
"The degeneration of axons that occurs when they are cut is now called Wallerian degeneration. Because it can be detected with certain staining methods, Wallerian degeneration was an early strategy used to trace axonal connections in the brain." - Neuroscience: Exploring the Brain, 5th Ed
2. FUNDAMENTAL BASIS: AXONAL TRANSPORT
To understand WD, one must understand axonal transport - the mechanism by which the soma maintains its distant axon:
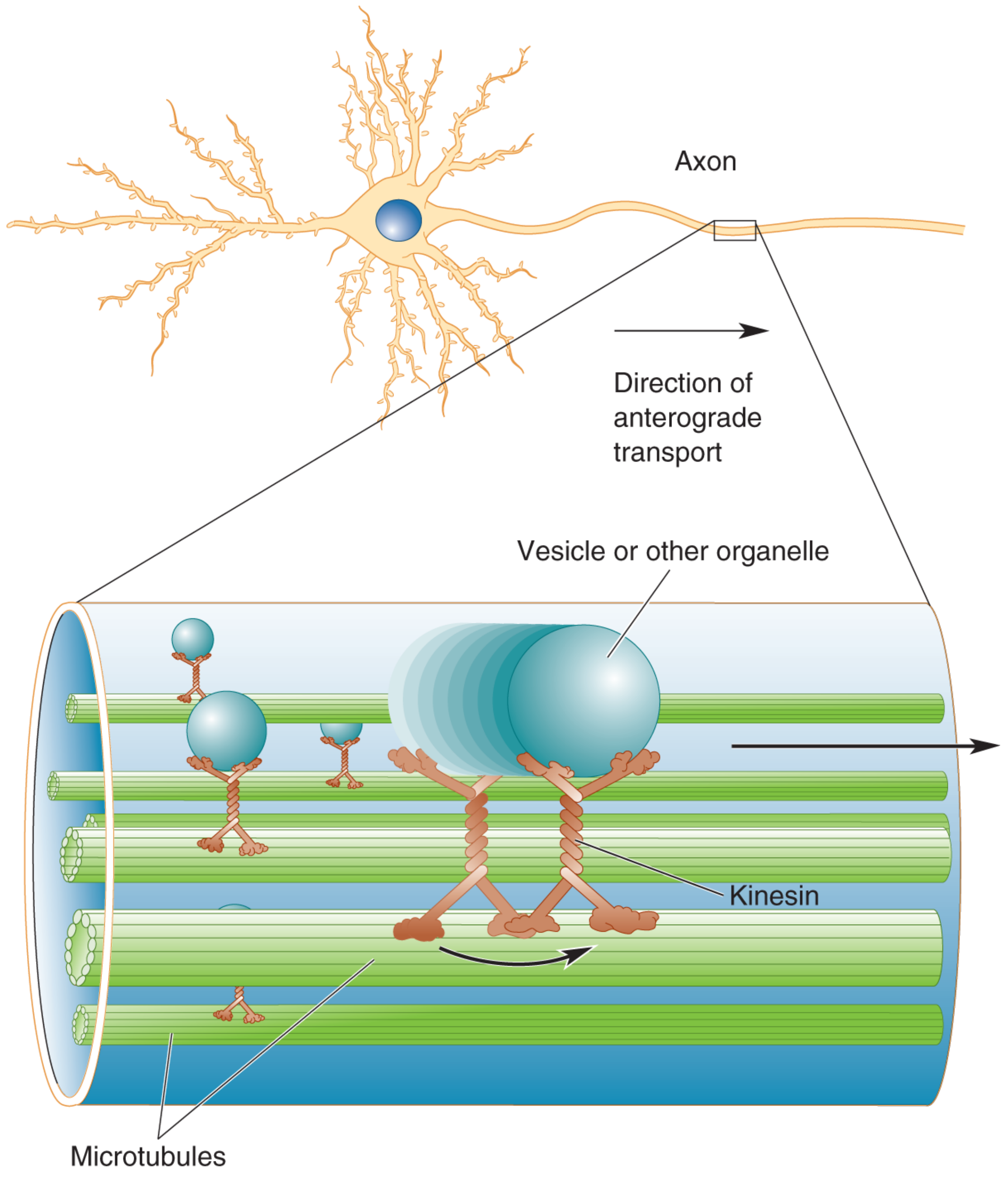
- Anterograde transport (soma → terminal): Carried by kinesin along microtubules at up to 1,000 mm/day (fast) or 1-10 mm/day (slow). Delivers organelles, vesicles, proteins, and membrane components.
- Retrograde transport (terminal → soma): Carried by dynein, providing feedback signals about metabolic needs of the terminal.
When the axon is severed, this bidirectional supply and signaling chain is broken. The distal segment is cut off from its trophic source and undergoes progressive dissolution.
3. ETIOLOGY - CAUSES
Wallerian degeneration occurs in any injury that disrupts axonal continuity. It does NOT occur in neurapraxia (grade I/Sunderland 1st degree) where only focal conduction block happens without axonal disruption. It occurs in:
| Nerve Injury Grade | Structure Disrupted | WD Occurs? |
|---|---|---|
| Neurapraxia (Seddon) / 1st degree (Sunderland) | Myelin only, axon intact | NO |
| Axonotmesis / 2nd degree | Axon disrupted, endoneurium intact | YES |
| Axonotmesis / 3rd degree | Axon + endoneurium disrupted, perineurium intact | YES |
| Neurotmesis / 4th degree | Axon + endo + perineurium, epineurium intact | YES |
| Neurotmesis / 5th degree | All layers including epineurium disrupted | YES |
Common causes:
- Trauma: laceration, crush, stretch/traction, avulsion, gunshot wound
- Compression: entrapment neuropathy (severe/chronic - e.g., carpal tunnel syndrome)
- Ischemia: nerve infarction (vasculitic neuropathy)
- Toxic/metabolic: severe axonal neuropathies (diabetic, alcoholic, chemotherapy-induced)
- Infections: leprosy, Lyme disease, HIV neuropathy
- Radiation injury
- Cold injury / electrical injury
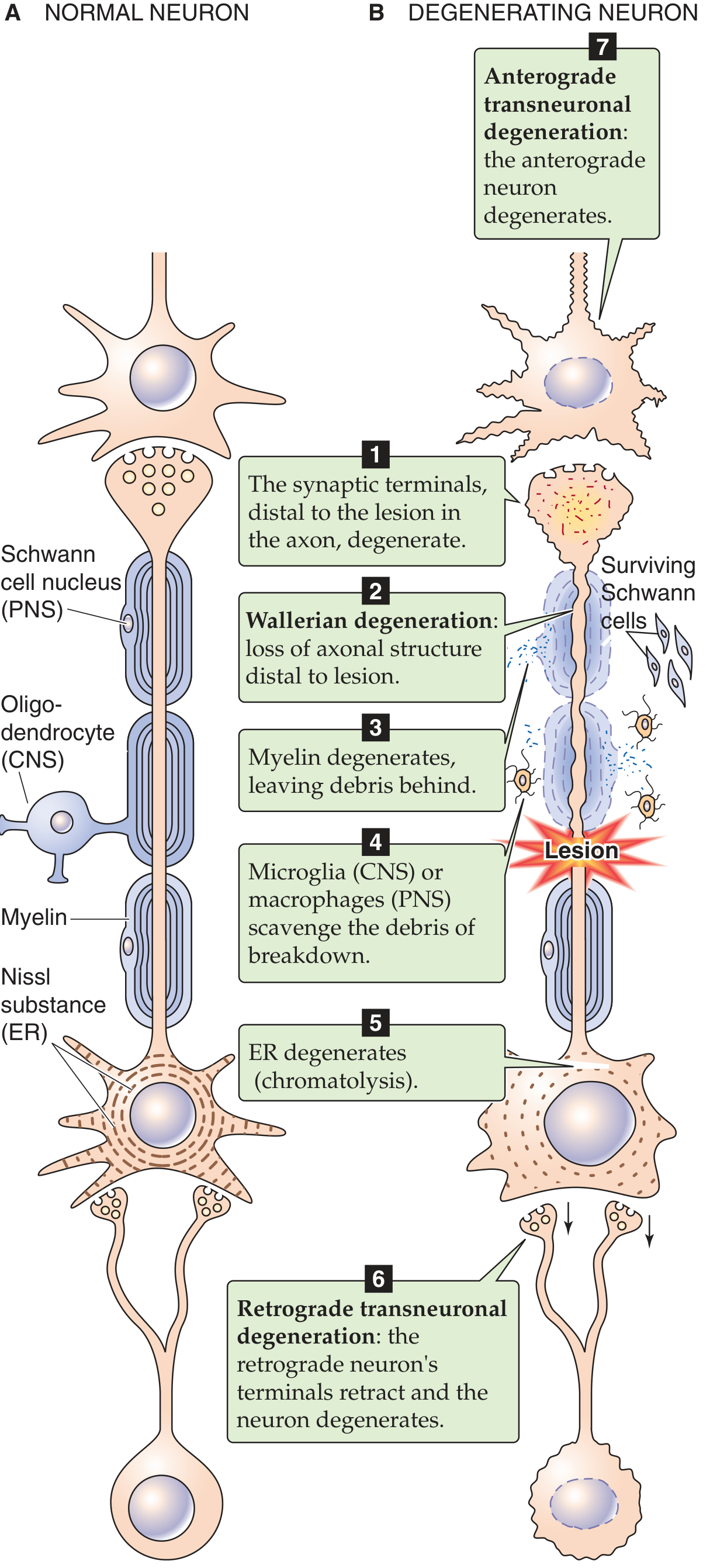
4. THE STAGES AND PROCESS OF WALLERIAN DEGENERATION
The complete sequence involves seven interconnected events, affecting the distal segment, the injury site, and the cell body.
Stage 1: Acute Axonal Changes (Minutes to Hours)
Within 30 minutes of injury:
- Separation of the proximal and distal ends
- Rapid influx of extracellular calcium and sodium through the disrupted axonal plasma membrane
- This calcium influx activates calcium-dependent proteases (calpains) - a cascade that shares features with programmed cell death (apoptosis)
- Axonal injury triggers recruitment of leukocytes and initiates a cytokine-mediated signaling cascade (TNF-α, IL-1α, IL-1β, IL-10)
- Synthesis of neurotrophins, chemokines, extracellular matrix molecules, and proteolytic enzymes begins
- The transected membranes are initially sealed
Stage 2: Axon Fragmentation - Distal Segment (Days 1-7)
This is "Wallerian degeneration" proper:
- By day 3: Schwann cells retract from the node of Ranvier
- The distal axon begins to swell, then fragment into irregular segments
- The axon breaks down into ovoids (digestion chambers of Cajal) - irregular membrane-bound packets of axoplasm and organelles
- The myelin sheath breaks into blocks and ovoids around these axonal fragments
- Myelin lamellae decompact and fragment into lipid droplets (neutral fats) and cholesterol esters
- The entire axonal degeneration process takes approximately 1 week
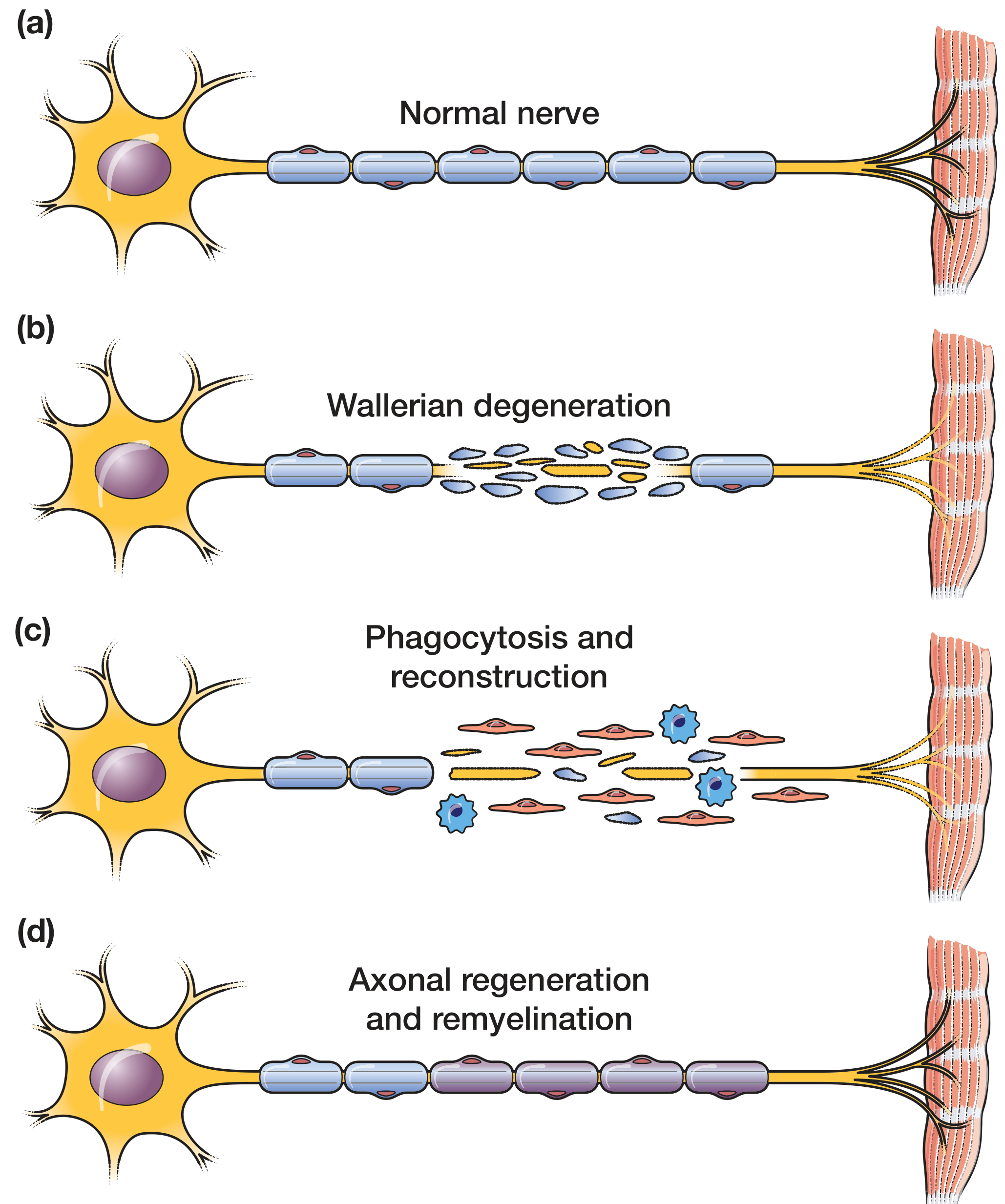
Stage 3: Myelin Degeneration
- The Schwann cell (the myelinating cell in the PNS) - unlike the axon - survives the process
- Schwann cells undergo a profound phenotypic switch from myelin-manufacturing cells to repair cells, driven by upregulation of c-Jun protein
- They begin to actively phagocytose their own myelin (myelinophagy) - taking up and degrading myelin debris
- The myelin breakdown products (neutral fats, cholesterol esters) are packaged for export
- In the CNS, oligodendrocytes and their myelin carry growth-inhibitory molecules (myelin-associated glycoprotein), which is one reason CNS regeneration is far less effective than PNS regeneration
Stage 4: Phagocytic Clearance (Days 3-14 and beyond)
- Activated Schwann cells and recruited macrophages (both tissue-resident endoneurial macrophages and circulating hematogenous macrophages entering via the leaky blood-nerve barrier) collaborate to phagocytose myelin ovoids and axonal debris
- Schwann cells handle early myelin clearance (the first 1-2 weeks); macrophages take over progressively from day 7 onwards
- Macrophages are guided by chemokines (MCP-1) secreted by Schwann cells
- This clearance is critical: axonal regeneration cannot begin until the endoneurial tubes are cleared of debris
- The cleared debris is carried via the bloodstream
- This process is much more rapid and efficient in the PNS than in the CNS (where microglia are slower), explaining the superior regeneration in the PNS
Stage 5: Chromatolysis - Cell Body Changes (Retrograde Reaction)
Simultaneously, the cell body (soma) undergoes a characteristic retrograde reaction:
- Chromatolysis: The rough endoplasmic reticulum (Nissl substance) breaks up, disperses, and migrates from the center to the periphery of the cell body
- The nucleus swells and moves to an eccentric (peripheral) position
- The cell body itself swells
- Increased expression of transcription factors switches gene expression from "axon maintenance" to "protein synthesis for regeneration" (growth-associated protein GAP-43, cytoskeletal proteins)
- This reflects the soma ramping up its metabolic machinery for axonal regrowth
- Chromatolysis begins within 1-2 days after injury and peaks at about 2 weeks
- Importantly: chromatolysis is reversible if the neuron survives and re-establishes its distal process
Regarding cell survival:
- After distal nerve transection, approximately 30% of primary sensory neurons die
- After proximal injury (e.g., avulsion), neuronal death is greater - some motor neurons and DRG neurons also die
- Very proximal injury (e.g., after proximal arm amputation) may lead to apoptosis of the cell body itself
Stage 6: Bands of Büngner Formation (Day 3 onwards)
This is the transition from degeneration to regeneration preparation:
- Schwann cells, having cleared myelin, now proliferate rapidly
- They elongate and align themselves within the intact endoneurial tube (basal lamina scaffolding)
- These aligned columns of Schwann cells form the bands of Büngner - cellular highways bounded by the original basal lamina
- The bands express adhesion molecules (cadherins, immunoglobulin superfamily, laminin) and neurotrophins (NGF, BDNF, NT-3, NT-4, GDNF, CNTF, IL-6)
- These molecular cues attract and guide regenerating axon sprouts from the proximal stump
- If reinnervation is delayed, Schwann cells atrophy, lose their pro-regenerative phenotype, and die - this begins by 2 months and becomes well-established thereafter
Stage 7: Transneuronal Degeneration (Variable)
- Retrograde transneuronal degeneration: Neurons that synaptically project onto the injured neuron (upstream neurons) may degenerate because they lose their postsynaptic target
- Anterograde transneuronal degeneration: Neurons that receive synapses from the injured neuron (downstream neurons) may degenerate because they are deprived of their presynaptic input
- The magnitude is variable and depends on the degree of dependence of connected neurons on trophic signals from the injured cell
5. DETAILED TIMELINE
| Time after injury | Event |
|---|---|
| Minutes | Calcium influx, membrane sealing, cytokine cascade begins |
| 24-30 hours | Axon fragmentation begins distally; axonal sprouts form from proximal stump |
| Day 3 | Schwann cells retract from nodes of Ranvier; early myelin phagocytosis begins |
| Days 3-7 | Macrophage recruitment; active debris clearance; chromatolysis peaks |
| Day 7 | Full Wallerian degeneration established in the distal segment |
| Days 7-21 | Bands of Büngner fully formed; endoneurial tubes cleared |
| Day 21+ | WD visible on electromyography (fibrillation potentials detectable) |
| Days 3-14 | Distal axon remains electrically excitable (important for electrodiagnosis) |
| 2 months | Schwann cell atrophy begins if not reinnervated |
| >12 months | Denervation atrophy of muscle becomes difficult to reverse |
| >24 months | Irreversible denervation atrophy of muscle |
"The distal axon takes some days to weeks to degenerate fully and may remain partially electrically active during this time. As a result, neurophysiology studies are not considered diagnostically reliable for some 3 to 6 weeks after proximal nerve injury." - Rockwood & Green's, 10th Ed
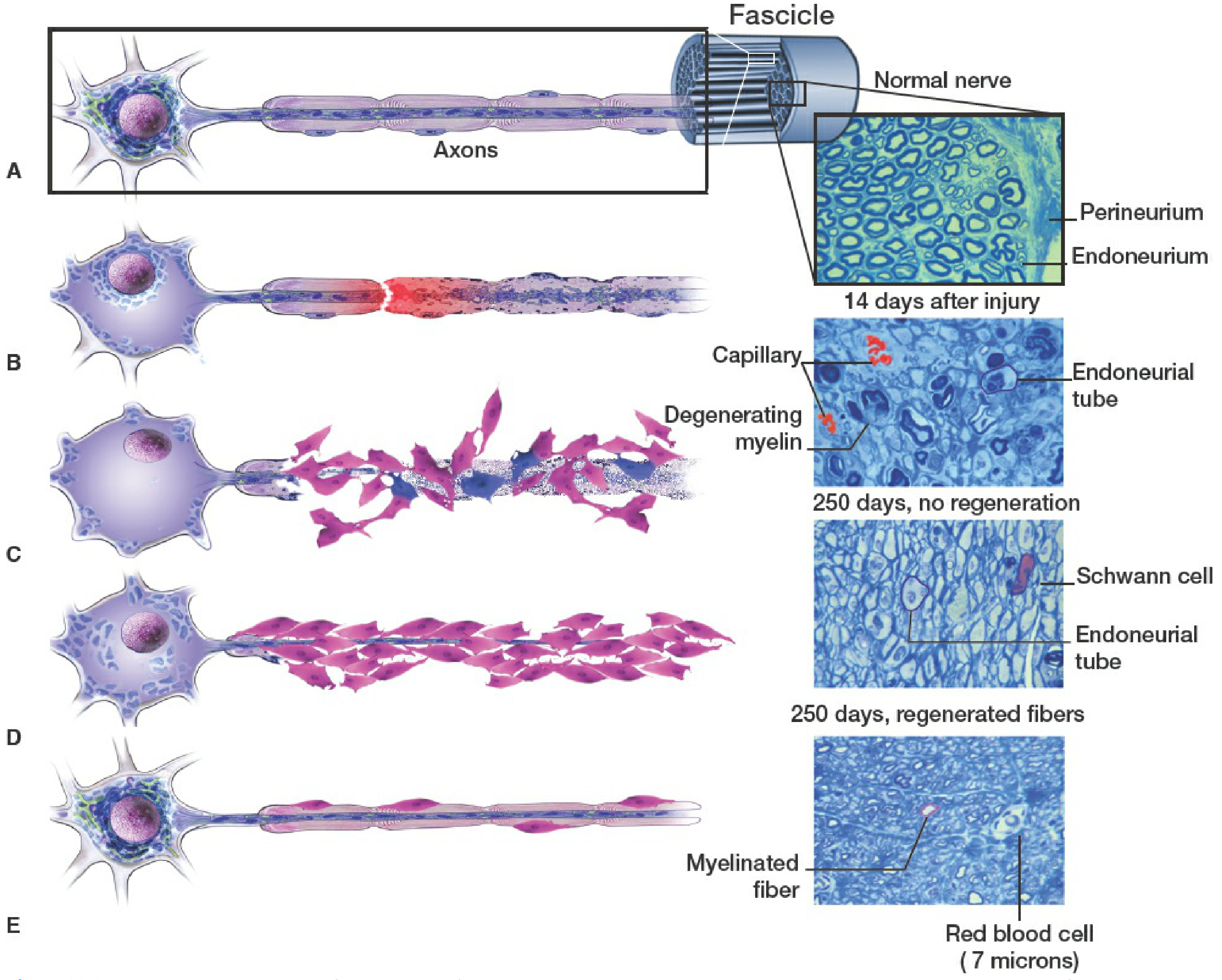
6. HISTOPATHOLOGY
The key histological appearances are:
- Digestion chambers (of Cajal): Ovoid membrane-bound structures containing fragmented axon and myelin debris
- Myelin ovoids: Spherical/oval lipid debris within endoneurial tubes, visible with osmium tetroxide staining
- Endoneurial tube collapse: Empty endoneurial tubes after debris clearance; at 250 days without regeneration, tubes are largely empty with residual Schwann cells
- Bands of Büngner: Parallel columns of Schwann cells within intact basal laminae visible on longitudinal section
- Regenerated fibers: Smaller diameter, shorter internodal segments, thinner myelin than original (visible on toluidine blue stained resin sections)
7. ELECTRODIAGNOSTIC CORRELATES
Understanding WD is essential for interpreting nerve conduction studies (NCS) and EMG:
- In the first 3-7 days after nerve injury: The distal nerve segment remains electrically excitable because WD is not yet complete. NCS may appear near-normal even in complete transection - this is a false-negative window
- After 7-21 days: WD is complete; the distal segment no longer conducts. NCS shows:
- Loss of CMAP (compound muscle action potential) amplitude
- Loss of SNAP (sensory nerve action potential) amplitude in sensory fibers
- After 21 days: EMG shows fibrillation potentials and positive sharp waves - spontaneous muscle fiber activity due to denervation supersensitivity to acetylcholine
- Fibrillation potentials are absent in neurapraxia (no WD, axon intact) - this distinguishes it from axonotmesis/neurotmesis
8. WD IN THE CNS VS. PNS
| Feature | PNS | CNS |
|---|---|---|
| Speed of myelin clearance | Rapid (days-weeks) | Slow (months-years) |
| Primary phagocytes | Schwann cells + macrophages | Microglia (slow) |
| Regeneration capacity | High (bands of Büngner guide axons) | Very low |
| Growth inhibitors | Absent (permissive environment) | Present (MAG, Nogo, OMgp on myelin) |
| Glial scar formation | Minimal | Prominent astrocytic scar - major barrier |
| Outcome | Functional recovery possible | Rarely meaningful recovery |
9. NERVE REGENERATION AFTER WD
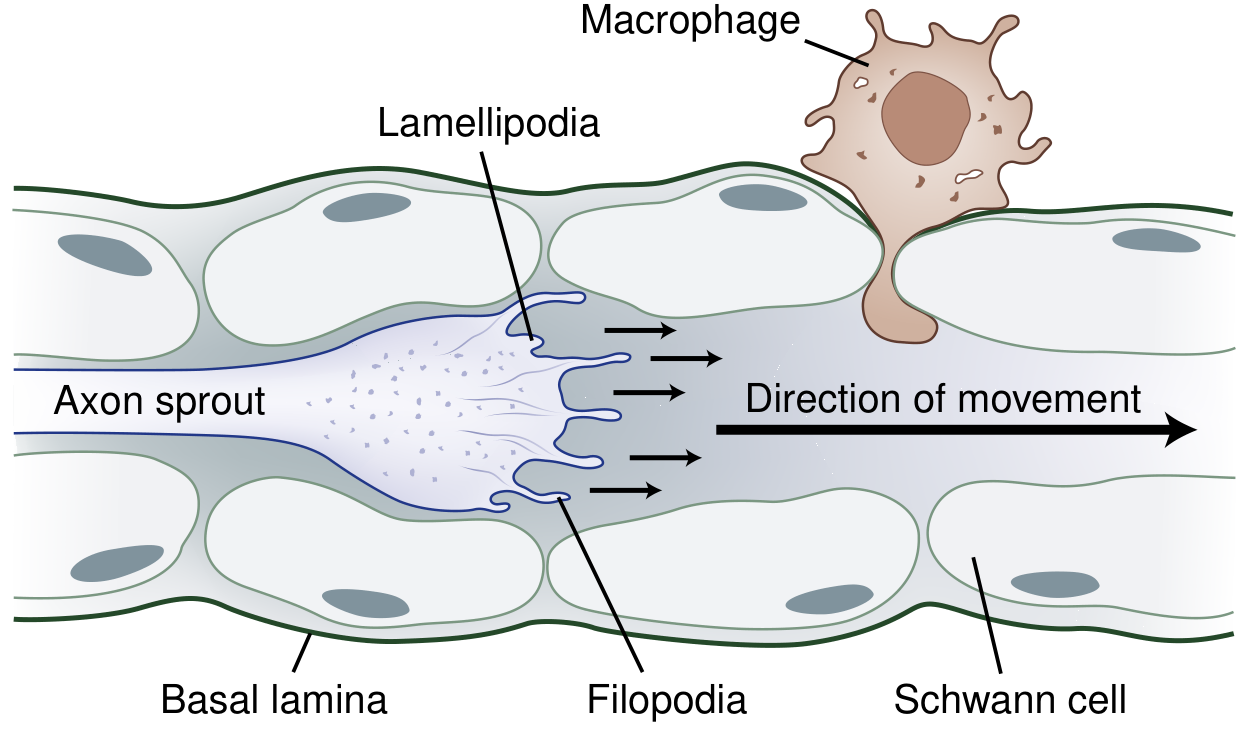
Once WD is complete and endoneurial tubes are cleared:
- Proximal stump activity: After a 2-3 week latency, neurites (sprouts) begin emerging from the proximal axon face. Multiple sprouts (up to 100 per axon) grow distally.
- Growth cone: The motile tip of each sprout bears lamellipodia (sheet-like projections) and filopodia (finger-like projections) rich in actin. These sense guidance molecules in the microenvironment.
- Neurotropism: Growth cone direction is guided by:
- Attractive signals: Neurotrophins (NGF, BDNF, NT-3, NT-4, GDNF), laminin, fibronectin in the bands of Büngner
- Repulsive signals: Semaphorins, ephrins, netrins, slits
- Plasminogen activators: Secreted by the growth cone to dissolve debris plugging endoneurial tubes
- Rate of regeneration: Approximately 1-2 mm/day (or ~1 inch/month). Proximal lesions regenerate faster (2-3 mm/day), distal lesions slower (~1 mm/day).
- Types of recovery:
- Collateral sprouting: Intact motor axons sprout to reinnervate denervated muscle fibers; begins within 4 days; clinically evident at 3-6 months
- Axon regeneration: Main mechanism from 6-24 months; requires crossing the repair site, traversing the distal stump, and reaching the target organ
Barriers to successful regeneration:
- ~50% of regenerating fibers fail to cross the repair site, forming a neuroma-in-continuity
- Mismatch of fiber type specificity (motor axon entering sensory endoneurial tube)
- Topographic misdirection (sensory axon to wrong cutaneous territory)
- Progressive Schwann cell atrophy with chronic denervation
- Endoneurial tube fibrosis and shrinkage with prolonged denervation
- Irreversible muscle fiber atrophy after ~24 months of denervation
10. OUTCOMES
| Nerve Injury Type | WD? | Expected Recovery |
|---|---|---|
| Neurapraxia | No | Full recovery in weeks to months (remyelination) |
| Axonotmesis (2nd degree) | Yes - endoneurium intact | Full recovery expected - axon regenerates along intact tube |
| Axonotmesis (3rd degree) | Yes - endo disrupted | Partial recovery - some misdirection |
| Axonotmesis (4th degree) | Yes - perineurium disrupted | Poor without surgery; neuroma-in-continuity |
| Neurotmesis (5th degree) | Yes - complete | No spontaneous recovery; surgery required |
Key prognostic factors:
- Proximal vs. distal injury: Proximal injuries have poorer outcomes - longer regeneration distance, greater likelihood of muscle atrophy before reinnervation
- Age: Younger patients regenerate more effectively
- Time to repair: Early repair (within 10-14 days) yields best results
- Tension-free repair: Critical - repair must be in a clean, well-vascularized bed without tension
- Muscle viability: Irreversible after 24 months of denervation
"Recovery is much slower with Wallerian or axonal degeneration, often requiring months to a year or more because the axon must first regenerate and then reinnervate the muscle, sensory organ, or blood vessel before function returns." - Adams & Victor's Principles of Neurology, 12th Ed
11. SUMMARY DIAGRAM OVERVIEW
| Stage | Location | Time | Key Event |
|---|---|---|---|
| 1 - Acute axonal injury | Injury site | Minutes | Ca²⁺ influx, proteases activated |
| 2 - Axon fragmentation | Distal segment | Day 1-7 | Axon breaks into ovoids |
| 3 - Myelin degeneration | Distal segment | Day 1-7 | Myelin breaks into lipid droplets |
| 4 - Phagocytic clearance | Distal segment | Day 3-14+ | Schwann cells + macrophages clear debris |
| 5 - Chromatolysis | Cell body | Day 1-14 | Nissl substance disperses, nucleus eccentric |
| 6 - Bands of Büngner | Distal endoneurial tubes | Day 3+ | Schwann cell columns form regeneration highway |
| 7 - Transneuronal degeneration | Connected neurons | Variable | Up- and downstream neurons affected |
| 8 - Axonal sprouting | Proximal stump | 2-3 weeks+ | Growth cones advance at 1-2 mm/day |
| 9 - Remyelination | Regenerated axon | Months | New myelin - shorter internodes, thinner sheath |
Sources: Bradley & Daroff's Neurology in Clinical Practice, p.1163-1200; Adams & Victor's Principles of Neurology 12th Ed, p.1675-1686; Rockwood & Green's Fractures in Adults 10th Ed, pp.766-784; Bailey & Love's 28th Ed, p.48; Medical Physiology, Boron & Boulpaep, pp.414-415; Neuroscience: Exploring the Brain 5th Ed, pp.206-208
This is a shared conversation. Sign in to Orris to start your own chat.