Protein Metabolism
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the essential content and diagrams needed for a comprehensive answer on Protein Metabolism. Let me compose the full response.
Protein Metabolism
Sources: Guyton and Hall Textbook of Medical Physiology; Lippincott Illustrated Reviews: Biochemistry, 8th ed; Schwartz's Principles of Surgery, 11th ed
1. Proteins and Amino Acids - The Building Blocks
Proteins are large molecules built from amino acids joined by peptide linkages. A carboxyl group of one amino acid combines with the amino group of another, releasing water to form the peptide bond. Most proteins contain 400 or more amino acids on average, and some chains coil into helices or fold into sheets held by hydrogen bonding and other non-covalent forces.
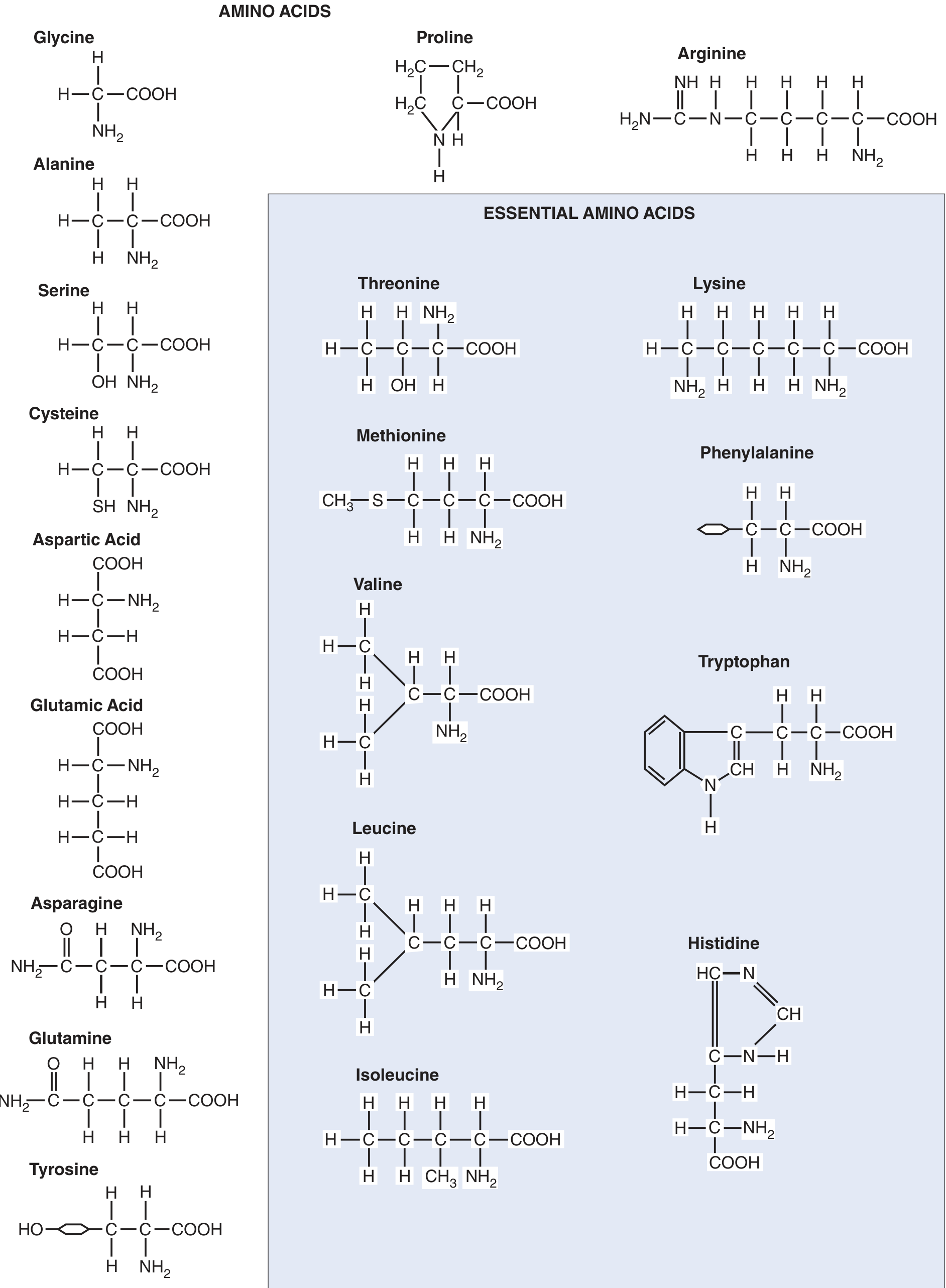
Essential vs. Non-essential Amino Acids
- 11 non-essential amino acids can be synthesized in the liver from appropriate α-keto acid precursors
- 9 essential amino acids cannot be synthesized in adequate quantities and must be obtained from diet: Threonine, Lysine, Methionine, Phenylalanine, Valine, Tryptophan, Leucine, Isoleucine, Histidine
The mnemonic PVT TIM HaLL (Phenylalanine, Valine, Tryptophan, Threonine, Isoleucine, Methionine, Histidine, Arginine*, Leucine, Lysine) is commonly used. *Arginine is conditionally essential.
2. Digestion and Absorption
Proteins from the GI tract are almost entirely absorbed as free amino acids; polypeptides and whole proteins are only rarely absorbed. After a meal, blood amino acid concentration rises only a few mg/dL above the normal range of 35-65 mg/dL, because:
- Digestion and absorption are extended over 2-3 hours
- Absorbed amino acids are taken up by cells within 5-10 minutes
Amino acids enter cells via active transport and facilitated transport using carrier mechanisms (too large for simple diffusion). In the kidney, filtered amino acids are reabsorbed in the proximal tubule - if plasma concentration exceeds the renal threshold, excess is lost in urine (aminoaciduria).
3. Storage and Equilibrium
Amino acids are not stored as free amino acids inside cells. Instead, they are incorporated into intracellular proteins via mRNA-directed ribosomal synthesis. These proteins can be rapidly re-hydrolyzed by lysosomal enzymes and released back into the blood.
A constant state of reversible equilibrium exists among:
- Plasma amino acids
- Tissue cell proteins
- Plasma proteins
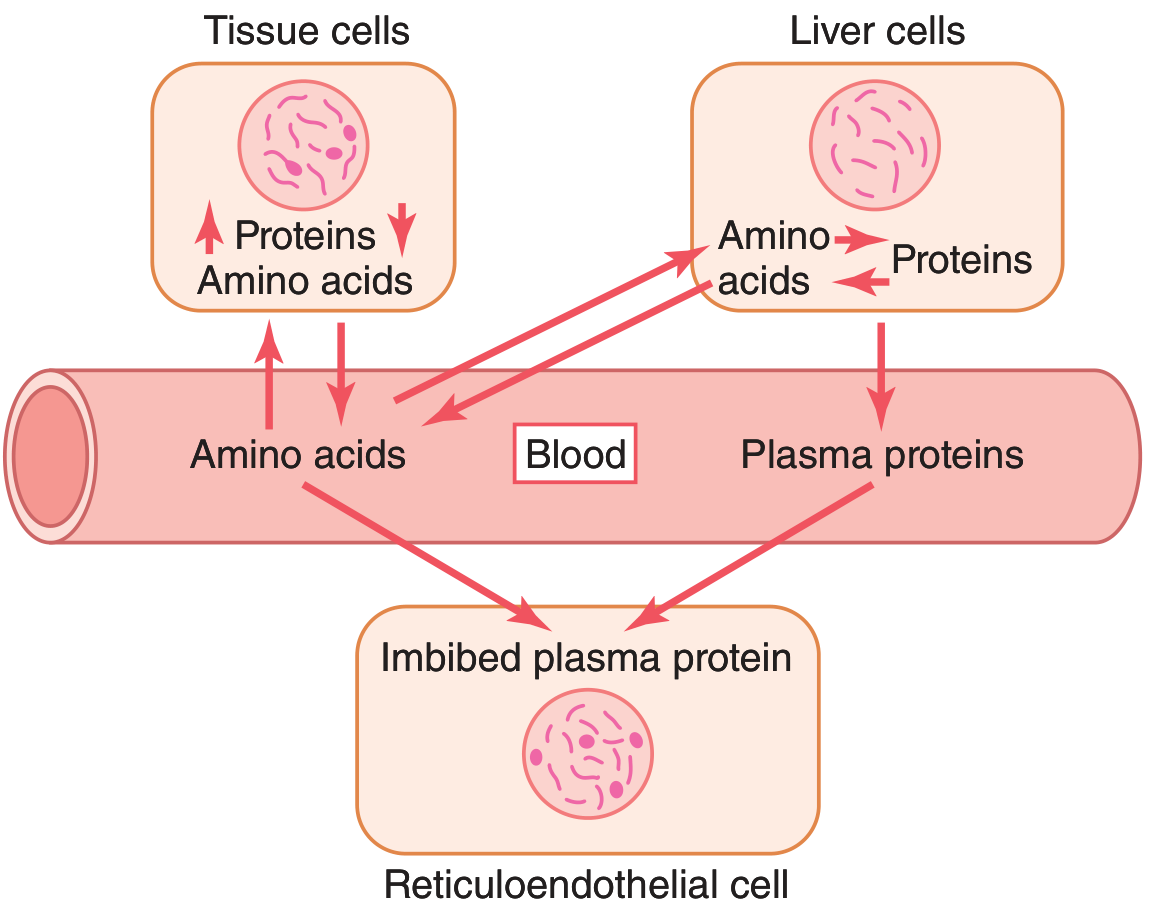
About 400 grams of body protein are synthesized and degraded each day as part of this continual flux. Even in starvation or disease, the ratio of tissue proteins to plasma proteins remains relatively constant at ~33:1.
- Guyton and Hall, p. 855
The liver, kidneys, and intestinal mucosa are the primary sites of rapid protein exchange. Structural proteins (collagen, muscle contractile proteins, chromosomal proteins) do NOT normally participate in this reversible exchange.
4. Protein Synthesis
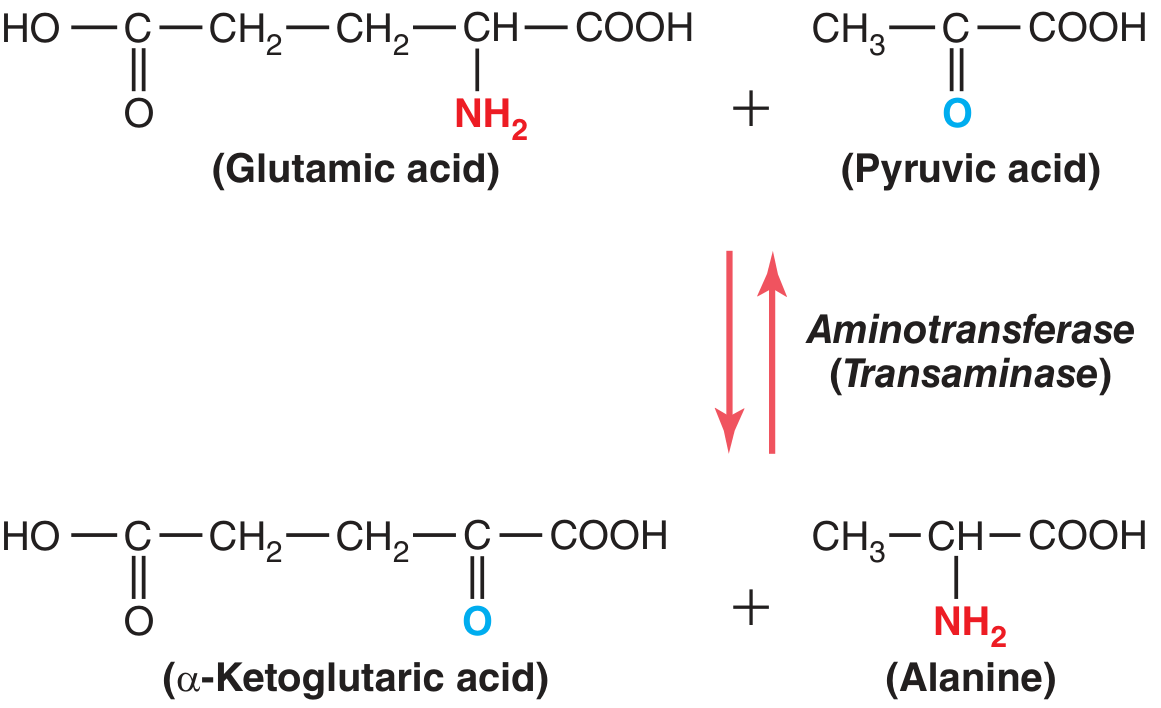
Cellular protein synthesis proceeds under the direction of mRNA and ribosomes. Non-essential amino acids are synthesized by transamination: an α-keto acid precursor is formed, and an amino group is transferred from a donor amino acid to that keto acid via aminotransferase enzymes (which require pyridoxine/Vitamin B6 as a cofactor).
Example: Synthesis of Alanine from Pyruvic Acid
- Glutamine acts as a major amino radical storehouse in tissues
- Amino radicals can also be donated from asparagine and aspartic acid
5. Protein Catabolism
5a. Deamination
When cells reach their storage limits for protein, or when energy is needed, amino acids are degraded - predominantly in the liver - beginning with deamination (removal of the amino group).
Most deamination occurs via transamination:
- The amino group is transferred to α-ketoglutaric acid, converting it to glutamic acid
- Glutamic acid can then transfer the amino group elsewhere or release it as ammonia (NH₃)
5b. Urea Cycle (Ornithine Cycle)
Ammonia released from deamination is highly toxic. The liver converts it to urea for safe excretion:
2NH₃ + CO₂ → H₂N-CO-NH₂ (urea) + H₂O
The urea cycle proceeds through the intermediates:
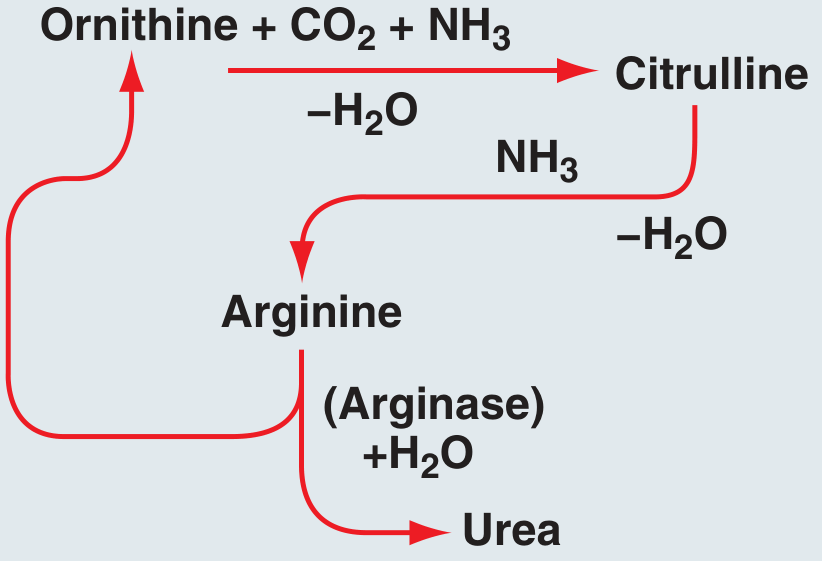
- Urea is formed exclusively in the liver
- If the liver fails or blood bypasses it (portal-caval shunt), plasma ammonia rises - causing hepatic coma
- The liver also synthesizes ~90% of all plasma proteins (max rate: 15-50 g/day); gamma globulins are the exception (formed by plasma cells in lymphoid tissue)
5c. Fate of the Carbon Skeleton
After deamination, the resulting keto acids can be:
- Converted to acetyl CoA or pyruvate → enter the TCA cycle for energy
- Used in gluconeogenesis (amino acids that yield glucose precursors are glucogenic - 18 of 20)
- Converted to fatty acids or ketone bodies (amino acids yielding acetyl CoA/acetoacetate are ketogenic - 19 of 20 can be converted to fatty acids)
6. The Liver's Central Role
The liver's contributions to protein metabolism are so critical that life cannot be sustained for more than a few days without them:
| Function | Details |
|---|---|
| Deamination | Primary site; small amounts in kidney |
| Urea synthesis | Removes toxic ammonia |
| Plasma protein synthesis | Albumin, clotting factors, transport proteins (~90% of total) |
| Transamination | Synthesis of non-essential amino acids |
| Gluconeogenesis | Amino acids → glucose during fasting |
Failure of plasma protein synthesis (as in cirrhosis) causes hypoalbuminemia → generalized edema and ascites due to loss of oncotic pressure.
7. Hormonal Regulation
| Hormone | Effect on Protein Metabolism |
|---|---|
| Growth Hormone | Increases cellular protein synthesis (↑ amino acid transport, ↑ DNA/RNA transcription/translation, ↓ protein oxidation) |
| Insulin | Necessary for protein synthesis; ↑ amino acid uptake into cells, ↓ protein degradation, ↓ need for amino acids as energy |
| Glucocorticoids | ↑ Breakdown of most tissue proteins; ↑ plasma amino acids; mobilize amino acids for gluconeogenesis |
| Testosterone | Causes protein deposition (anabolic effect) in tissues |
| Thyroid Hormone | Small amounts increase protein synthesis; large amounts increase catabolism; overall anabolic in physiologic doses |
8. Branched-Chain Amino Acids (BCAAs)
The BCAAs - Leucine, Isoleucine, Valine - are unique in that the liver has limited capacity to initiate their degradation. They pass through the liver essentially unchanged and are primarily metabolized in muscle. During fasting, BCAAs from muscle catabolism produce alanine and glutamine, which are released for hepatic gluconeogenesis.
- Alanine and glutamine are the quantitatively most important glucogenic amino acids from muscle
- This pathway is the glucose-alanine cycle: liver makes glucose → muscle uses it → releases alanine → liver converts alanine back to glucose
- (Lippincott Biochemistry, p. 926)
9. Protein Requirements and Nitrogen Balance
| Parameter | Value |
|---|---|
| Normal protein intake | 80-120 g/day |
| Energy yield | ~4 kcal/g protein |
| Nitrogen content | 1 g N per 6 g protein |
| Minimum daily requirement | 30-40 g/day (obligatory protein loss) |
| RDA (sedentary adult) | ~0.8 g/kg/day (≈60 g/day for 75 kg adult) |
Nitrogen balance is the key clinical indicator:
- Positive N balance = protein synthesis > breakdown (growth, recovery, pregnancy)
- Negative N balance = breakdown > synthesis (starvation, trauma, infection, burns)
After major injury, urinary nitrogen excretion can exceed 30 g/day, corresponding to ~1.5% lean body mass loss per day. Activation of the ubiquitin-proteasome system in muscle cells is a primary pathway for this accelerated protein degradation, worsened by hypoxia, acidosis, insulin resistance, and elevated glucocorticoids.
- Schwartz's Principles of Surgery, p. 93
10. Protein Metabolism in Fasting and Starvation
| State | Response |
|---|---|
| Well-fed (absorptive) | Amino acids used for protein synthesis; surplus deaminated and converted to fat or energy |
| Short-term fasting | Rapid muscle proteolysis (driven by ↓ insulin, ↑ glucocorticoids); amino acids → hepatic gluconeogenesis |
| Prolonged fasting (>2 weeks) | Rate of proteolysis decreases as brain shifts to using ketone bodies, sparing muscle protein |
| Starvation | Up to 125 g/day protein degradation; rapid cellular function deterioration |
Carbohydrates and fats are "protein sparers" - they are preferentially used for energy when available, protecting protein from oxidation.
Summary Flowchart
Dietary Protein
↓ (GI digestion)
Amino Acids (blood: 35-65 mg/dL)
↓
Tissue Uptake (active transport)
├── Protein Synthesis (ribosomes, mRNA)
├── Transamination → non-essential AA synthesis
└── Catabolism (when cells saturated or energy needed)
↓ Deamination (liver)
NH₃ → Urea Cycle → Urea (excreted by kidneys)
Carbon skeleton
├── Glucogenic AAs → Pyruvate/OAA → Gluconeogenesis
├── Ketogenic AAs → Acetyl CoA → TCA / Ketone bodies
└── Oxidation for ATP
Key Clinical Points:
- Deficiency of Vitamin B6 impairs transamination → poor amino acid synthesis and protein formation
- Loss of liver function → hyperammonemia → encephalopathy
- Hypoalbuminemia (chronic liver disease, malnutrition) → edema, ascites
- Excess protein intake beyond cell storage capacity → converted to fat (stored in adipose) or glycogen
This is a shared conversation. Sign in to Orris to start your own chat.