Give mechanism of action of specific iv antibiotics with theri coverage
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from Katzung's 16th Edition. Let me compile the full, detailed answer on IV antibiotic mechanisms and coverage.
IV Antibiotics: Mechanism of Action and Coverage
Source: Katzung's Basic and Clinical Pharmacology, 16th Ed; Jawetz Medical Microbiology 28th Ed; Harrison's Principles of Internal Medicine 22E
1. BETA-LACTAMS
Mechanism of Action
Beta-lactams (penicillins, cephalosporins, carbapenems, monobactams) work by binding to penicillin-binding proteins (PBPs) - transpeptidase enzymes on the bacterial cell membrane. This inhibits the transpeptidation step of peptidoglycan cross-linking, halting cell wall synthesis. Without a complete cell wall, bacteria undergo osmotic lysis. They are bactericidal and require actively dividing bacteria for full effect.
Beta-lactams bind the transpeptidase at the PBP site, resulting in inhibition of transpeptidation, thus halting peptidoglycan synthesis. - Katzung 16th Ed
A. Penicillins (IV)
| Agent | Spectrum / Coverage |
|---|---|
| Penicillin G (IV) | Streptococci (Group A, B, viridans), Streptococcus pneumoniae (sensitive strains), Neisseria meningitidis, Treponema pallidum, Clostridium (not difficile), Actinomyces |
| Ampicillin (IV) | Extends to Enterococci, Listeria monocytogenes, H. influenzae (non-beta-lactamase), E. coli, Proteus mirabilis |
| Ampicillin-sulbactam (IV) | Above + beta-lactamase producing organisms, MSSA, Bacteroides |
| Piperacillin-tazobactam (IV) | Broadest: Pseudomonas aeruginosa, Enterobacterales, anaerobes, MSSA; NOT MRSA |
| Nafcillin / Oxacillin (IV) | MSSA primarily (anti-staphylococcal) |
B. Cephalosporins (IV)
| Generation | Agents | Coverage |
|---|---|---|
| 1st gen | Cefazolin | MSSA, streptococci, limited gram-negatives (E. coli, Klebsiella, Proteus). Surgical prophylaxis. |
| 2nd gen | Cefuroxime, Cefoxitin, Cefotetan | Expanded gram-negatives; Cefoxitin/Cefotetan also cover anaerobes (Bacteroides) |
| 3rd gen | Ceftriaxone, Cefotaxime, Ceftazidime | Broad gram-negative including H. influenzae, Neisseria, Enterobacterales, S. pneumoniae; Ceftazidime covers Pseudomonas |
| 4th gen | Cefepime | Extended gram-negative including Pseudomonas + better gram-positive (pneumococci, streptococci); stable to many beta-lactamases |
| 5th gen | Ceftaroline | MRSA + broad gram-negatives (NOT Pseudomonas) |
| Novel | Ceftolozane-tazobactam, Ceftazidime-avibactam | MDR and carbapenem-resistant Pseudomonas, ESBL/KPC-producing organisms |
C. Carbapenems (IV)
| Agent | Coverage |
|---|---|
| Imipenem-cilastatin | Broadest spectrum: most gram-negatives (including Pseudomonas), gram-positives, anaerobes. Resistant to most beta-lactamases but not carbapenemases (KPC, MBL). NOT: MRSA, VRE, C. difficile, Stenotrophomonas. Requires cilastatin to prevent renal dehydropeptidase degradation. |
| Meropenem | Similar to imipenem; slightly better gram-negative activity, not degraded by dehydropeptidase. Used for meningitis (better CNS penetration). |
| Ertapenem | NO Pseudomonas, NO Acinetobacter. Good for ESBL-producing Enterobacterales, community-acquired infections, once-daily dosing. |
| Meropenem-vaborbactam | Adds coverage against KPC-producing carbapenem-resistant Enterobacterales (CRE). |
The carbapenems are resistant to most beta-lactamases but not serine carbapenemases nor metallo-beta-lactamases. - Katzung 16th Ed
D. Monobactams (IV)
| Agent | Coverage |
|---|---|
| Aztreonam | Gram-negatives ONLY (including Pseudomonas). No gram-positive or anaerobic activity. Safe in penicillin allergy (no cross-reactivity except with ceftazidime). |
2. GLYCOPEPTIDES (IV)
Mechanism of Action
Vancomycin binds firmly to the D-Ala-D-Ala terminus of nascent peptidoglycan pentapeptide chains. This inhibits transglycosylase, preventing further elongation of peptidoglycan and ultimately inhibiting cell wall synthesis. It acts at a different step than beta-lactams (earlier - before transpeptidation), explaining why there is no cross-resistance. It is bactericidal against staphylococci and bacteriostatic against enterococci.
Vancomycin inhibits cell wall synthesis by binding firmly to the d-Ala-d-Ala terminus of nascent peptidoglycan pentapeptide - Katzung 16th Ed
| Agent | Coverage |
|---|---|
| Vancomycin (IV) | MRSA (drug of choice), MSSA, S. epidermidis, Streptococci, Enterococci (not VRE). For penicillin-allergic patients with serious gram-positive infections. C. difficile (oral form only for GI). |
| Teicoplanin (IV/IM) | Similar to vancomycin; MRSA, staphylococci, streptococci, enterococci. |
3. AMINOGLYCOSIDES (IV)
Mechanism of Action
Aminoglycosides have a two-step mechanism:
- They are taken up across the bacterial cell membrane via an energy-dependent process (requires aerobic respiration - hence inactive against anaerobes and in anaerobic/acidic environments).
- Inside, they bind to the 30S ribosomal subunit (specifically protein S12 in the case of streptomycin, multiple sites for newer aminoglycosides), causing misreading of mRNA codons - leading to incorporation of wrong amino acids and production of aberrant, non-functional proteins. These abnormal proteins insert into the cell membrane, increasing permeability and allowing more aminoglycoside entry - a self-amplifying process.
They are concentration-dependent bactericidal antibiotics.
The aminoglycoside blocks the normal activity of the "initiation complex" of peptide formation and binds to protein S12 on the 30S subunit - Jawetz Medical Microbiology 28th Ed
| Agent | Coverage |
|---|---|
| Gentamicin | Gram-negatives: Enterobacterales (E. coli, Klebsiella, Proteus, Serratia), Pseudomonas. Synergy with beta-lactams for gram-positives (Enterococcus, Staphylococcus, viridans streptococci in endocarditis). |
| Tobramycin | Similar to gentamicin; better Pseudomonas activity |
| Amikacin | Broadest: resistant to most inactivating enzymes; MDR gram-negatives, Mycobacteria (M. avium complex) |
| Streptomycin | Mycobacterium tuberculosis, plague (Y. pestis), tularemia, synergy in endocarditis |
Inactive against: Strict anaerobes, Streptococcus pneumoniae alone (need synergy).
4. FLUOROQUINOLONES (IV)
Mechanism of Action
Fluoroquinolones inhibit two bacterial enzymes critical for DNA replication and repair:
- DNA gyrase (topoisomerase II) - primary target in gram-negative bacteria. Introduces negative supercoils ahead of the replication fork.
- Topoisomerase IV - primary target in gram-positive bacteria. Required for decatenation (separation) of daughter chromosomes after replication.
By blocking these enzymes, fluoroquinolones cause ds-DNA strand breaks and are bactericidal. They are concentration-dependent killers.
| Agent | Coverage |
|---|---|
| Ciprofloxacin (IV) | Excellent gram-negatives: Pseudomonas, Enterobacterales, H. influenzae, Neisseria, Legionella. Moderate gram-positives. Atypicals (Chlamydia, Mycoplasma). NOT reliable for streptococci/pneumococci. |
| Levofloxacin (IV) | "Respiratory quinolone" - all of ciprofloxacin's gram-negative coverage PLUS excellent S. pneumoniae, atypicals (Legionella, Mycoplasma, Chlamydia), Mycobacteria. |
| Moxifloxacin (IV) | Best gram-positive and anaerobic coverage. Excellent for respiratory pathogens, atypicals, anaerobes (intra-abdominal). Less Pseudomonas activity than ciprofloxacin. |
5. LINCOSAMIDES & STREPTOGRAMINS (IV)
Mechanism of Action
Clindamycin and quinupristin-dalfopristin bind the 50S ribosomal subunit, inhibiting translocation of peptide chain during protein synthesis. They are generally bacteriostatic.
| Agent | Coverage |
|---|---|
| Clindamycin (IV) | MSSA, streptococci (Group A, B), anaerobes above the diaphragm (Bacteroides, Peptostreptococcus), Toxoplasma (with pyrimethamine), Pneumocystis (with primaquine). NOT gram-negatives. |
| Quinupristin-dalfopristin (Synercid) (IV) | VRE (E. faecium only, NOT faecalis), MRSA, resistant streptococci. Bactericidal combo (component A binds 50S, B stabilizes complex). |
6. OXAZOLIDINONES (IV)
Mechanism of Action
Linezolid binds to the 23S rRNA of the 50S ribosomal subunit, blocking formation of the 70S initiation complex - a unique mechanism not shared by any other antibiotic class. This prevents translation before it even begins.
| Agent | Coverage |
|---|---|
| Linezolid (IV/oral) | MRSA (DOC alongside vancomycin), VRE (both faecalis and faecium), drug-resistant pneumococci, streptococci. Used in MDR-TB. Bacteriostatic against most organisms but bactericidal against streptococci. |
7. LIPOPEPTIDES (IV)
Mechanism of Action
Daptomycin inserts its lipid tail into the bacterial cell membrane in a calcium-dependent manner, causing rapid depolarization of the membrane potential. This leads to loss of intracellular potassium, inhibition of DNA/RNA/protein synthesis, and rapid bactericidal death.
| Agent | Coverage |
|---|---|
| Daptomycin (IV) | Gram-positives ONLY: MRSA, VRE, penicillin-resistant S. pneumoniae, S. aureus endocarditis, complicated skin infections. Inactivated by pulmonary surfactant - NEVER use for pneumonia. |
8. CARBOXYPENICILLINS & TETRACYCLINES - IV
Tigecycline (IV - Glycylcycline)
Mechanism: Binds 30S ribosome (same class as tetracyclines) but overcomes major resistance mechanisms. Inhibits protein synthesis.
Coverage: Very broad - MRSA, VRE, ESBL-producing Enterobacterales, Acinetobacter, anaerobes, atypicals. NOT reliable against Pseudomonas or Proteus. Used for complicated intra-abdominal and skin infections.
9. POLYMYXINS (IV)
Mechanism of Action
Polymyxin B and colistin (polymyxin E) act as detergents - they are cationic cyclic polypeptides that bind to the anionic lipopolysaccharide (LPS) of gram-negative outer membranes, displacing calcium and magnesium ions that normally stabilize the membrane. This disrupts membrane integrity, leading to cell lysis.
| Agent | Coverage |
|---|---|
| Colistin / Polymyxin B (IV) | Last-resort agents for MDR gram-negatives ONLY: carbapenem-resistant Acinetobacter, Pseudomonas, KPC-producing Klebsiella. No gram-positive or anaerobic activity. Significant nephrotoxicity. |
Summary Table
| Class | MOA Target | Bactericidal? | Gram+ | Gram- | Anaerobes | Key IV Agents |
|---|---|---|---|---|---|---|
| Penicillins | PBP / transpeptidase (cell wall) | Yes | ++ | +/- | +/- | Pen G, Pip-Tazo, Ampicillin |
| Cephalosporins | PBP / transpeptidase | Yes | ++ | ++ | +/- | Cefazolin, Ceftriaxone, Cefepime |
| Carbapenems | PBP / transpeptidase | Yes | ++ | +++ | +++ | Imipenem, Meropenem, Ertapenem |
| Monobactams | PBP / transpeptidase | Yes | - | +++ | - | Aztreonam |
| Glycopeptides | D-Ala-D-Ala (cell wall) | Yes* | +++ | - | - | Vancomycin |
| Aminoglycosides | 30S ribosome | Yes | +/- | +++ | - | Gentamicin, Amikacin |
| Fluoroquinolones | DNA gyrase / Topo IV | Yes | ++ | +++ | +/- | Ciprofloxacin, Levofloxacin |
| Clindamycin | 50S ribosome | No | ++ | - | +++ | Clindamycin |
| Linezolid | 50S / 70S initiation | No* | +++ | - | - | Linezolid |
| Daptomycin | Cell membrane | Yes | +++ | - | - | Daptomycin |
| Tigecycline | 30S ribosome | No | ++ | ++ | ++ | Tigecycline |
| Polymyxins | Outer membrane (LPS) | Yes | - | +++ | - | Colistin, Polymyxin B |
Linezolid is bactericidal vs streptococci; Vancomycin bacteriostatic vs Enterococcus
Key clinical pearls:
- MRSA: Vancomycin (1st line), Daptomycin, Linezolid, Ceftaroline
- Pseudomonas: Pip-tazobactam, Ceftazidime, Cefepime, Imipenem/Meropenem, Ciprofloxacin, Aztreonam, Tobramycin - never Ertapenem
- VRE: Linezolid, Daptomycin, Quinupristin-dalfopristin (faecium only)
- CRE (carbapenem-resistant Enterobacterales): Ceftazidime-avibactam, Meropenem-vaborbactam, Colistin, Tigecycline
- Anaerobes: Metronidazole, Pip-tazobactam, Carbapenems, Moxifloxacin, Clindamycin
How to remember easily gram postive and gram negative bacteria
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
I now have everything needed - two excellent flowcharts plus full content. Here's a comprehensive, memorable guide:
How to Remember Gram-Positive vs Gram-Negative Bacteria
Source: Harriet Lane Handbook 23rd Ed, Medical Microbiology 9th Ed, Jawetz 28th Ed
Step 1 - The Core Concept (Never Forget This)
| Gram-Positive | Gram-Negative | |
|---|---|---|
| Color | Purple (retains crystal violet) | Pink/Red (loses it, takes safranin) |
| Cell wall | Thick peptidoglycan (no outer membrane) | Thin peptidoglycan + outer lipid membrane (LPS) |
| Memory trick | "Purple Positive" | "Negative = Not purple = Nink (pink)" |
Think: "Gram-Positive = Pretty Purple" and "Gram-Negative = Not Purple (pink)"
Step 2 - The Master Visual Flowcharts
Here are the actual clinical classification flowcharts from Harriet Lane Handbook:
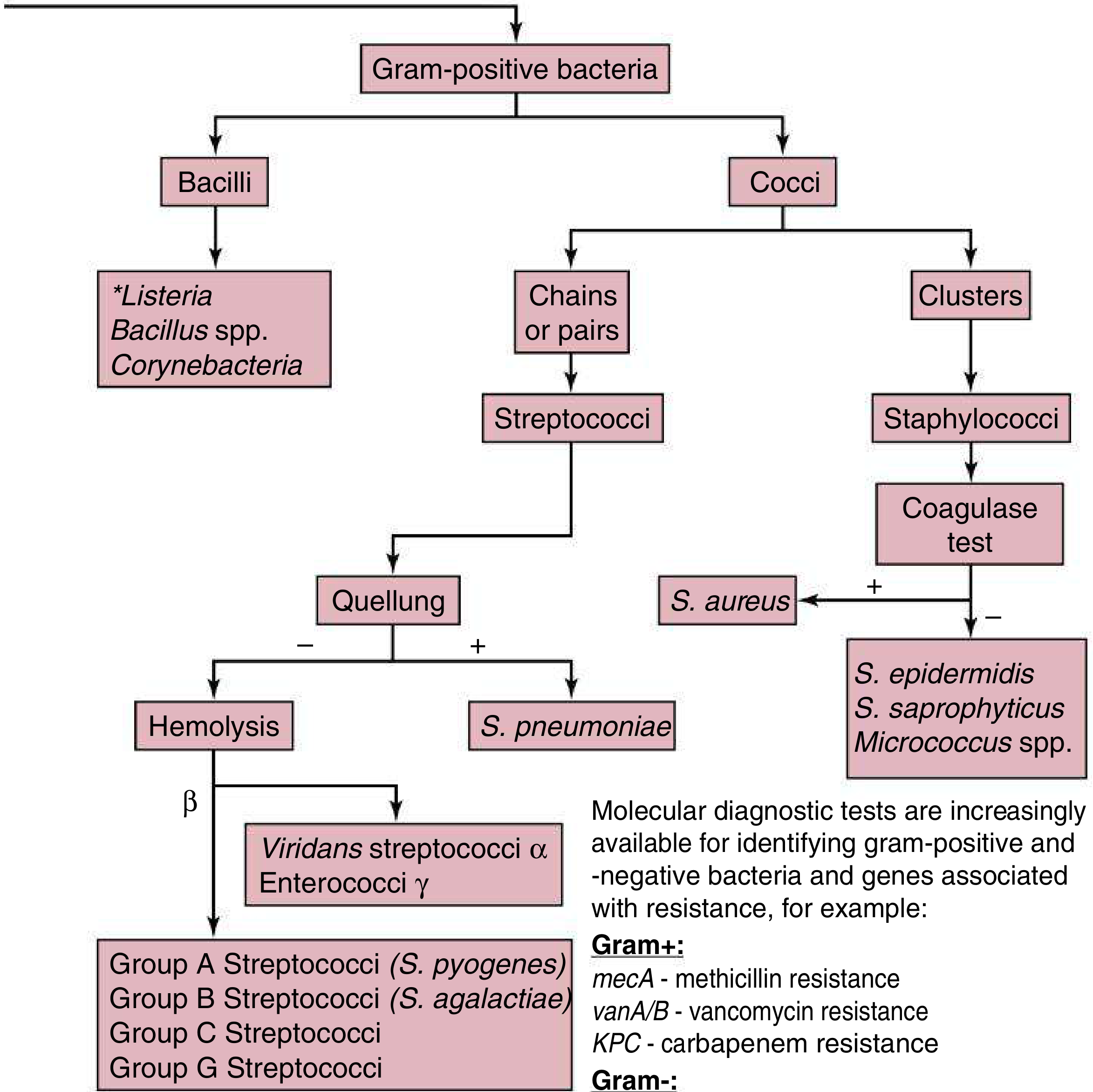
Gram-Positive bacteria (by morphology + diagnostic tests):
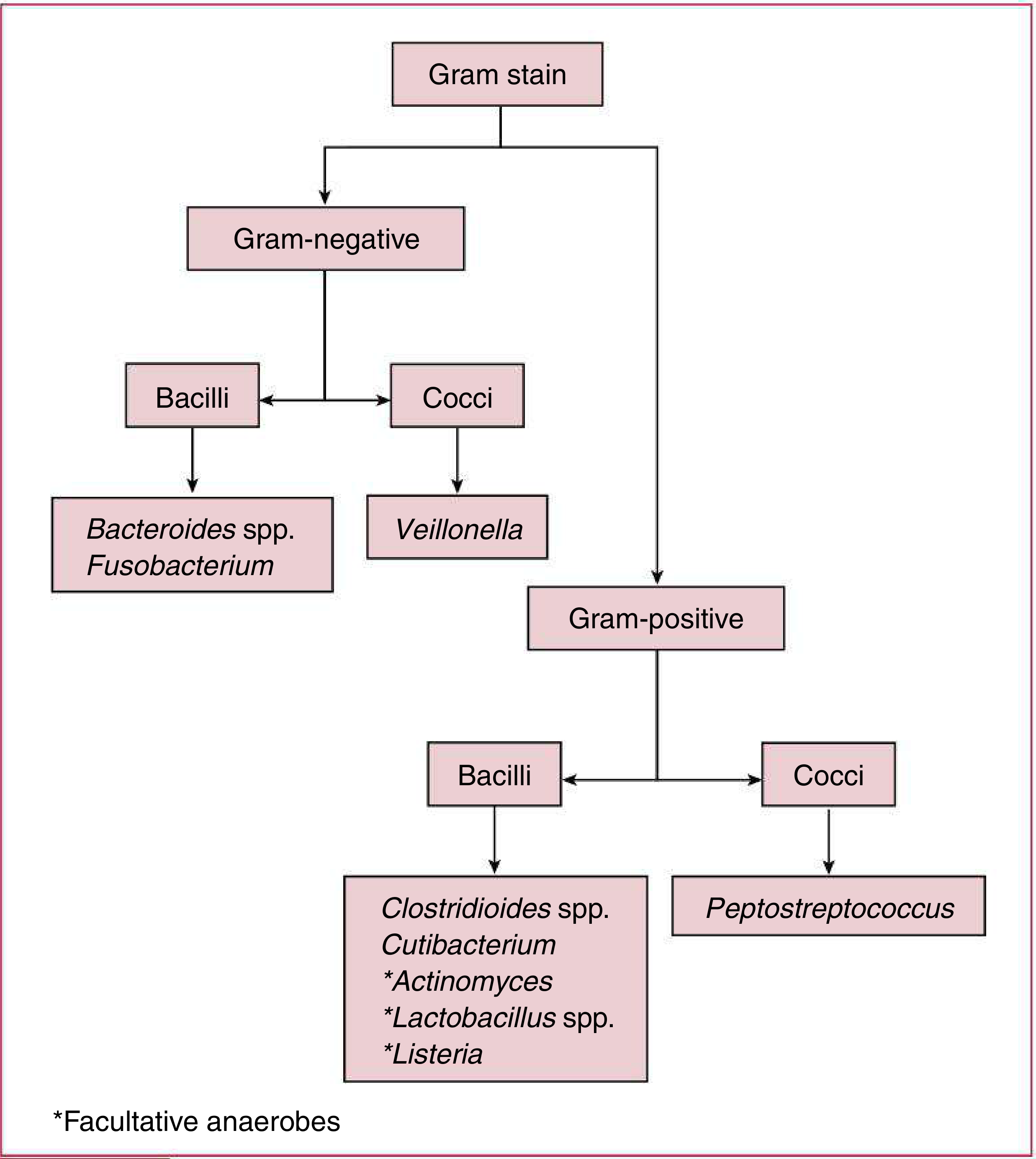
Anaerobic bacteria (gram-positive and gram-negative):
Step 3 - The BIG MNEMONIC Framework
Organize everything by shape first, then gram stain.
GRAM-POSITIVE COCCI
Mnemonic: "Staph Stays in Clusters, Strep Stays in Strings"
| Organism | Shape | Key Feature | Memory Hook |
|---|---|---|---|
| Staphylococcus aureus | Clusters | Coagulase + | "Staph = Sunflower seed clusters" |
| S. epidermidis | Clusters | Coagulase - | Lives on epidermis (skin) |
| S. saprophyticus | Clusters | UTI in young women | "Saphy loves young women's UTIs" |
| Streptococcus pyogenes (Grp A) | Chains | Beta-hemolysis | "Strep pyogenes = pyus (pus) maker" |
| S. agalactiae (Grp B) | Chains | Neonatal infection | Baby Bug (Group B) |
| S. pneumoniae | Pairs (diplococcus) | Quellung+ | "Pneumo = Lung" (pairs = lungs) |
| Enterococcus | Chains/pairs | GI/GU | Lives in entero (gut) |
Quick mnemonic for Gram+ Cocci:
"Silly Students Sometimes Eat Peanut Butter Sandwiches" S. aureus, S. epidermidis, S. saprophyticus, Enterococcus, Pneumococcus, Beta-strep (Grp A/B), S. viridans
GRAM-POSITIVE RODS (Bacilli)
Mnemonic: "Listen Back Corny Clostridium"
| Organism | Key Disease | Memory Hook |
|---|---|---|
| Listeria monocytogenes | Meningitis (newborns/elderly), listeriosis | "Listens to cold" - grows in fridge (cold enrichment!) |
| Bacillus anthracis | Anthrax | "Big spores" - Bacillus = Big spore former |
| Bacillus cereus | Food poisoning (fried rice) | "Serious cereal (rice) problem" |
| Corynebacterium diphtheriae | Diphtheria | "Corny diphtheria" - Club-shaped = corn club |
| Clostridium perfringens | Gas gangrene | "Perfect gas gang" |
| C. tetani | Tetanus | "Tetanus = Tetraspasm" |
| C. botulinum | Botulism | "Bottle poison" |
| C. difficile | Pseudomembranous colitis | "Difficult diarrhea" |
| Actinomyces | Lumpy jaw | Actino = Acts like fungus but it's NOT |
GRAM-NEGATIVE COCCI
Only 2 you need to remember!
Mnemonic: "The Two Neisseria Neighbors"
| Organism | Disease | Memory Hook |
|---|---|---|
| Neisseria meningitidis | Meningitis | "Meningitidis = Mind infection" |
| Neisseria gonorrhoeae | Gonorrhea | "Gonorrhea = Genital" |
Both are diplococci (kidney-bean shaped pairs), oxidase-positive, intracellular.
GRAM-NEGATIVE RODS (Bacilli) - The Big Group
This is the hardest group. Use the "SEEK PPH + MYBHVS" system:
Enterobacteriaceae ("The Enteric Family")
Mnemonic: "Eggs Kinda Smell, People Sneeze Every Saturday"
| Bug | Disease | Hook |
|---|---|---|
| Escherichia coli | UTI, meningitis (neonates), diarrhea | E = Everywhere |
| Klebsiella pneumoniae | Pneumonia (alcoholics), UTI | Klebsiella = Killer pneumonia (currant jelly sputum) |
| Salmonella | Typhoid, food poisoning | Salad = Salmonella |
| Shigella | Dysentery | Shigella = Shits blood |
| Proteus mirabilis | UTI, kidney stones | Proteus = urease+ = Pee rocks (struvite stones) |
| Enterobacter | Nosocomial infections | Enterobacter = Enter hospital first |
| Serratia marcescens | Nosocomial pneumonia/UTI | Serratia = Scarlet (red pigment) |
The "SPACE" Organisms (AmpC beta-lactamase inducers)
Mnemonic: "SPACE"
- Serratia
- Pseudomonas
- Acinetobacter / Aeromonas
- Citrobacter / C. freundii
- Enterobacter
Non-Enteric Gram-Negative Rods
Mnemonic: "Please Have Better Luck Fighting Bugs"
| Bug | Disease | Hook |
|---|---|---|
| Pseudomonas aeruginosa | Lung (CF), burns, ICU | Pseu = Pool/hot tub bug, Blue-green pus |
| Haemophilus influenzae | Meningitis, otitis, epiglottitis | Haemo = needs blood factors (X and V) |
| Bordetella pertussis | Whooping cough | Border = Borderline violent cough |
| Legionella pneumophila | Legionnaire's disease | Living in water coolers / AC systems |
| Francisella tularensis | Tularemia | Francis the rabbit farmer (rabbit contact) |
| Brucella | Brucellosis | Brucella = Brute animal contact |
Spiral/Curved Gram-Negatives
Mnemonic: "Campy Heli Vibrio"
| Bug | Disease | Hook |
|---|---|---|
| Campylobacter jejuni | Bloody diarrhea, Guillain-Barré | Camp food = Campy |
| Helicobacter pylori | Peptic ulcer, gastric cancer | Heli = Helix living in stomach |
| Vibrio cholerae | Cholera (rice water stools) | Vibrio = Violent vomiting |
Step 4 - The "Special" Categories (Neither standard G+ nor G-)
| Bug | Gram Stain | Why Special | Hook |
|---|---|---|---|
| Mycobacterium (TB, leprae) | Acid-fast (neither) | Waxy mycolic acid wall | "Myco = waxy coat" |
| Mycoplasma | Cannot be stained | No cell wall at all | "Mycoplasma = no wall = no penicillin effect" |
| Treponema pallidum | Too thin to stain | Spirochete | "Treponema = Treponema (syphilis spiral)" |
| Rickettsia, Chlamydia | Obligate intracellular | Cannot grow outside cells | "Rick and Chlam only live inside" |
Step 5 - Quick 60-Second Recall Table
| Category | Gram+ | Gram- |
|---|---|---|
| Cocci | Staph (clusters), Strep (chains), Pneumo (pairs), Entero | Neisseria (pairs) |
| Rods | Listeria, Bacillus, Coryne, Clostridium, Actinomyces | E. coli, Klebsiella, Salmonella, Shigella, Proteus, Pseudomonas, H. influenzae, Legionella |
| Spiral | None | Campylobacter, H. pylori, Vibrio, Treponema |
Step 6 - One Final Super-Mnemonic
GRAM POSITIVE = "Silly Staph, Strep, and Enterococcus Love Being Corny Clowns At Christmas"
- Staph, Strep, Enterococcus (cocci)
- Listeria, Bacillus, Corynebacterium, Clostridium, Actinomyces (rods)
GRAM NEGATIVE = "Every Kilogram Salted Shrimp Produces Energy, Silly People Have Legs, Frank Buys Vibrant Camphor"
- Enterobacterales: E. coli, Klebsiella, Salmonella, Shigella, Proteus, Enterobacter, Serratia
- Pseudomonas, H. influenzae, Legionella, Francisella, Brucella, Vibrio, Campylobacter
The two flowcharts above (from Harriet Lane Handbook 23rd Ed) are the best visual reference - they show exactly how to classify any unknown organism step by step using morphology, hemolysis, coagulase test, and Quellung reaction.
Anerobes
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Here is the full guide on anaerobes:
Anaerobes - Complete Guide
Source: Harrison's Principles of Internal Medicine 22E (2025), Jawetz Medical Microbiology 28th Ed, Medical Microbiology 9th Ed
What Are Anaerobes?
Bacteria that cannot survive in the presence of oxygen (or require very low oxygen tension). They lack superoxide dismutase and/or catalase, so they cannot detoxify oxygen free radicals.
Key rule: Anaerobes live at mucosal surfaces as normal flora and cause disease only when they breach those surfaces into low-oxygen environments (abscesses, necrotic tissue, deep wounds).
The Master Classification
ANAEROBES
├── GRAM-POSITIVE
│ ├── Spore-forming RODS → Clostridium spp.
│ ├── Non-spore-forming RODS → Actinomyces, Propionibacterium, Lactobacillus, Bifidobacterium
│ └── COCCI → Peptostreptococcus (Finegoldia magna)
│
└── GRAM-NEGATIVE
├── RODS → Bacteroides fragilis group, Prevotella, Porphyromonas, Fusobacterium
└── COCCI → Veillonella
GRAM-POSITIVE ANAEROBES
1. Clostridium - The Spore-Formers (Most Important!)
Mnemonic: "4 Terrible Toxin Producers - BPDT"
"Big Patients Die Terribly" = Botulinum, Perfringens, Difficile, Tetani
| Species | Disease | Toxin/Mechanism | Key Memory Hook |
|---|---|---|---|
| C. botulinum | Botulism (flaccid paralysis, floppy baby) | Blocks ACh release at NMJ | "Bottle poison = Bottom of can (canned food)" |
| C. perfringens | Gas gangrene, food poisoning | Alpha toxin (lecithinase), destroys cell membranes | "Perfect gas gang" - crackling, foul wound |
| C. difficile | Pseudomembranous colitis (antibiotic-associated diarrhea) | Toxin A (enterotoxin) + Toxin B (cytotoxin) | "Difficult diarrhea after antibiotics" |
| C. tetani | Tetanus (spastic paralysis) | Tetanospasmin - blocks glycine/GABA (inhibitory NTs) | "Tetanus = Tetanic spasms (lockjaw)"** |
| C. septicum | Spontaneous gas gangrene | Associated with colon cancer | "Septicum = secret cancer sign" |
Clostridium key facts:
- All gram-positive, spore-forming rods
- Found in soil and GI tract
- Spores survive boiling, autoclaving needed
- C. tetani and C. botulinum are obligate anaerobes; C. perfringens is more aerotolerant
2. Actinomyces
| Feature | Detail |
|---|---|
| Gram stain | Gram-positive rod (branching) |
| Distinguishing feature | Sulfur granules in pus (yellow, gritty) |
| Key infection | Lumpy jaw (cervicofacial actinomycosis), pulmonary actinomycosis, pelvic actinomycosis (IUD-associated) |
| Looks like but isn't | Fungus (it's a bacterium!) |
| Treatment | Penicillin G for prolonged duration (months) |
Mnemonic: "Actino-MY-ces = MINE! Lives in MY jaw, MY lung, MY pelvis"
3. Peptostreptococcus (Finegoldia magna)
- Gram-positive anaerobic cocci in chains
- Part of normal flora of mouth, GI, vagina
- Causes: mixed wound infections, pelvic abscess, brain abscess, aspiration pneumonia
- Treat with penicillin, clindamycin, metronidazole
GRAM-NEGATIVE ANAEROBES
1. Bacteroides fragilis - THE Most Clinically Important Anaerobe
| Feature | Detail |
|---|---|
| Gram stain | Gram-negative rod (pleomorphic) |
| Normal home | Colon (dominant anaerobe in gut) |
| Why dangerous | Produces beta-lactamase (resistant to penicillin) + has capsule (resists phagocytosis) |
| Key infections | Intra-abdominal abscess, peritonitis, pelvic abscess, bacteremia |
| Virulence | Fragilysin (BFT toxin) - metalloprotease causing diarrhea |
| Resistance | Resists penicillin G (always produce beta-lactamase) |
Mnemonic: "B. fragilis = FRAG-ile penicillin won't work, use METRO"
B. fragilis group also includes: B. thetaiotaomicron, B. ovatus, B. distasonis - all in the colon.
From Harrison's 22E: "B. fragilis is the anaerobe most commonly isolated from blood cultures... isolation from blood indicates underlying infection associated with a 60% mortality rate if untreated."
2. Prevotella & Porphyromonas
| Feature | Detail |
|---|---|
| Location | Mouth, upper respiratory tract, female genital tract |
| Key infections | Periodontal disease, aspiration pneumonia, lung abscess, brain abscess, pelvic infections |
| Color clue | Black pigmented colonies on blood agar (Prevotella melaninogenica, Porphyromonas) |
| Beta-lactamase | Yes - about 2/3 of strains produce it |
Mnemonic: "Pre-VOTT-ella = Previous mouth/throat bug (oro-dental)"
3. Fusobacterium nucleatum / necrophorum
| Feature | Detail |
|---|---|
| Shape | Long, thin, fusiform (spindle-shaped) gram-negative rod |
| Key syndrome | Lemierre's syndrome - septic thrombophlebitis of internal jugular vein following pharyngitis (F. necrophorum) |
| Also causes | Aspiration pneumonia, lung abscess, Vincent's angina (trench mouth) |
| Clue | Found in oropharyngeal infections, especially in young adults post-tonsillitis |
Mnemonic: "Fuso = Fuse the throat vein shut (Lemierre's)"
4. Veillonella
- Gram-negative anaerobic cocci (tiny)
- Only gram-negative anaerobic cocci of clinical significance
- Normal flora of the mouth and GI tract
- Rarely pathogenic but found in mixed infections
Mnemonic: "Veil-onella = hidden behind the veil (rarely causes disease alone)"
WHERE Do Anaerobes Cause Infection? (Clinical Distribution)
Distribution of anaerobic infections from Harrison's 22E:
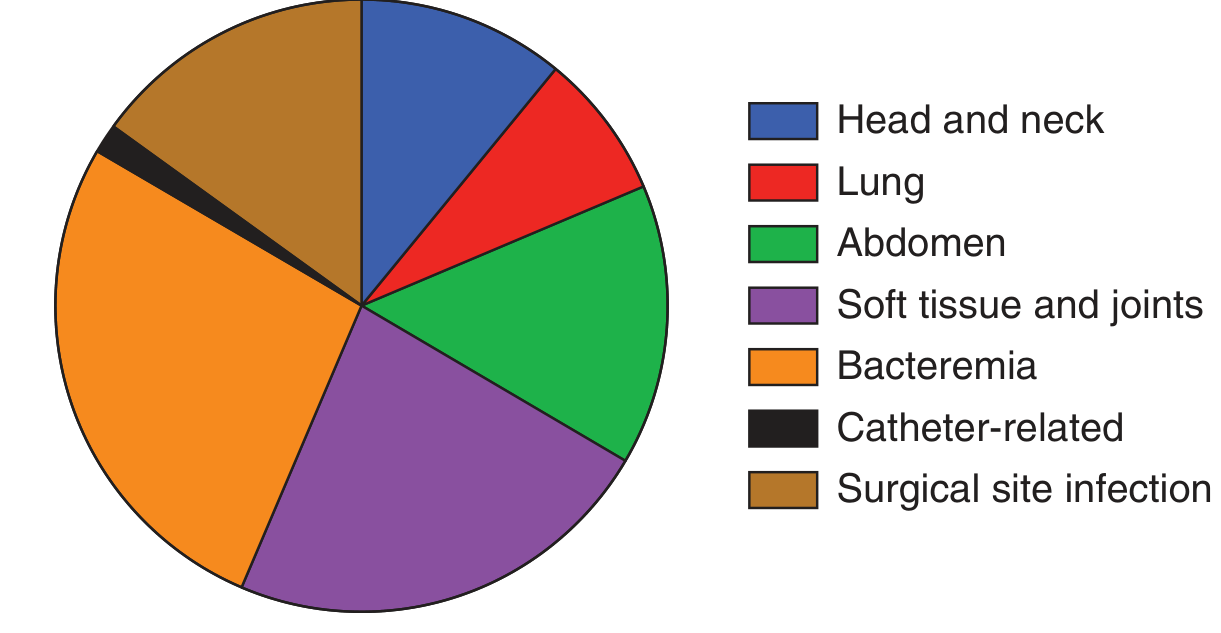
Key rule - Above vs. Below the Diaphragm:
| Location | Predominant Anaerobes | Key Antibiotics |
|---|---|---|
| Above diaphragm (mouth, lung, brain) | Prevotella, Porphyromonas, Fusobacterium, Peptostreptococcus | Clindamycin (1st choice above) + penicillin |
| Below diaphragm (abdomen, pelvis) | Bacteroides fragilis group | Metronidazole + cover gram-negatives; carbapenems; pip-tazo |
From Jawetz 28th Ed: "Clindamycin is preferred for infections above the diaphragm. Relatively few anaerobes are resistant to clindamycin (B. fragilis group excepted) and few, if any, are resistant to metronidazole."
Clinical Clues That Scream "ANAEROBE!"
Mnemonic: "FANG + G"
| Clue | Meaning |
|---|---|
| F - Foul smell | Putrid, offensive discharge (volatile fatty acids) |
| A - Abscess / Avascular tissue | Necrotic tissue, abscesses in deep sites |
| N - Negative aerobic culture | "Sterile pus" on routine culture - Gram stain shows organisms |
| G - Gas in tissues | Crepitus on palpation (especially Clostridium) |
| G - Gingival / GI / Genital proximity | Infection near mucosa (bowel, mouth, vagina) |
Treatment Summary
| Drug | Coverage | Use |
|---|---|---|
| Metronidazole | All obligate anaerobes (best drug) | Below-diaphragm infections; B. fragilis; CNS anaerobes |
| Clindamycin | Excellent above-diaphragm anaerobes | Lung abscess, orofacial infections; NOT B. fragilis (resistance rising) |
| Piperacillin-tazobactam | Anaerobes + gram-negatives | Mixed infections, peritonitis |
| Carbapenems (imipenem, meropenem, ertapenem) | Broadest anaerobic cover | Severe mixed/intra-abdominal infections |
| Cefoxitin / Cefotetan | Anaerobes including B. fragilis | Surgical prophylaxis (bowel surgery) - NOTE: resistance increasing |
| Penicillin G | Non-beta-lactamase anaerobes (Clostridium, Actinomyces, Peptostreptococcus) | Actinomycosis, C. tetani/botulinum/perfringens |
| Tigecycline | Most anaerobes including B. fragilis | Complicated intra-abdominal infections |
NEVER use: Aminoglycosides (inactive - require O₂ uptake), Aztreonam (gram-negative aerobes only), trimethoprim-sulfamethoxazole
Quick Memory Table - All Key Anaerobes
| Anaerobe | G+/G- | Shape | Key Disease | Treatment | Memory Hook |
|---|---|---|---|---|---|
| C. botulinum | G+ | Rod (spore) | Botulism (flaccid) | Antitoxin | Canned food, honey, floppy baby |
| C. tetani | G+ | Rod (spore) | Tetanus (spastic) | Antitoxin + Pen G | Rusty nail, drumstick spore |
| C. perfringens | G+ | Rod (spore) | Gas gangrene, food poisoning | Surgical + Pen G | Gas in wound, crepitus |
| C. difficile | G+ | Rod (spore) | Pseudomembranous colitis | Oral Vanc / Fidaxomicin | Post-antibiotic diarrhea |
| Actinomyces | G+ | Rod (branching) | Lumpy jaw, pelvic (IUD) | Pen G (long course) | Sulfur granules |
| Peptostreptococcus | G+ | Cocci | Mixed wound/pelvic abscess | Pen G, Clindamycin | Normal mouth/vaginal flora |
| B. fragilis | G- | Rod | Intra-abdominal abscess, bacteremia | Metronidazole / Carbapenems | Colon resident, beta-lactamase |
| Prevotella | G- | Rod | Lung abscess, periodontal | Clindamycin / Metro | Black pigment, mouth bug |
| Fusobacterium | G- | Rod (fusiform) | Lemierre's, Vincent's angina | Metronidazole / Pen G | JV thrombosis post-sore throat |
| Veillonella | G- | Cocci | Rarely pathogenic | Metro | Only GN anaerobic cocci |
The Single Best Mnemonic to Remember All Anaerobes
"Can Peter Eat Foul Pus? Big Bacteria Prefer Foul Veggies"
- Clostridium (4 types: Bot, Perf, Diff, Tet)
- Peptostreptococcus
- E - (Actinomyces → has "es" sound)
- Fusobacterium
- Prevotella / Porphyromonas
- Bacteroides fragilis
- Bifido / other non-spore G+ rods
- Putrid smell = clue to all
- Fragilis = below diaphragm
- Veillonella = GN cocci
This is a shared conversation. Sign in to Orris to start your own chat.