Cardiac reflexes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
I now have all the material needed for a comprehensive answer. Let me compile it:
Cardiac Reflexes
Cardiac reflexes are autonomic feedback mechanisms that regulate heart rate, contractility, and arterial blood pressure in response to sensory inputs from receptors located in the heart, great vessels, and other organs. They operate through reflex arcs: receptor → afferent nerve → medullary cardiovascular center → efferent nerve → effector (heart/vessels).
1. Baroreceptor Reflex (Carotid Sinus / Aortic Arch Reflex)
This is the primary, best-known cardiac reflex for short-term blood pressure regulation.
Receptors
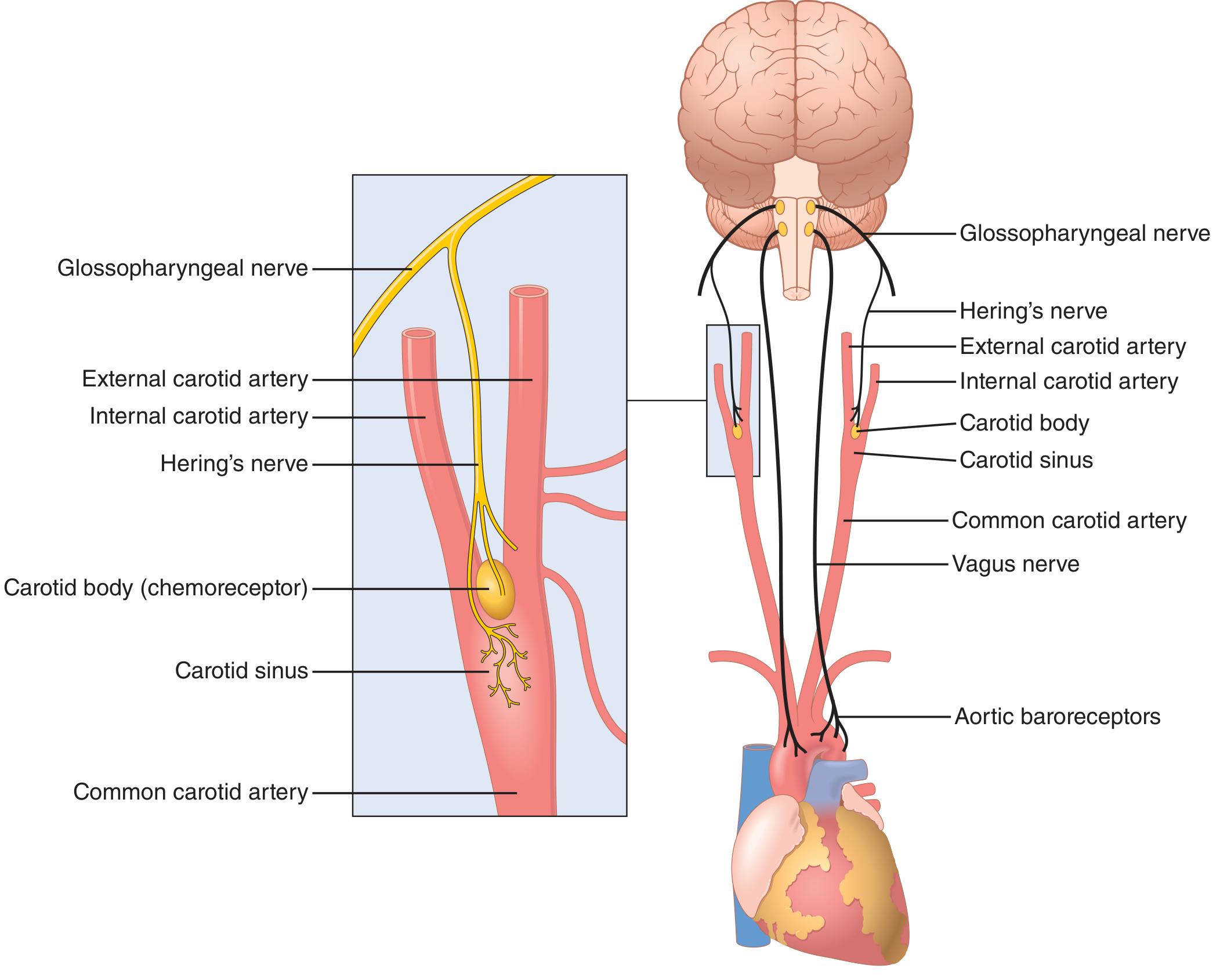
Baroreceptors are spray-type mechanoreceptors (stretch receptors) located in:
- Carotid sinus - the dilated portion of the internal carotid artery just above the carotid bifurcation
- Aortic arch - respond mainly to increases in pressure (less sensitive to hypotension than carotid sinus receptors)
They are most sensitive to rapid changes in pressure rather than a static level.
Afferent Pathway
| Location | Nerve |
|---|---|
| Carotid sinus | Hering's nerve → Glossopharyngeal nerve (CN IX) |
| Aortic arch | Vagus nerve (CN X) |
Both pathways converge on the nucleus tractus solitarius (NTS) in the medullary cardiovascular center.
Central Processing
The NTS is the primary relay. It projects to two functionally distinct medullary areas:
- Lateral rostral area - raises blood pressure (sympathoexcitatory)
- Central caudal area - lowers blood pressure (sympathoinhibitory); also integrates input from hypothalamus and limbic system
Efferent Response to Hypertension (↑ BP)
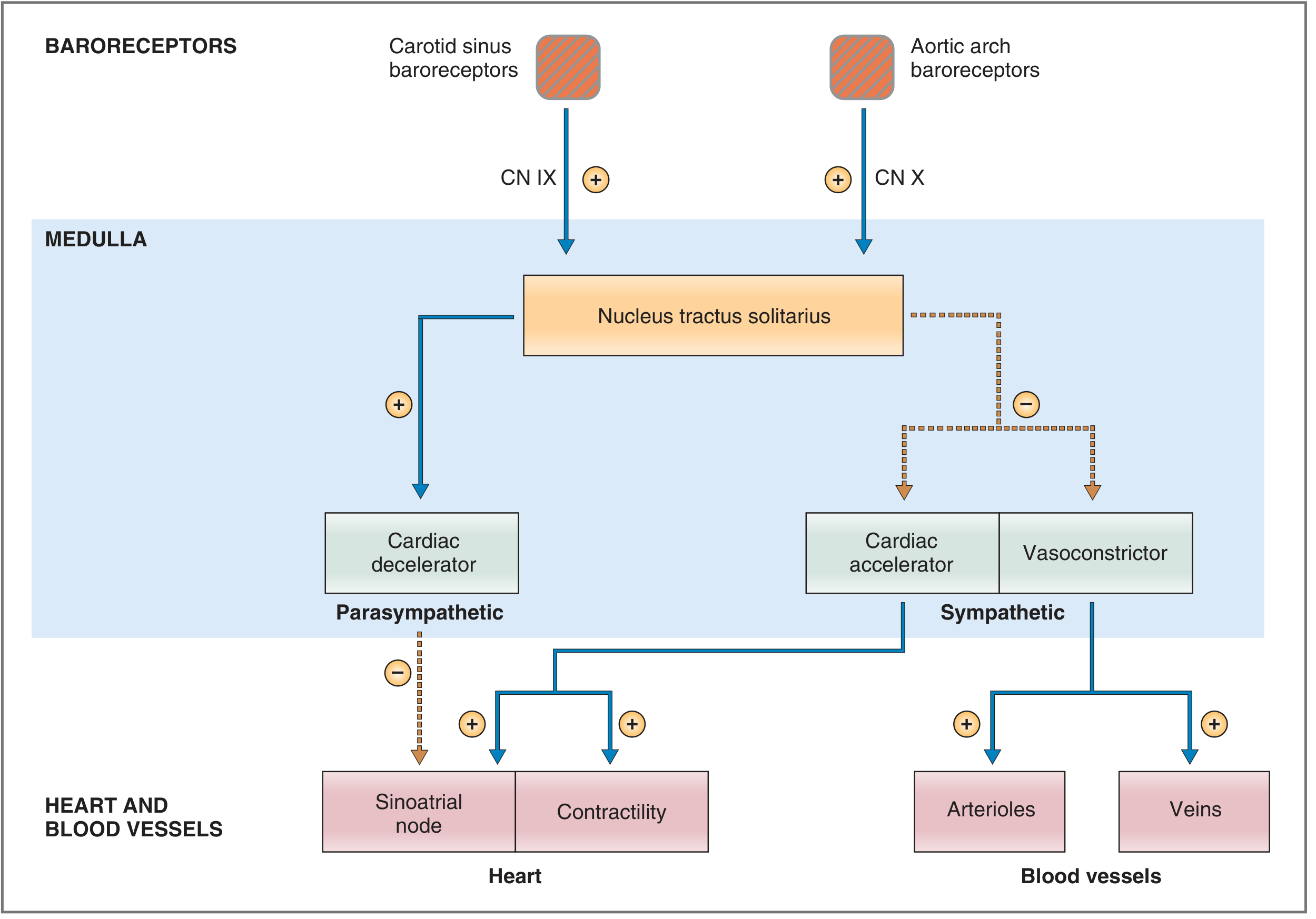
- Increased baroreceptor firing → NTS activation
- ↓ Sympathetic outflow: decreased heart rate, contractility, arteriolar and venous tone
- ↑ Parasympathetic (vagal) outflow: further decreases heart rate and contractility
- Net result: ↓ HR, ↓ CO, ↓ TPR → ↓ BP
Efferent Response to Hypotension (↓ BP)
- Decreased baroreceptor firing → reduced NTS inhibition of sympathetic centers
- ↑ Sympathetic outflow: increased HR, contractility, arteriolar vasoconstriction, venous constriction (reduces unstressed volume, increases venous return)
- ↓ Parasympathetic outflow: further increases HR
- Net result: ↑ HR, ↑ CO, ↑ TPR → ↑ BP
Key Points
- Baroreceptors are not stimulated below 50-60 mmHg; maximal activity around 180 mmHg (carotid); aortic baroreceptors operate ~30 mmHg higher
- The reflex is most sensitive in the normal operating range (~100 mmHg)
- They respond more to rate of pressure change than to absolute pressure
- In chronic hypertension, the set point is "reset" upward - the reflex maintains the elevated pressure rather than correcting it
- Volatile anesthetics (especially halothane) inhibit the heart rate component of this reflex
- Loses functional capacity when BP falls below 50 mmHg
Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology 7e; Miller's Anesthesia 10e
2. Chemoreceptor Reflex
Receptors
Peripheral chemoreceptors are located in the:
- Carotid bodies (at the carotid bifurcation)
- Aortic body
They respond to:
- PaO₂ < 50 mmHg (hypoxia)
- Acidosis (↓ pH)
- Elevated PaCO₂
Afferent Pathway
- Carotid bodies → sinus nerve of Hering → glossopharyngeal nerve (CN IX)
- Aortic body → vagus nerve (CN X)
- Both converge on the chemosensitive area of the medulla
Response
- Stimulation of respiratory centers → increased ventilatory drive
- Activation of parasympathetic system → ↓ heart rate and ↓ myocardial contractility
- In persistent hypoxia: direct CNS stimulation → ↑ sympathetic activity (overrides initial bradycardia)
Miller's Anesthesia 10e
3. Bainbridge Reflex (Atrial Reflex / Volume Reflex)
Trigger
Increased right-sided filling pressure (e.g., rapid IV fluid infusion, increased venous return).
Receptor & Pathway
- Stretch receptors in the right atrial wall and cavoatrial junction
- Afferents travel via the vagus nerve to the medullary cardiovascular center
Response
- Inhibition of parasympathetic outflow → tachycardia
- Direct mechanical stretch of the SA node also contributes to rate increase
- The net change in heart rate depends on the baseline heart rate at time of stimulation
Physiologic role: Prevents blood from pooling in the venous circulation - when more blood returns to the heart, the heart speeds up to pump it out. This is an important mechanism during exercise and volume loading.
Miller's Anesthesia 10e
4. Bezold-Jarisch Reflex
Trigger
Noxious stimuli within the left ventricular wall - activation of ventricular chemoreceptors and mechanoreceptors by:
- Myocardial ischemia or infarction
- Reperfusion/thrombolysis/revascularization
- Certain drugs (veratrum alkaloids, serotonin, capsaicin)
- Excessive ventricular mechanoreceptor stretch
Receptor & Pathway
- C-fiber (type C, unmyelinated) vagal afferents in the LV wall
- Signals travel to medulla via vagus nerve
Response - Classic Triad:
- Bradycardia
- Hypotension (vasodilation)
- Coronary artery dilation
All mediated by increased parasympathetic tone.
Clinical Significance
- Considered a cardioprotective reflex - reduces myocardial oxygen demand during ischemia
- Implicated in syncope (vasovagal episodes)
- May contribute to bradycardia/hypotension following inferior MI (inferior wall has highest receptor density) or post-thrombolysis
- Natriuretic peptides (ANP, BNP) modulate this reflex via their receptors
- Less pronounced in cardiac hypertrophy and atrial fibrillation
Miller's Anesthesia 10e
5. Cushing Reflex (CNS Ischemic Response)
Trigger
Raised intracranial pressure (ICP) → cerebral ischemia → CO₂ accumulation at medullary vasomotor center.
Response - Cushing's Triad:
- Hypertension (powerful sympathetic activation, can raise BP to 250 mmHg)
- Bradycardia (baroreceptor-mediated reflex in response to the hypertension)
- Irregular/slow respirations (Cheyne-Stokes pattern)
Mechanism
Cerebral ischemia at the vasomotor center → local CO₂ buildup + acidosis → intense sympathetic activation → hypertension → baroreceptor-mediated reflex bradycardia.
Role
- Operates only when BP falls below ~60 mmHg (cerebral perfusion threatened)
- Does NOT function as a normal BP regulator
- Functions as a "last-ditch" emergency mechanism to maintain cerebral perfusion
- The specific form triggered by raised CSF pressure is the Cushing reaction
Guyton and Hall Textbook of Medical Physiology; Miller's Anesthesia 10e
6. Oculocardiac Reflex
Trigger
- Pressure applied to the globe of the eye
- Traction on extraocular muscles or periorbital structures
- Common during ophthalmic surgery (especially strabismus surgery in children)
Receptor & Afferent Pathway
- Stretch receptors in extraocular muscles
- Short and long ciliary nerves → nasociliary branch of ophthalmic nerve (CN V₁) → trigeminal ganglion → trigeminal nerve (CN V)
Efferent Pathway
- Vagus nerve (CN X) → SA node
Response
- Bradycardia (can be profound)
- Nausea, vomiting
- Hypotension
- In severe cases: atrioventricular block, ventricular arrhythmias, asystole
Clinical Management
- Prophylaxis: retrobulbar block (interrupts the afferent limb) or IV atropine/glycopyrrolate before surgery
- Treatment: stop ocular stimulation immediately; give IV atropine if bradycardia persists
- Particularly pronounced in children and with hypoxia, hypercapnia, or light anesthesia
Miller's Anesthesia 10e; Barash Clinical Anesthesia 9e
7. Valsalva Maneuver - Cardiovascular Reflex Responses
Forced expiration against a closed glottis produces a stereotyped sequence:
| Phase | Mechanism | Effect |
|---|---|---|
| Phase I (strain onset) | ↑ intrathoracic pressure → ↑ BP transiently | Brief hypertension |
| Phase II | ↓ venous return → ↓ CO → ↓ BP → baroreceptors detect ↓ BP | Tachycardia, ↑ TPR |
| Phase III (release) | ↓ intrathoracic pressure, venous pooling | Brief hypotension |
| Phase IV | ↑ venous return → overshoot ↑ BP → baroreceptors detect ↑ BP | Reflex bradycardia |
The Phase IV bradycardia is a baroreceptor-mediated parasympathetic response. An absent overshoot and absent bradycardia indicate autonomic neuropathy or baroreceptor dysfunction.
Miller's Anesthesia 10e
Summary Table
| Reflex | Trigger | Receptor Site | Afferent | Response |
|---|---|---|---|---|
| Baroreceptor | ↑ or ↓ arterial pressure | Carotid sinus, aortic arch | CN IX, CN X → NTS | ↓ BP: tachycardia, vasoconstriction; ↑ BP: bradycardia, vasodilation |
| Chemoreceptor | Hypoxia, acidosis | Carotid/aortic bodies | CN IX, CN X | ↑ ventilation; ↓ HR initially |
| Bainbridge | ↑ venous return / atrial filling | RA wall, cavoatrial junction | Vagal afferents → medulla | Tachycardia |
| Bezold-Jarisch | LV noxious stimuli (ischemia) | LV wall (C-fibers) | Vagal C-fibers | Bradycardia + hypotension + coronary dilation |
| Cushing | ↑ ICP → cerebral ischemia | Medullary vasomotor center (CO₂) | Direct CNS | Hypertension + reflex bradycardia |
| Oculocardiac | Ocular pressure/traction | Extraocular muscle receptors | CN V → CN X | Bradycardia, arrhythmia |
Go on
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Excellent content gathered. Now I have everything needed to continue comprehensively. Here is the extended coverage:
Continuing Cardiac Reflexes
8. Low-Pressure Receptor Reflex (Cardiopulmonary / Volume Receptor Reflex)
This is the counterpart to the high-pressure baroreceptor system. It monitors venous filling and volume rather than arterial pressure.
Receptors
"Low-pressure receptors" (volume receptors) are stretch receptors located in:
- Right atrial wall and cavoatrial junction
- Pulmonary blood vessels
- Ventricular walls
Afferent Pathway
Signals travel via vagal afferents to the medullary cardiovascular centers and hypothalamus.
Response to Increased Venous Volume / Stretch
- Inhibition of sympathetic renal nerve activity → decreased tubular sodium reabsorption → natriuresis and diuresis
- Suppression of ADH (vasopressin) secretion from the posterior pituitary → water diuresis
- Suppression of the renin-angiotensin-aldosterone system (RAAS) → further reduction in sodium retention
- Stimulation of ANP release from atrial cardiomyocytes → added natriuresis
Physiologic Role
This reflex is most important in the first few hours after a large increase in salt and water intake. It acts as a volume sensor - when blood is "full," the body sheds salt and water. It is distinct from the arterial baroreceptor reflex but both cooperate to stabilize cardiovascular homeostasis.
The Bainbridge reflex (tachycardia with atrial stretch) is the heart rate arm of this same low-pressure receptor system. The natriuresis/diuresis response just described is the renal arm.
Guyton and Hall Textbook of Medical Physiology; Medical Physiology (Boron & Boulpaep)
9. Bainbridge Reflex - Deeper Understanding
The Bainbridge reflex interacts with the baroreceptor reflex in a biphasic, competing fashion to control heart rate:
| Blood Volume State | Dominant Reflex | Heart Rate Effect |
|---|---|---|
| Volume loading (↑ venous return) | Bainbridge reflex | ↑ HR (tachycardia) |
| Volume depletion (↓ arterial pressure) | Baroreceptor reflex | ↑ HR (tachycardia) |
| Normal blood volume | Both balanced | HR at minimum |
Key consequence: both volume loading and volume depletion raise heart rate - by different mechanisms. Heart rate is minimal at normal blood volume.
The Bainbridge reflex saturates at high atrial pressures. Its heart-rate effect is greatest when the baseline HR is slow. Its efferent limb runs via both parasympathetic (withdrawal) and sympathetic (activation) pathways to the SA node. Contractility and stroke volume are NOT significantly altered by the Bainbridge reflex - it is purely a chronotropic reflex.
Direct atrial stretch of the SA node itself accounts for ~15% of the HR increase; the neural Bainbridge reflex accounts for the remaining 40-60%.
Guyton and Hall; Medical Physiology (Boron & Boulpaep)
10. Vasovagal (Neurocardiogenic) Syncope
This is the most common clinical expression of an exaggerated cardiac reflex. It is technically a reflex-mediated syncope.
Mechanism
- Prolonged standing, emotional stress, pain, or venous pooling reduces venous return
- The LV contracts vigorously around a low volume → paradoxically activates ventricular mechanoreceptors (C-fibers - same as Bezold-Jarisch)
- This triggers sudden withdrawal of sympathetic tone + surge in vagal (parasympathetic) tone
- Result: vasodilation + bradycardia → precipitous fall in BP → cerebral hypoperfusion → syncope
Triggers
- Prolonged upright posture
- Fear, pain, emotional distress
- Venipuncture/instrumentation
- Prolonged standing in warm/crowded environments
- Situational: coughing, micturition, defecation, swallowing
Subtypes (by ESC classification)
| Type | HR response | BP response |
|---|---|---|
| Cardioinhibitory | Predominant bradycardia (asystole ≥3s) | Variable |
| Vasodepressor | Little or no bradycardia | Pronounced hypotension |
| Mixed | Both bradycardia and hypotension | Both fall |
Prodromal Symptoms
Diaphoresis, nausea, "warm sensation," pallor, lightheadedness - mediated by the sympathetic surge that precedes the vasovagal collapse.
Management
- Lifestyle: hydration, salt intake, avoidance of triggers, physical counter-pressure maneuvers (leg crossing, tensing)
- Compression stockings
- Pharmacological: fludrocortisone, midodrine, beta-blockers (selected cases)
- Cardioinhibitory type with recurrent severe episodes: pacemaker implantation
Braunwald's Heart Disease; Tintinalli's Emergency Medicine
11. Carotid Sinus Hypersensitivity (Carotid Sinus Syndrome)
Definition
An exaggerated baroreceptor response to carotid sinus stimulation producing:
- Asystole ≥ 3 seconds, OR
- Fall in systolic BP ≥ 50 mmHg, OR
- Both - in a patient with unexplained dizziness or syncope
Subtypes
| Type | Feature |
|---|---|
| Cardioinhibitory (~75%) | Pronounced bradycardia/asystole |
| Vasodepressor (~10%) | Drop in BP ≥50 mmHg without significant bradycardia |
| Mixed (~15%) | Both components |
Demographics
- More common in older men
- Associated with: hypertension, ischemic heart disease, head and neck malignancy
- History: syncope triggered by neck pressure, tight collar, turning the head, shaving, or swallowing
Diagnosis
Carotid sinus massage (CSM):
- Patient supine, continuous ECG and BP monitoring
- Longitudinal massage for 5 seconds at right carotid sinus (between superior thyroid cartilage and angle of mandible)
- Contraindications: recent stroke/TIA, carotid bruits, known carotid stenosis - risk of plaque embolization
- Ultrasound of carotid recommended before CSM in patients >50 years
Treatment
- Cardioinhibitory type: dual-chamber pacemaker (most effective)
- Vasodepressor type: responds poorly to pacing; managed with compression stockings, fludrocortisone
- Surgical denervation in refractory cases
Bradley and Daroff's Neurology in Clinical Practice; Tintinalli's Emergency Medicine
12. Diving Reflex (Mammalian Diving Reflex)
Trigger
Simultaneous apnea + cold-water facial immersion (the trigeminal cold receptors of the face are critical - submersion alone without facial cold water attenuates the response).
Response - Triad of Oxygen-Conservation:
- Bradycardia - reduces myocardial O₂ consumption dramatically
- Peripheral vasoconstriction - shunts blood away from muscles/skin toward vital organs (heart, brain)
- Splenic contraction - ejects stored red blood cells into circulation, increasing oxygen-carrying capacity
Mechanism
Cold trigeminal receptors (CN V, ophthalmic branch) → medullary cardiovascular center → increased vagal output → bradycardia; simultaneous sympathetic activation → peripheral vasoconstriction.
Clinical Relevance
- Used therapeutically to terminate SVT (ice water facial immersion - especially in infants/children; "diving reflex maneuver")
- Protective role in cold-water drowning - particularly in children (preserves cerebral and cardiac perfusion, explains occasional survival after prolonged submersion in cold water)
- Elite free-divers exploit this reflex: genetic adaptation in populations like the Bajau ("sea nomads") includes enlarged spleen and modified dive response
Braunwald's Heart Disease; Murray & Nadel's Respiratory Medicine; Rosen's Emergency Medicine
13. Chemoreceptor Reflex - Extended Detail
Central Chemoreceptors
Located in the retrotrapezoid nucleus of the medulla (and other medullary sites). They respond to:
- Rising CO₂ / falling pH in the CSF
- More potent respiratory drive than peripheral chemoreceptors
- No direct cardiac effect - act primarily on respiratory pattern generator
Peripheral Chemoreceptors
Carotid and aortic bodies - as covered previously. Their cardiac effects:
- At moderate hypoxia: ↑ vagal tone → bradycardia + ↓ contractility (pure chemoreceptor response)
- In intact person: hypoxia also stimulates breathing → lung inflation activates pulmonary stretch receptors → secondary tachycardia overrides primary bradycardia
- In severe/persistent hypoxia: direct CNS stimulation → sympathetic override → tachycardia, ↑ BP
Interaction with Baroreceptors
The two systems normally cooperate. During hypoxia with intact respiration: the respiratory response (hyperventilation, lung inflation) feeds back to inhibit the cardiac-slowing component, so the net result is often tachycardia rather than bradycardia in an awake patient.
Miller's Anesthesia 10e; Ganong's Review of Medical Physiology 26e
14. Bezold-Jarisch Reflex - Clinical Extensions
| Clinical Scenario | Mechanism | Clinical Manifestation |
|---|---|---|
| Inferior MI | RCA ischemia activates posterior LV C-fibers (highest receptor density there) | Bradycardia + hypotension (Bezold-Jarisch often worsens inferior MI hemodynamics) |
| Thrombolysis/PCI reperfusion | Sudden washout of ischemic metabolites re-activates receptors | Post-reperfusion bradycardia and hypotension |
| Spinal anesthesia | High sympathetic block → paradoxical LV vigorous contraction with low filling | Bradycardia + sudden hypotension |
| Contrast injection (coronary) | Chemical activation of ventricular receptors | Transient bradycardia |
| Upright syncope (vasovagal) | Vigorous LV contraction on low volume activates C-fibers | Vasovagal collapse |
The Bezold-Jarisch reflex explains why inferior MI is more likely to cause bradycardia and hypotension than anterior MI - the inferior wall has the densest population of ventricular C-fiber afferents.
Miller's Anesthesia 10e
15. Reflex Cardiac Arrhythmias (Neurally-Mediated)
Beyond syncope, autonomic reflexes can precipitate direct arrhythmias:
| Arrhythmia | Reflex Mechanism |
|---|---|
| Sinus bradycardia | Excessive vagal tone (vasovagal, Bezold-Jarisch, diving reflex, oculocardiac) |
| AV block (transient) | Intense vagal surge (oculocardiac, vasovagal in cardioinhibitory type) |
| Asystole | Extreme vagal activation (carotid sinus hypersensitivity, severe vasovagal) |
| Reflex tachycardia | Baroreceptor unloading (hypovolemia, vasodilation), Bainbridge reflex |
| VF (rare) | Intense sympathetic surges (Cushing reflex, pheochromocytoma, subarachnoid hemorrhage) |
Subarachnoid hemorrhage produces massive sympathetic discharge that can cause catecholamine-induced myocardial injury (neurogenic stunned myocardium / Takotsubo-like pattern) and life-threatening arrhythmias - an extreme form of neurocardiogenic interaction.
Bradley and Daroff's Neurology in Clinical Practice; Braunwald's Heart Disease
Integrated Overview: Hierarchy of Cardiac Reflex Control
FASTEST (milliseconds-seconds)
↓
Baroreceptor reflex — beat-to-beat pressure buffering
Chemoreceptor reflex — hypoxia/acidosis response
Bainbridge reflex — volume-to-rate matching
Bezold-Jarisch reflex — ventricular protection
Oculocardiac / Diving / Cushing — organ-specific reflexes
↓
SLOWER (seconds-minutes)
↓
Low-pressure / Cardiopulmonary reflex — volume regulation (renal arm)
Vasovagal syncope — pathological amplification of normal reflexes
RAAS, ADH, ANP — humoral extensions of reflex arcs
↓
SLOWEST (hours-days)
↓
Baroreceptor set-point resetting (chronic hypertension)
All these reflexes share a common final pathway: modulation of the SA node (heart rate), AV node (conduction), ventricular contractility, and vascular tone through the balance of sympathetic and parasympathetic outflow - orchestrated by the medullary cardiovascular centers.
I did not get the first part only.
Here is the first part again in full:
Cardiac Reflexes
Cardiac reflexes are autonomic feedback mechanisms that regulate heart rate, contractility, and arterial blood pressure in response to sensory inputs from receptors located in the heart, great vessels, and other organs. They operate through reflex arcs: receptor → afferent nerve → medullary cardiovascular center → efferent nerve → effector (heart/vessels).
1. Baroreceptor Reflex (Carotid Sinus / Aortic Arch Reflex)
This is the primary, best-known cardiac reflex for short-term blood pressure regulation.
Receptors
Baroreceptors are spray-type mechanoreceptors (stretch receptors) located in:
- Carotid sinus - the dilated portion of the internal carotid artery just above the carotid bifurcation
- Aortic arch - respond mainly to increases in pressure (less sensitive to hypotension than carotid sinus receptors)
They are most sensitive to rapid changes in pressure rather than a static level.
Afferent Pathway
| Location | Nerve |
|---|---|
| Carotid sinus | Hering's nerve → Glossopharyngeal nerve (CN IX) |
| Aortic arch | Vagus nerve (CN X) |
Both pathways converge on the nucleus tractus solitarius (NTS) in the medullary cardiovascular center.
Central Processing
The NTS is the primary relay. It projects to two functionally distinct medullary areas:
- Lateral rostral area - raises blood pressure (sympathoexcitatory)
- Central caudal area - lowers blood pressure (sympathoinhibitory); also integrates input from hypothalamus and limbic system
Efferent Response to Hypertension (↑ BP)
- Increased baroreceptor firing → NTS activation
- ↓ Sympathetic outflow: decreased heart rate, contractility, arteriolar and venous tone
- ↑ Parasympathetic (vagal) outflow: further decreases heart rate and contractility
- Net result: ↓ HR, ↓ CO, ↓ TPR → ↓ BP
Efferent Response to Hypotension (↓ BP)
- Decreased baroreceptor firing → reduced NTS inhibition of sympathetic centers
- ↑ Sympathetic outflow: increased HR, contractility, arteriolar vasoconstriction, venous constriction (reduces unstressed volume, increases venous return)
- ↓ Parasympathetic outflow: further increases HR
- Net result: ↑ HR, ↑ CO, ↑ TPR → ↑ BP
Key Points
- Baroreceptors are not stimulated below 50-60 mmHg; maximal activity around 180 mmHg (carotid); aortic baroreceptors operate ~30 mmHg higher
- The reflex is most sensitive in the normal operating range (~100 mmHg)
- They respond more to rate of pressure change than to absolute pressure
- In chronic hypertension, the set point is "reset" upward - the reflex maintains the elevated pressure rather than correcting it
- Volatile anesthetics (especially halothane) inhibit the heart rate component of this reflex
- Ca²⁺-channel blockers, ACE inhibitors, and phosphodiesterase inhibitors reduce the baroreceptor-mediated pressor response
- Loses functional capacity when BP falls below 50 mmHg
Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology 7e; Miller's Anesthesia 10e
2. Chemoreceptor Reflex
Receptors
Peripheral chemoreceptors are located in the:
- Carotid bodies (at the carotid bifurcation)
- Aortic body
They respond to:
- PaO₂ < 50 mmHg (hypoxia)
- Acidosis (↓ pH)
- Elevated PaCO₂
Afferent Pathway
- Carotid bodies → sinus nerve of Hering → glossopharyngeal nerve (CN IX)
- Aortic body → vagus nerve (CN X)
- Both converge on the chemosensitive area of the medulla
Response
- Stimulation of respiratory centers → increased ventilatory drive (primary response)
- Activation of parasympathetic system → ↓ heart rate and ↓ myocardial contractility (pure cardiac response)
- In persistent hypoxia: direct CNS stimulation → ↑ sympathetic activity overrides the initial bradycardia
Important Interaction
In an intact, awake patient with normal lungs, hypoxia triggers hyperventilation → lung inflation activates pulmonary stretch receptors → secondary tachycardia. So the net observed cardiac response to hypoxia is usually tachycardia, not bradycardia, in clinical practice.
Miller's Anesthesia 10e; Ganong's Review of Medical Physiology 26e
3. Bainbridge Reflex (Atrial Reflex / Volume Reflex)
Trigger
Increased right-sided filling pressure (e.g., rapid IV fluid infusion, increased venous return).
Receptor & Pathway
- Stretch receptors in the right atrial wall and cavoatrial junction
- Afferents travel via the vagus nerve to the medullary cardiovascular center
- Efferent limb: both parasympathetic (withdrawal) and sympathetic (activation) to the SA node
Response
- Inhibition of parasympathetic outflow + activation of sympathetic outflow → tachycardia
- Direct mechanical stretch of the SA node also contributes (~15% of the HR increase)
- The Bainbridge neural reflex accounts for 40-60% of the HR increase
- The net HR change depends on baseline heart rate - greatest when the baseline HR is slow
Physiologic Role
Prevents blood from pooling in the venous circulation. When more blood returns to the heart, the heart speeds up to pump it out - matching output to input. Important during exercise and volume loading.
Guyton and Hall; Medical Physiology (Boron & Boulpaep); Miller's Anesthesia 10e
4. Bezold-Jarisch Reflex
Trigger
Noxious stimuli within the left ventricular wall - activation of ventricular chemoreceptors and mechanoreceptors by:
- Myocardial ischemia or infarction
- Reperfusion/thrombolysis/revascularization
- Certain drugs (veratrum alkaloids, serotonin, capsaicin)
- Excessive ventricular mechanoreceptor stretch (e.g., low-volume vigorous contraction)
Receptor & Pathway
- Unmyelinated type C vagal afferents in the LV wall
- Signals travel to medulla via vagus nerve
- Efferent: increased parasympathetic tone
Response - Classic Triad:
- Bradycardia
- Hypotension (peripheral vasodilation)
- Coronary artery dilation
Clinical Significance
- Considered a cardioprotective reflex - reduces myocardial oxygen demand during ischemia
- Inferior MI causes more pronounced Bezold-Jarisch activation (inferior wall has the highest ventricular C-fiber density) - explaining the bradycardia and hypotension more common with inferior than anterior MI
- Implicated in syncope (vasovagal episodes), post-reperfusion bradycardia, and hypotension during spinal anesthesia
- Natriuretic peptides (ANP, BNP) modulate this reflex; less pronounced in cardiac hypertrophy and atrial fibrillation
Miller's Anesthesia 10e
5. Cushing Reflex (CNS Ischemic Response)
Trigger
Raised intracranial pressure (ICP) → cerebral ischemia → CO₂ and acid accumulation at the medullary vasomotor center.
Response - Cushing's Triad:
- Hypertension (powerful sympathetic activation; BP can rise to 250 mmHg)
- Bradycardia (baroreceptor-mediated reflex in response to the hypertension)
- Irregular/slow respirations
Mechanism
Cerebral ischemia at the vasomotor center → local CO₂ buildup + lactic acidosis → intense sympathetic activation → severe hypertension → baroreceptor-mediated reflex bradycardia. The bradycardia here is secondary - it is the baroreceptor response to the Cushing-driven hypertension, not a direct effect.
Role and Threshold
- Operates only when BP falls below ~60 mmHg (cerebral perfusion threatened)
- Does NOT function as a normal BP regulator
- Functions as a "last-ditch" emergency mechanism to maintain cerebral perfusion
- The specific form triggered by raised CSF pressure compressing cerebral arteries is the Cushing reaction (Cushing response to raised ICP)
Guyton and Hall Textbook of Medical Physiology; Miller's Anesthesia 10e
6. Oculocardiac Reflex
Trigger
- Pressure applied to the globe of the eye
- Traction on extraocular muscles or periorbital structures
- Most common during strabismus surgery (especially in children) and orbital blow-out fracture repair
Receptor & Afferent Pathway
- Stretch receptors in extraocular muscles
- Short and long ciliary nerves → nasociliary nerve → ophthalmic division (CN V₁) → trigeminal ganglion → trigeminal nerve (CN V) - this is the afferent limb
Efferent Pathway
- Dorsal motor nucleus of vagus → vagus nerve (CN X) → SA node
Response
- Bradycardia (can be severe and sudden)
- Nausea, vomiting
- Hypotension
- In severe cases: AV block, ventricular ectopy, ventricular fibrillation, asystole
Clinical Management
- Prevention: retrobulbar or peribulbar block interrupts the afferent limb; IV atropine or glycopyrrolate prophylactically before surgery
- Treatment: immediately release/stop ocular traction; if bradycardia persists, give IV atropine
- More pronounced in: children, hypoxia, hypercapnia, light planes of anesthesia, halothane anesthesia
Miller's Anesthesia 10e; Barash Clinical Anesthesia 9e
7. Valsalva Maneuver - Cardiovascular Reflex Responses
Forced expiration against a closed glottis produces a stereotyped four-phase sequence:
| Phase | Event | Mechanism | Heart Rate / BP |
|---|---|---|---|
| I (onset of strain) | ↑ intrathoracic pressure compresses aorta | Mechanical | Brief ↑ BP |
| II (sustained strain) | ↓ venous return → ↓ CO → ↓ BP | Baroreceptors detect ↓ BP | ↑ HR, ↑ TPR |
| III (release) | ↓ intrathoracic pressure, transient venous pooling | Mechanical | Brief ↓ BP |
| IV (recovery) | ↑ venous return → ↑ CO → BP overshoots | Baroreceptors detect ↑ BP | Reflex bradycardia |
The Phase IV bradycardia (reflex slowing after the overshoot) is a baroreceptor-mediated parasympathetic response. Its absence indicates autonomic neuropathy or baroreceptor dysfunction - used diagnostically in diabetes, Parkinson's disease, and other autonomic disorders.
Miller's Anesthesia 10e
Summary Table
| Reflex | Trigger | Receptor Site | Afferent | Net Response |
|---|---|---|---|---|
| Baroreceptor | ↑/↓ arterial pressure | Carotid sinus, aortic arch | CN IX, CN X → NTS | Opposes BP change (negative feedback) |
| Chemoreceptor | Hypoxia, acidosis | Carotid/aortic bodies | CN IX, CN X | ↑ ventilation; ↓ HR (pure); ↑ HR (clinical) |
| Bainbridge | ↑ venous return / atrial filling | RA wall, cavoatrial junction | Vagal afferents | Tachycardia |
| Bezold-Jarisch | LV noxious stimuli (ischemia) | LV wall C-fibers | Vagal C-fibers | Bradycardia + hypotension + coronary dilation |
| Cushing | ↑ ICP → cerebral ischemia | Medullary vasomotor center | Direct CO₂ effect | Hypertension + reflex bradycardia |
| Oculocardiac | Ocular pressure/traction | Extraocular muscle receptors | CN V → CN X | Bradycardia, arrhythmia |
| Valsalva | Forced expiration | Baroreceptors (Phase II & IV) | CN IX, CN X | Phase II tachycardia; Phase IV bradycardia |
This is a shared conversation. Sign in to Orris to start your own chat.