Stroke
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"stroke" AND "management"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative content from Harrison's 22e, Bradley & Daroff's Neurology, Rosen's Emergency Medicine, and Adams & Victor's. Here is the full, structured overview of stroke:
Stroke - A Comprehensive Overview
Definition
A stroke (cerebrovascular accident, CVA) is the sudden onset of a focal neurological deficit caused by disruption of blood supply to the brain. It is the second leading cause of death worldwide and the leading cause of adult disability.
Classification
Strokes fall into two broad categories:
| Type | Frequency | Mechanism |
|---|---|---|
| Ischemic stroke | ~87% | Arterial occlusion (thrombotic or embolic) |
| Hemorrhagic stroke | ~13% | Vessel rupture (ICH or SAH) |
TIA (Transient Ischemic Attack): Historically defined as a focal deficit lasting <24 hours; now tissue-based - a transient episode of neurological dysfunction caused by focal ischemia WITHOUT evidence of infarction on imaging. TIA has a high short-term stroke risk and warrants urgent evaluation.
Pathophysiology
Ischemic Stroke
When cerebral blood flow (CBF) falls acutely:
- Normal CBF: 40-60 mL/100 g brain/min
- Below 16-18 mL/100 g/min: neurons become electrically silent but remain viable - this is the ischemic penumbra (salvageable)
- Below 10 mL/100 g/min: membrane failure, influx of extracellular K⁺ and intracellular Ca²⁺, irreversible infarct core forms within 4-10 minutes
The ischemic penumbra is the primary therapeutic target. Collateral blood flow from surrounding vessels temporarily sustains this zone. Duration of occlusion is the critical determinant of neuronal survival - hence the motto "time is brain."
The cascade of ischemia involves glutamate excitotoxicity, oxidative stress, inflammation, and ultimately apoptosis and necrosis.
Hemorrhagic Stroke (ICH)
Acute vessel rupture causes a hematoma that:
- Directly compresses/destroys surrounding tissue
- Causes progressive perihematomal edema
- Raises intracranial pressure (ICP)
The two main causes of spontaneous ICH are hypertensive vasculopathy (lipohyalinosis of deep penetrating arteries) and cerebral amyloid angiopathy (CAA, affects lobar vessels, typically in the elderly).
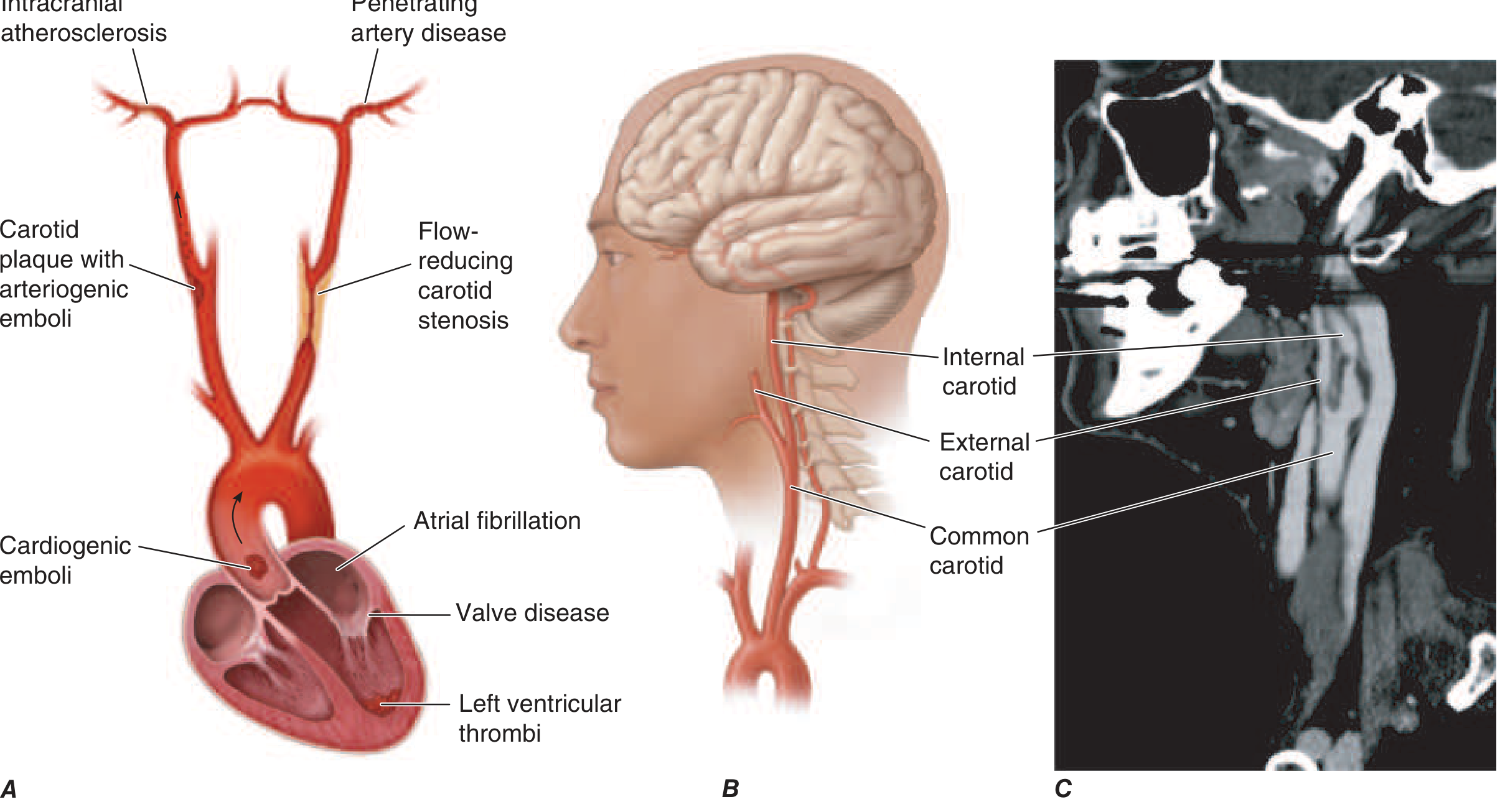
Etiology of Ischemic Stroke
Three core mechanisms (Harrison's 22e):
- Embolism - from cardiac sources (atrial fibrillation, mural thrombus, valvular disease) or artery-to-artery (carotid plaque)
- In situ thrombosis - of large or small (lacunar) intracranial vessels, often on atherosclerotic plaque
- Hypoperfusion - flow-limiting stenosis causing watershed ischemia
Common Causes (Harrison's Table 438-2)
| Common Causes | Uncommon Causes |
|---|---|
| Lacunar (small vessel) stroke | Hypercoagulable disorders |
| Large-vessel thrombosis | Antiphospholipid syndrome |
| Cardioembolic (AFib, MI, valve disease) | Arterial dissection |
| Carotid bifurcation atherosclerosis | CADASIL |
| Aortic arch atherosclerosis | Moyamoya disease |
| Sickle cell disease | |
| Vasculitis |
Sites of Hypertensive ICH (Rosen's EM)
| Location | Frequency |
|---|---|
| Putamen | 44% |
| Other cortical areas | 25% |
| Thalamus | 13% |
| Cerebellum | 9% |
| Pons | 9% |
Risk Factors
Non-modifiable: Age, male sex, race (higher incidence in Black patients), family history, prior stroke/TIA
Modifiable:
- Hypertension (most important)
- Atrial fibrillation
- Diabetes mellitus
- Dyslipidemia
- Smoking
- Carotid atherosclerosis
- Obesity, physical inactivity
Clinical Features
Anterior Circulation (ICA, MCA, ACA territory)
- Contralateral hemiparesis/hemisensory loss (face and body)
- Aphasia (dominant hemisphere)
- Neglect (non-dominant hemisphere)
- Homonymous hemianopia
- Gaze deviation toward the lesion
Posterior Circulation (Vertebrobasilar territory)
- Ipsilateral cranial nerve deficits + contralateral hemiparesis (crossed signs)
- Vertigo, diplopia, ataxia, dysarthria
- Wallenberg syndrome (lateral medullary stroke): vertigo, Horner syndrome, ipsilateral facial numbness + loss of corneal reflex, contralateral loss of pain/temperature
- PCA stroke: homonymous hemianopia, alexia without agraphia
Lacunar Syndromes (pure small-vessel disease)
- Pure motor hemiplegia (posterior limb of internal capsule/pons)
- Pure sensory stroke (thalamus)
- Ataxic hemiparesis
- Dysarthria-clumsy hand syndrome
Hemorrhagic Stroke
Classic presentation: sudden onset severe headache ("worst headache of life" in SAH), vomiting, markedly elevated BP, and focal deficits that progress over minutes to hours - distinguishes ICH from ischemic stroke (which is typically maximal at onset).
NIHSS (National Institutes of Health Stroke Scale)
Scored 0-42; assesses LOC, gaze, visual fields, facial palsy, motor arm/leg, ataxia, sensory, language, dysarthria, extinction. Score >15 indicates large infarction.
Diagnosis
Initial Workup
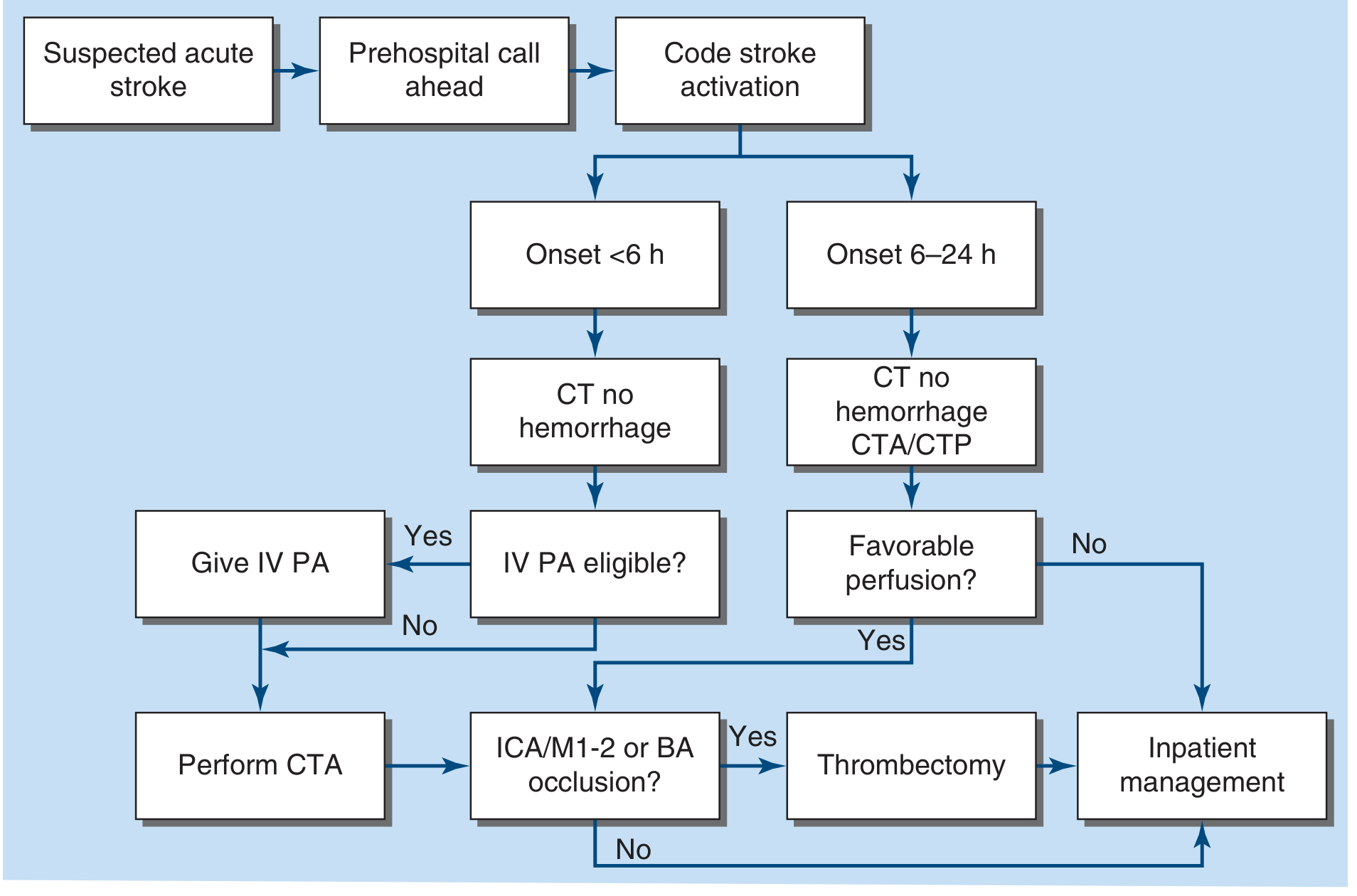
- Non-contrast CT head - first-line; immediately identifies hemorrhage, excludes ICH before thrombolysis. Ischemic changes appear 6-12 hours after onset
- CT Angiography (CTA) - identifies large vessel occlusion (LVO), carotid stenosis, dissection; guides thrombectomy decision
- CT Perfusion (CTP) - identifies penumbra vs. core in extended time windows (6-24 h)
- MRI/DWI - most sensitive for early ischemia; preferred for posterior fossa strokes
- ECG + troponin - concurrent myocardial ischemia in 3-20% of stroke patients; cardiac monitoring ≥48 hours to detect paroxysmal AFib
- Labs: CBC, PT/INR, aPTT, glucose, BMP
Early CT signs of ischemia: hyperdense artery sign, loss of insular ribbon, loss of gray-white differentiation, sulcal effacement
Acute Management
Acute Ischemic Stroke
General (ABCs):
- Airway protection; maintain O₂ sat >94%
- Treat fever aggressively (worsens ischemic outcome)
- Glucose: maintain 60-180 mg/dL; avoid hypoglycemia and hyperglycemia
- BP: do not lower unless >220/120 mmHg (or >185/110 mmHg if giving tPA)
- Head of bed >30° (aspiration prevention); NPO until swallow assessment
- Pneumatic compression stockings for DVT prophylaxis
- Cardiac monitoring ≥48 hours
IV Thrombolysis (tPA / Alteplase):
- Dose: 0.9 mg/kg IV (max 100 mg); 10% as bolus, remainder over 60 minutes
- Window: ≤4.5 hours from symptom onset (for otherwise eligible patients with disabling symptoms)
- Requires BP <185/110 mmHg before administration
- Risk of symptomatic ICH: 2-7%
- Tenecteplase is an alternative (single bolus; equal or superior efficacy in some settings)
- Goal door-to-needle: ≤60 minutes (target ≤45 min)
Endovascular Thrombectomy (EVT):
- Indicated for large vessel occlusion (ICA, M1-M2, basilar artery)
- Window: up to 24 hours from last known well with favorable perfusion imaging (DAWN/DEFUSE-3 trial criteria)
- Most effective treatment for LVO; NIHSS-guided selection
- Combine with IV tPA when both eligible
Antithrombotic:
- Aspirin 160-325 mg within 24-48 hours (not within 24 h of tPA)
- Dual antiplatelet therapy (aspirin + clopidogrel or ticagrelor) for 21-30 days for minor non-cardioembolic stroke / high-risk TIA (then aspirin alone)
Hemorrhagic Stroke (ICH)
Blood pressure control: Systolic BP reduction to <140 mmHg within 1 hour (if BP 150-220 mmHg) is safe and may limit hematoma expansion
Reversal of anticoagulation:
- Warfarin: Prothrombin complex concentrate (PCC) preferred over FFP (faster INR correction, lower volume, lower infection risk) + Vitamin K
- Dabigatran: Idarucizumab
- Factor Xa inhibitors: Andexanet alfa
Surgical: Hematoma evacuation for cerebellar hemorrhage >3 cm or patients with hydrocephalus; decompressive craniectomy for malignant MCA infarction
ICP management: Head of bed 30°, osmotic therapy (mannitol, hypertonic saline), hyperventilation as temporizing measure
Secondary Prevention
Antiplatelet therapy: Aspirin 75-100 mg/day (non-cardioembolic stroke); dual antiplatelet short-term for TIA/minor stroke
Anticoagulation: Oral anticoagulants (DOACs preferred over warfarin) for cardioembolic stroke due to AFib
- Apixaban 5 mg BID (reduced dose 2.5 mg BID if impaired renal function)
- Timing: generally start within 2-14 days depending on stroke size and hemorrhagic risk
Carotid revascularization:
- Symptomatic carotid stenosis ≥50-70%: carotid endarterectomy (CEA) is first-line, ideally within 2 weeks
- Intracranial stenting reserved for recurrent stroke despite optimal medical therapy
Risk factor control:
- BP: target <130/80 mmHg
- Statin therapy (LDL lowering): all ischemic stroke patients
- Glucose control in diabetics
- Smoking cessation, weight management, physical activity
Complications
- Brain edema (peaks day 2-3, up to 10 days) - greatest risk in large MCA infarctions and young patients
- Hemorrhagic transformation of ischemic stroke
- Aspiration pneumonia (15-25% mortality; swallowing assessment mandatory)
- Post-stroke seizures and epilepsy (16-17x increased risk vs. general population; higher with cortical and hemorrhagic strokes)
- DVT/PE
- Cardiac arrhythmias (particularly AFib discovered after stroke)
- Post-stroke depression (~30% of patients)
Rehabilitation
Early mobilization and stroke unit care are associated with lower mortality, shorter hospital stay, and reduced discharge to nursing home. Rehabilitation involves:
- Speech therapy (aphasia, dysphagia)
- Physical therapy (motor recovery)
- Occupational therapy (ADLs)
- Psychological support
Neuroplasticity allows significant recovery, particularly in the first 3-6 months post-stroke.
Sources: Harrison's Principles of Internal Medicine 22e (2025), Bradley and Daroff's Neurology in Clinical Practice, Rosen's Emergency Medicine 9e, Adams and Victor's Principles of Neurology 12e.
Now make full ppt on this
Reading File
Reading File
Reading File
Running Command
Running Command
Writing File
Running Command
Reading File
Running Command
Running Command
Editing File
Searching Content
Searching Content
Reading File
Editing File
Running Command
The presentation was generated successfully. Here it is:
Stroke Comprehensive
Presentation · PPTX
What's inside (20 slides):
| # | Slide |
|---|---|
| 1 | Title Slide |
| 2 | Table of Contents (12 topics) |
| 3 | Definition & Epidemiology (stats cards + TIA note) |
| 4 | Classification - Ischemic vs. Hemorrhagic |
| 5 | Pathophysiology - Ischemic (CBF thresholds, penumbra, ischemic cascade) |
| 6 | Pathophysiology - Hemorrhagic (hypertensive vasculopathy, CAA, injury mechanism) |
| 7 | Etiology - TOAST Classification |
| 8 | Risk Factors (modifiable vs. non-modifiable) |
| 9 | Clinical Features - Vascular Territory Syndromes |
| 10 | Clinical Features - ICH vs. Ischemic comparison + NIHSS table |
| 11 | Diagnosis - Imaging Modalities (CT, CTA, CTP, MRI/DWI) |
| 12 | Diagnosis - Labs & Cardiac Workup + "Time is Brain" banner |
| 13 | Acute Management - General (ABCs: Airway, BP, Glucose, Temp) |
| 14 | Acute Management - IV Thrombolysis (tPA dosing, contraindications, tenecteplase) |
| 15 | Acute Management - Mechanical Thrombectomy (time windows, EVT criteria) |
| 16 | Acute Management - Hemorrhagic Stroke (BP control, reversal agents, surgery) |
| 17 | Secondary Prevention (antiplatelet, anticoagulation, carotid CEA, statins) |
| 18 | Complications (edema, hemorrhagic transformation, aspiration, seizures, DVT, depression) |
| 19 | Rehabilitation & Prognosis (PT/OT/ST, neuroplasticity, prognosis factors) |
| 20 | Key Takeaways (summary slide) |
Design: Deep navy + crimson red palette with teal accents, card-based layouts, section divider slides, and a consistent footer citing Harrison's 22e, Bradley & Daroff's, Rosen's EM, and Adams & Victor's.
This is a shared conversation. Sign in to Orris to start your own chat.