Hypochromic aemia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypochromic anemia" OR "iron deficiency anemia"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
hypochromic microcytic anemia peripheral blood smear iron deficiency
I have comprehensive content. Let me now compose a thorough, well-structured answer.
Hypochromic Anaemia
Hypochromic anaemia is characterised by red blood cells that are pale (hypochromic) due to a reduced mean corpuscular haemoglobin (MCH). It is almost always accompanied by microcytosis (low MCV) and reflects a quantitative defect in haemoglobin synthesis.
Blood Film Appearance
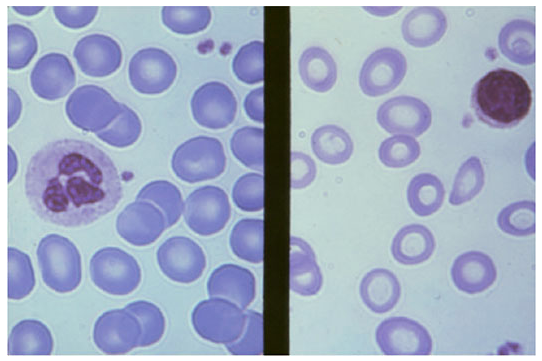
Left: Normal RBCs with small central pallor. Right: Iron deficiency — pale, small cells with markedly increased central pallor (hypochromia + microcytosis).
Causes
The four major causes of microcytic/hypochromic anaemia are:
| Cause | Key Feature |
|---|---|
| Iron deficiency anaemia (IDA) | Most common; depleted iron stores |
| Anaemia of inflammation (AI) | Also called anaemia of chronic disease; serum iron low but stores normal/high |
| Thalassaemia | Genetic globin chain synthesis defect; basophilic stippling, target cells |
| Sideroblastic anaemia | Ring sideroblasts in marrow; dimorphic film; may be acquired (drugs, lead) or inherited |
— Henry's Clinical Diagnosis and Management by Laboratory Methods; Goldman-Cecil Medicine
Iron Deficiency Anaemia — The Most Common Form
Definition
Iron deficiency occurs when body iron stores are insufficient to support iron metabolism. It can exist without anaemia (causing fatigue, alopecia, and tissue symptoms) or progress to a frank microcytic, hypochromic anaemia with further iron depletion. In functional iron deficiency, stores are adequate but cannot be mobilised for erythropoiesis.
Epidemiology
- Prevalence ~1–2% in men; much higher in women
- Menstruation causes average loss of 35 mL blood / 16 mg iron per cycle; iron requirements in women average 1–3 mg/day
- Bone marrow iron stores are absent in ~25% of healthy college-age women
- Pregnancy requires ~900 mg iron; requirements rise to 6 mg/day in the third trimester
- After menstruation, gastrointestinal (GI) bleeding is the second leading cause
- GI cancer (especially colon, gastric) found in up to 10% of older patients with IDA
- Higher incidence in developing countries (inadequate bioavailable dietary iron)
— Goldman-Cecil Medicine
Iron Physiology & Pathobiology
Dietary sources:
- Heme iron (meat, Fe²⁺): absorbed via a specific heme receptor at 30–40% efficiency
- Non-heme iron (plant-based, Fe³⁺): reduced by stomach acid to Fe²⁺, absorbed via divalent metal transporter 1 (DMT1) — far less efficient
Transport and storage:
- Absorbed iron is exported from enterocytes via ferroportin (SLC40A1) → binds transferrin (carries up to 2 iron atoms) → delivered to marrow transferrin receptors
- Excess iron stored in ferritin (24-subunit shell, stores up to 4,000 iron molecules) in liver and macrophages
- The iron recycling cycle is >95% efficient
Master regulator — Hepcidin:
- Liver-derived peptide that binds and degrades ferroportin
- When hepcidin is elevated (e.g. in inflammation): iron cannot be released from enterocytes or hepatocytes → iron-restricted erythropoiesis
- Iron deficiency and hypoxia suppress hepcidin → increase iron absorption
- Inflammation upregulates hepcidin → this is the mechanism behind anaemia of chronic disease
— Goldman-Cecil Medicine; Goodman & Gilman's Pharmacological Basis of Therapeutics
Causes of Iron Deficiency
- Blood loss — menstrual, GI (peptic ulcer, cancer, H. pylori, NSAIDs, IBD), haematuria
- Reduced absorption — coeliac disease, H. pylori-associated achlorhydria, gastrectomy, proton pump inhibitor use
- Increased requirements — pregnancy, infancy, adolescence
- Inadequate intake — vegetarian/vegan diets (non-heme iron less bioavailable)
Clinical Features
Symptoms of anaemia:
- Fatigue, dyspnoea on exertion, pallor, palpitations, headache
Specific to iron deficiency (tissue iron depletion):
- Koilonychia (spoon-shaped nails)
- Angular cheilitis and glossitis
- Pica (craving for non-food substances: ice [pagophagia], clay, starch)
- Alopecia
- Dysphagia (Plummer-Vinson / Patterson-Brown-Kelly syndrome: post-cricoid web)
Laboratory Investigations
The diagnostic table from Harrison's Principles of Internal Medicine summarises the key differentials:
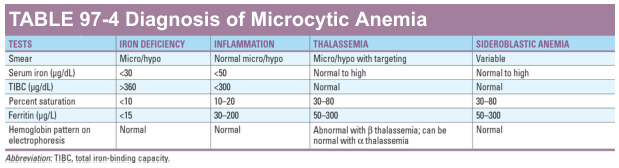
| Test | Iron Deficiency | Anaemia of Inflammation | Thalassaemia | Sideroblastic |
|---|---|---|---|---|
| Serum iron (µg/dL) | < 30 | < 50 | Normal–high | Normal–high |
| TIBC (µg/dL) | > 360 | < 300 | Normal | Normal |
| % Transferrin saturation | < 10% | 10–20% | 30–80% | 30–80% |
| Ferritin (µg/L) | < 15 | 30–200 | 50–300 | 50–300 |
| Hb electrophoresis | Normal | Normal | Abnormal (β-thal); may be normal (α-thal) | Normal |
Key points:
- Ferritin is the most sensitive and specific single test for IDA; < 15 µg/L is diagnostic
- Both IDA and AI have low serum iron — the difference is TIBC (elevated in IDA, low/normal in AI) and ferritin (low in IDA, normal/elevated in AI)
- Bone marrow biopsy showing absent Prussian-blue stainable iron is the gold standard but rarely needed
- If basophilic stippling is present with normal/high serum iron → suspect thalassaemia → check Hb electrophoresis, HbA₂, HbF, and family studies
- Ring sideroblasts on bone marrow Prussian blue → sideroblastic anaemia (consider isoniazid, lead, MDS)
Treatment
Iron Deficiency
Identify and treat the underlying cause (mandatory — especially in adult males and post-menopausal women where GI malignancy must be excluded).
Oral iron:
- Ferrous sulphate 325 mg (65 mg elemental iron) once or twice daily is first-line
- Vitamin C enhances absorption; milk, antacids, PPIs, and tannins reduce it
- Side effects: constipation, nausea, dark stools (common causes of non-compliance)
- Reticulocyte response begins within 3–5 days; haemoglobin normalises in 4–8 weeks
- Stores must be replenished: continue therapy for 3–6 months after Hb normalises
Intravenous iron:
Indicated when:
- Oral iron is not tolerated
- Malabsorption (coeliac disease, post-gastrectomy)
- Ongoing rapid blood loss exceeds oral replacement capacity
- Inflammatory bowel disease
- Renal failure on erythropoietin therapy
Formulations include ferric carboxymaltose, iron sucrose, and low-molecular-weight iron dextran. Note: ferric carboxymaltose can cause hypophosphatemia (a recognised complication per recent systematic reviews, PMID 39935027).
Anaemia of Chronic Disease / Inflammation
- Treat the underlying condition
- Intravenous iron if functional deficiency confirmed
- Erythropoiesis-stimulating agents (EPO) in selected cases (renal disease, chemotherapy)
Thalassaemia
- Genetic counselling; trait carriers are usually asymptomatic with mild microcytosis
- Do not give iron unless concurrent IDA is confirmed (iron supplementation is harmful in thalassaemia major)
- Severe forms require regular transfusions and iron chelation therapy
Sideroblastic Anaemia
- Pyridoxine (vitamin B₆) for hereditary/isoniazid-induced forms
- Remove offending drugs or toxins (lead chelation if lead poisoning)
- MDS-associated: supportive care ± disease-modifying therapy
Summary Algorithm
Hypochromic/microcytic anaemia (↓MCV, ↓MCH)
│
├─ Serum ferritin < 15 µg/L → IRON DEFICIENCY ANAEMIA
│ → Find cause (GI workup in adults)
│ → Oral/IV iron replacement
│
├─ Low serum iron + low TIBC + normal/↑ ferritin → ANAEMIA OF INFLAMMATION
│ → Treat underlying disease
│
├─ Normal/↑ serum iron + basophilic stippling → THALASSAEMIA
│ → Hb electrophoresis, HbA₂, HbF
│
└─ Ring sideroblasts on bone marrow → SIDEROBLASTIC ANAEMIA
→ Check drugs (INH, lead), consider MDS
Sources: Goldman-Cecil Medicine (Ch. 145); Henry's Clinical Diagnosis and Management by Laboratory Methods (Ch. 33); Goodman & Gilman's Pharmacological Basis of Therapeutics (Ch. 45); Harrison's Principles of Internal Medicine, 21st ed.
This is a shared conversation. Sign in to Orris to start your own chat.