Causes of vh
Reading File
search_medical_text
vitreous hemorrhage causes etiology
search_medical_image
vitreous hemorrhage fundus
GradeResponse
GradeResponse
Causes of Vitreous Hemorrhage (VH)
Vitreous hemorrhage occurs when blood enters the vitreous cavity. The causes are broadly categorized below:
Most Common Causes
| Cause | Key Details |
|---|---|
| Proliferative Diabetic Retinopathy (PDR) | #1 cause overall. Neovascularization on the retinal surface or disc bleeds into the vitreous. |
| Posterior Vitreous Detachment (PVD) | The vitreous pulls away from the retina, tearing a blood vessel. About 2/3 of VH cases with PVD have at least one retinal break; ~88% of breaks occur in the superior quadrants. |
| Retinal Breaks / Tears | A tear in the retina severs a retinal vessel. Often associated with PVD. Can progress to retinal detachment. |
| Retinal Vein Occlusion (BRVO/CRVO) | Venous occlusion leads to hemorrhagic infarction and neovascularization. |
| Sickle Cell Retinopathy | Peripheral neovascularization ("sea fan" pattern) prone to bleeding. |
Other Important Causes
Neovascular / Ischemic
- Retinal artery occlusion (with subsequent neovascularization)
- Ocular ischemic syndrome
- Radiation retinopathy
Traumatic
- Blunt or penetrating ocular trauma (most common cause in young patients)
- Terson syndrome: intracranial hemorrhage (e.g., subarachnoid hemorrhage) causing VH via sudden ICP rise
Retinal Detachment
- Rhegmatogenous retinal detachment with vessel rupture at the tear site
Vascular Anomalies
- Retinal macroaneurysm (especially in elderly hypertensive patients)
- Eales disease (idiopathic retinal vasculitis, young males)
- Coat's disease (telangiectatic vessels)
Neoplastic
- Choroidal melanoma or metastases breaking through the retina
- Retinoblastoma (in children)
Inflammatory / Infectious
- Proliferative vitreoretinopathy
- CMV retinitis, toxoplasmosis
Hematologic
- Anticoagulation therapy
- Thrombocytopenia, leukemia
Idiopathic
- Up to 10–17% of cases have no identifiable cause after workup
Image: Vitreous Hemorrhage on Fundus Photography
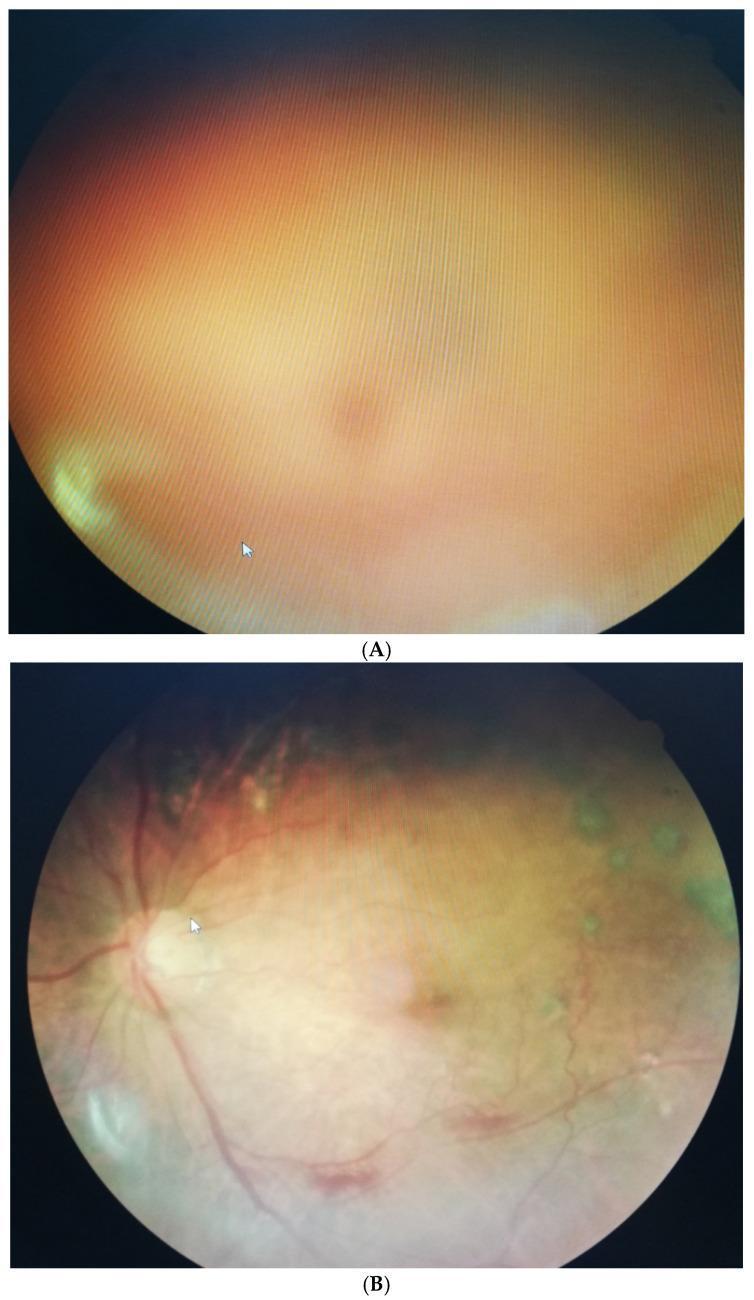
Left (A): Dense vitreous hemorrhage obscuring fundal view. Right (B): Significant clearing at 3 months in a 58-year-old diabetic male, with the optic disc and vessels now visible.
Key Points by Age Group
- Young patients: Trauma, sickle cell retinopathy, Eales disease
- Middle-aged: Diabetic retinopathy, retinal vein occlusion
- Elderly: PVD with retinal tear, macroaneurysm, AMD (wet type with subretinal neovascularization)
Source: Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration (p. 12)
Causes of VH & their management . Take reference from decision making in ophthalmology
search_medical_text
vitreous hemorrhage causes etiology decision making ophthalmology
search_medical_text
vitreous hemorrhage management treatment decision making ophthalmology
GradeResponse
GradeResponse
search_medical_text
vitreous hemorrhage diabetic retinopathy proliferative management anti-VEGF laser
search_medical_text
vitreous hemorrhage retinal tear PVD posterior vitreous detachment management observation
Causes of Vitreous Hemorrhage & Their Management
Primary reference: Decision Making in Ophthalmology; supplemented by Diabetic Retinopathy guidelines and Posterior Vitreous Detachment, Retinal Breaks & Lattice Degeneration.
Overview
Vitreous hemorrhage (VH) results from blood entering the vitreous cavity from any source: retinal vessels, neovascularization, or trauma. Management depends on the underlying etiology and whether the retina can be visualized.
1. Proliferative Diabetic Retinopathy (PDR) — Most Common Cause
Mechanism: Retinal ischemia → neovascularization → fragile new vessels rupture into vitreous.
Management
| Step | Intervention |
|---|---|
| Initial | Dilated exam + B-scan ultrasound (if fundus obscured) to rule out tractional/rhegmatogenous RD |
| Medical | Intravitreal Anti-VEGF (bevacizumab, ranibizumab, aflibercept) — first-line for persistent VH |
| Laser | Panretinal photocoagulation (PRP) — when media clears; destroys ischemic retina to regress NV |
| Surgical | Pars plana vitrectomy (PPV) — for nonclearing VH, tractional RD involving/threatening macula, combined traction-rhegmatogenous RD, dense premacular subhyaloid hemorrhage |
DRVS (Diabetic Retinopathy Vitrectomy Study): Early vitrectomy (within 1–6 months) yields better outcomes than late vitrectomy at 1 year (Diabetic Retinopathy guidelines, p. 40).
Pre-operative anti-VEGF (bevacizumab) before PPV reduces surgical duration, number of retinal breaks, intraoperative bleeding, and post-op VH (Cochrane review; Diabetic Retinopathy guidelines, p. 40).
2. Posterior Vitreous Detachment (PVD) with Retinal Break
Mechanism: Vitreous pulls away from retina → tears a bridging retinal vessel or creates a full-thickness retinal break.
- ~2/3 of VH with PVD have ≥1 retinal break
- ~88% of breaks are in superior quadrants
- 1/3 of those with breaks have multiple breaks (Posterior Vitreous Detachment, Retinal Breaks & Lattice Degeneration, p. 12)
Management
| Finding | Management |
|---|---|
| PVD + VH, no break seen | Serial observation; B-scan US to exclude break/RD; repeat exam as hemorrhage clears |
| PVD + retinal break, no RD | Laser retinopexy or cryotherapy to demarcate break |
| PVD + rhegmatogenous RD | Urgent PPV or scleral buckle ± vitrectomy |
| Nonclearing VH (>3 months) | PPV to clear vitreous and treat break |
3. Retinal Vein Occlusion (BRVO / CRVO)
Mechanism: Venous occlusion → retinal ischemia → neovascularization → VH.
Management
| Step | Intervention |
|---|---|
| Acute | Observation; intravitreal anti-VEGF or steroids for macular edema |
| Ischemic BRVO/CRVO with NV | Sector/panretinal laser photocoagulation |
| Nonclearing VH | PPV |
4. Trauma (Most Common Cause in Young Patients)
Mechanism: Direct vessel rupture from blunt or penetrating injury; associated with retinal tears, dialysis, or giant retinal tears.
Management
| Finding | Management |
|---|---|
| Blunt trauma + VH, no RD | B-scan US; observation; avoid anti-coagulants/aspirin; head elevation |
| Penetrating trauma | Urgent surgical exploration and PPV |
| Associated retinal break/RD | Prompt PPV ± scleral buckle |
5. Terson Syndrome
Mechanism: Rapid rise in intracranial pressure (e.g., subarachnoid hemorrhage) → vitreous/preretinal hemorrhage adjacent to optic nerve head (Abusive Head Trauma in Infants and Children, p. 12).
Management
- Treat underlying intracranial pathology (neurosurgical)
- Most VH resolves spontaneously over months
- PPV if VH is dense, nonclearing, or causing deprivation amblyopia (children)
6. Retinal Macroaneurysm
Mechanism: Arteriolar aneurysm ruptures → sub-/pre-retinal or vitreous hemorrhage, typically in elderly hypertensive patients.
Management
- Most resolve spontaneously; observation for 3–6 months
- Laser photocoagulation to the macroaneurysm if persistent or threatening macula
- PPV rarely needed for nonclearing VH
7. Sickle Cell Retinopathy
Mechanism: Peripheral vascular occlusion → "sea fan" neovascularization → VH.
Management
- Scatter laser (peripheral PRP) to sea fan lesions
- Anti-VEGF (adjunct)
- PPV for nonclearing VH — caution: high risk of iatrogenic breaks; avoid scleral buckle (can worsen sickling)
8. Wet AMD (Choroidal Neovascularization)
Mechanism: CNV breaks through RPE and retina → sub-/pre-retinal or vitreous hemorrhage.
Management
- Intravitreal anti-VEGF (bevacizumab, ranibizumab, aflibercept) — mainstay
- PPV for dense submacular hemorrhage with displacement techniques
9. Eales Disease
Mechanism: Idiopathic obliterative retinal vasculitis in young males → peripheral ischemia → NV → VH.
Management
- Systemic steroids (for active inflammation)
- Peripheral laser photocoagulation to ischemic retina
- PPV for nonclearing VH
General Algorithm for VH Management
Vitreous Hemorrhage
│
▼
B-scan ultrasound (if fundus not visible)
│
┌────┴────┐
RD present No RD
│ │
Urgent PPV Observation 4–6 weeks
+ treat underlying cause
│
VH clearing?
┌──────┴──────┐
Yes No (>3 months)
│ │
Treat cause PPV + treat cause
Key Surgical Indications for PPV in VH
- Nonclearing VH > 1–3 months
- Tractional or rhegmatogenous RD
- Dense premacular subhyaloid hemorrhage
- Only-seeing eye (earlier intervention)
- Young patients (earlier, to prevent amblyopia)
- Terson syndrome with amblyogenic VH
This is a shared conversation. Sign in to Orris to start your own chat.