Define and classify dead space Consequences of increase in dead space
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have excellent, comprehensive material from multiple authoritative textbooks. Here is the complete answer:
Dead Space: Definition, Classification, and Consequences
1. Definition
Dead space is the volume of the airways and lungs that does not participate in gas exchange. Each breath consists of two components:
- Alveolar ventilation (V_A): the portion reaching the alveoli and undergoing gas exchange
- Dead space ventilation (V_D): the portion that is "wasted" - it contributes nothing to CO₂ elimination or O₂ uptake
Normally, V_D = ~150 mL and V_T (tidal volume) = ~500 mL, so dead space constitutes ~1/3 of each tidal volume (V_D/V_T ≈ 0.3).
"Dead space is a general term that refers to both the anatomic dead space of the conducting airways and a functional, or physiologic, dead space." - Costanzo Physiology 7th Ed.
2. Classification of Dead Space
A. Anatomic Dead Space
The volume of gas filling the conducting airways - nose/mouth, pharynx, larynx, trachea, bronchi, and bronchioles up to (but not including) the respiratory bronchioles and alveoli. These structures have walls but no alveolar-capillary membrane for gas exchange.
- Normal value: ~150 mL in a healthy adult male (approximately 1 mL per pound of ideal body weight)
- Women generally have smaller anatomic dead space due to smaller airway caliber
- Increases slightly after age 50-60
- Measured by the Fowler method (single-breath nitrogen washout)
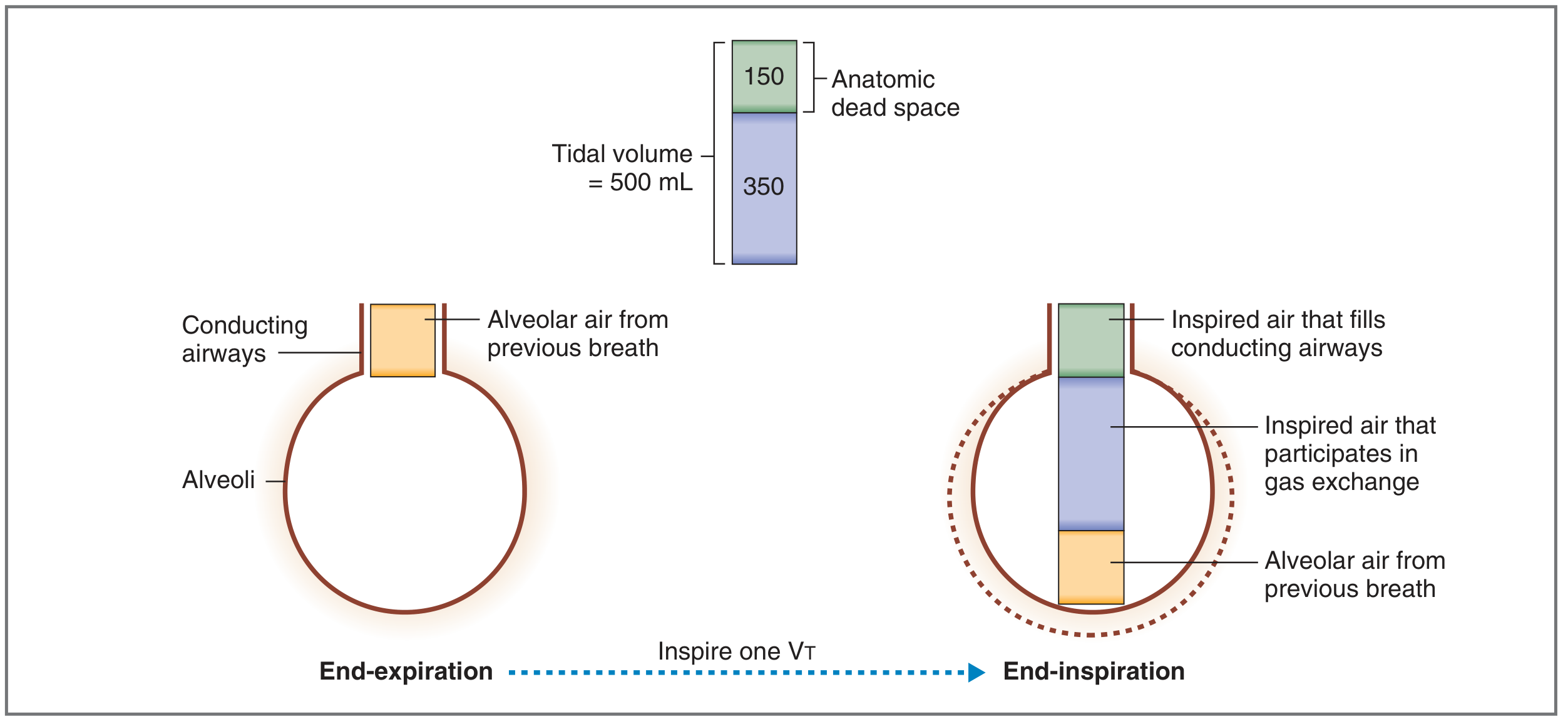
Key point on mechanics: At end-expiration, the conducting airways are filled with alveolar air from the previous breath. On the next inspiration, this old alveolar air enters the alveoli first - but undergoes no further gas exchange ("already been there, done that"). Only the fresh 350 mL from the new breath participates in gas exchange.
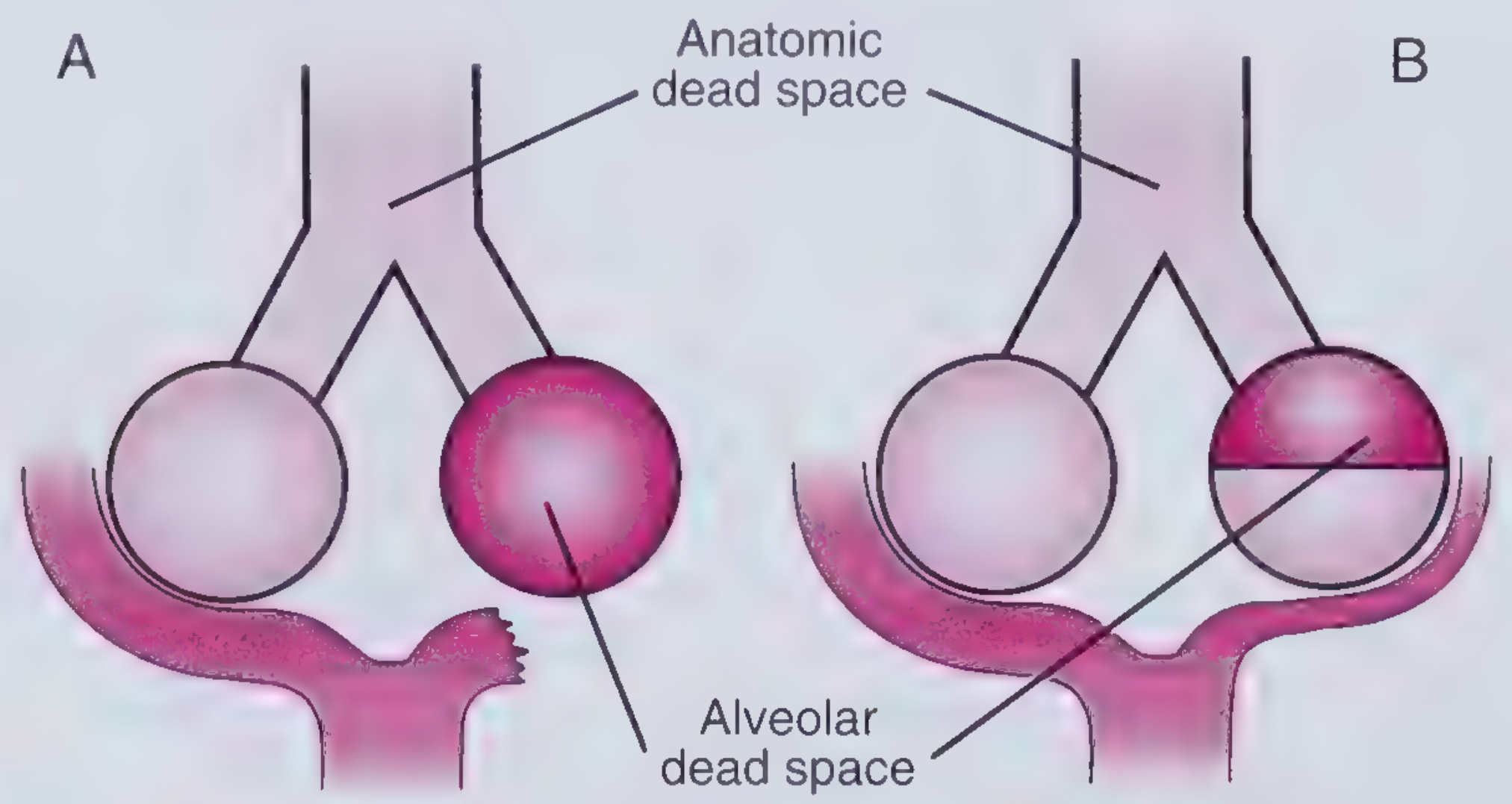
B. Alveolar Dead Space
The volume of gas reaching ventilated alveoli that are not perfused (or very poorly perfused) by pulmonary capillary blood. These alveoli have a V/Q ratio of infinity (ventilation without perfusion).
- Normal value: ~zero in healthy individuals
- Represents a pathological component
- Arises whenever alveolar perfusion is interrupted (e.g., pulmonary embolism)
C. Physiologic (Functional) Dead Space
Total dead space = the volume of the lung that does not participate in gas exchange, regardless of mechanism.
$$\boxed{V_D^{physiologic} = \text{Anatomic dead space} + \text{Alveolar dead space}}$$
- In normal persons: physiologic ≈ anatomic dead space (alveolar dead space ≈ 0)
- In disease: physiologic dead space can exceed anatomic dead space many times over (up to 10x, or 1-2 L) - Guyton & Hall
Measured by the Bohr equation using CO₂ as the marker gas:
$$V_D = V_T \times \frac{PaCO_2 - PE_{CO_2}}{PaCO_2}$$
Where:
- V_D = physiologic dead space
- V_T = tidal volume
- PaCO₂ = arterial PCO₂ (proxy for alveolar PCO₂)
- PE_CO₂ = PCO₂ of mixed expired air
The Bohr method detects alveolar dead space (e.g., in pulmonary embolism), while the Fowler nitrogen washout method measures only anatomic dead space. - Medical Physiology (Boron & Boulpaep)
D. Apparatus Dead Space (Additional Type)
Relevant in mechanically ventilated or anesthetized patients - the volume of the breathing circuit (mask, mouthpiece, tubing) that the patient must re-breathe. Can add up to 300 mL to the effective dead space. - Miller's Anesthesia 10e
Summary Table: Classification
| Type | Location | Normal Value | V/Q Ratio | Clinical Relevance |
|---|---|---|---|---|
| Anatomic | Conducting airways | ~150 mL | No perfusion (airways) | Baseline always present |
| Alveolar | Non-perfused alveoli | ~0 mL | ∞ (ventilated, not perfused) | Pathological |
| Physiologic | Total (anatomic + alveolar) | ~150 mL | - | Most clinically relevant measure |
| Apparatus | External breathing circuit | Variable (up to 300 mL) | - | Anesthesia/ventilation |
3. Consequences of Increased Dead Space
A. Reduced Alveolar Ventilation
Alveolar ventilation is:
$$\dot{V}_A = \text{Frequency} \times (V_T - V_D)$$
If dead space increases while minute ventilation (V_E) remains constant, effective alveolar ventilation falls. Using normal values: 12 breaths/min × (500 - 150) = 4,200 mL/min. If V_D rises to 300 mL with the same V_T, alveolar ventilation drops to 12 × 200 = 2,400 mL/min - a near-halving of effective gas exchange.
B. Hypercapnia (Elevated PaCO₂)
This is the primary and most direct consequence. CO₂ elimination is determined by alveolar ventilation:
$$\dot{V}A = k \times \frac{\dot{V}{CO_2}}{P_{ACO_2}}$$
As V_A falls, PaCO₂ rises. However, hypercapnia does not occur until dead space exceeds ~50% of total ventilation, because compensatory hyperventilation normally maintains PaCO₂:
- An increase in dead space stimulates minute ventilation via CO₂-sensitive chemoreceptors
- In healthy individuals with intact ventilatory reserve, PaCO₂ can be normalized even with large increases in dead space
- In patients with limited ventilatory reserve (severe COPD, neuromuscular disease), hypercapnia occurs at lower thresholds
"Patients with severe COPD may have a VD/VT ratio of up to 0.9 and would have to hyperventilate massively (30-50 L/min) to maintain normal PaCO₂, which is not possible where ventilator reserve is diminished." - Miller's Anesthesia 10e
C. Hypoxemia
Increased V/Q mismatch causing alveolar dead space also causes ventilation-perfusion inequality that reduces oxygenation. Blood from normally-perfused alveoli mixes with blood that has not undergone adequate gas exchange, lowering PaO₂.
- Hypoxemia from increased dead space generally responds to supplemental oxygen (unlike shunt, which responds poorly) - Frameworks for Internal Medicine
- Compensatory bronchoconstriction acts locally to normalize V/Q ratios in areas of increased dead space
D. Increased Work of Breathing and Dyspnea
To compensate for elevated dead space, the respiratory system must increase minute ventilation. This:
- Requires greater respiratory muscle effort
- Causes dyspnea, especially with exertion
- With pulmonary embolism, V_D/V_T can exceed 0.8, requiring a 2.7-fold increase in V_E (nearly 20 L/min) just to maintain normal alveolar ventilation
E. Widened PaCO₂ - EtCO₂ Gradient
Normally, end-tidal CO₂ (EtCO₂) closely approximates PaCO₂ (normal gradient < 5 mmHg). Increased alveolar dead space dilutes the exhaled CO₂ with dead space gas (which has no CO₂), causing:
- EtCO₂ to fall despite a normal or elevated PaCO₂
- Widened arterial-to-end-tidal CO₂ gradient (PaCO₂ - EtCO₂ gap)
- Used clinically as a marker of dead space - important in monitoring mechanical ventilation and suspecting pulmonary embolism
F. Clinical Examples by Etiology
| Cause | Mechanism | Dead Space Effect |
|---|---|---|
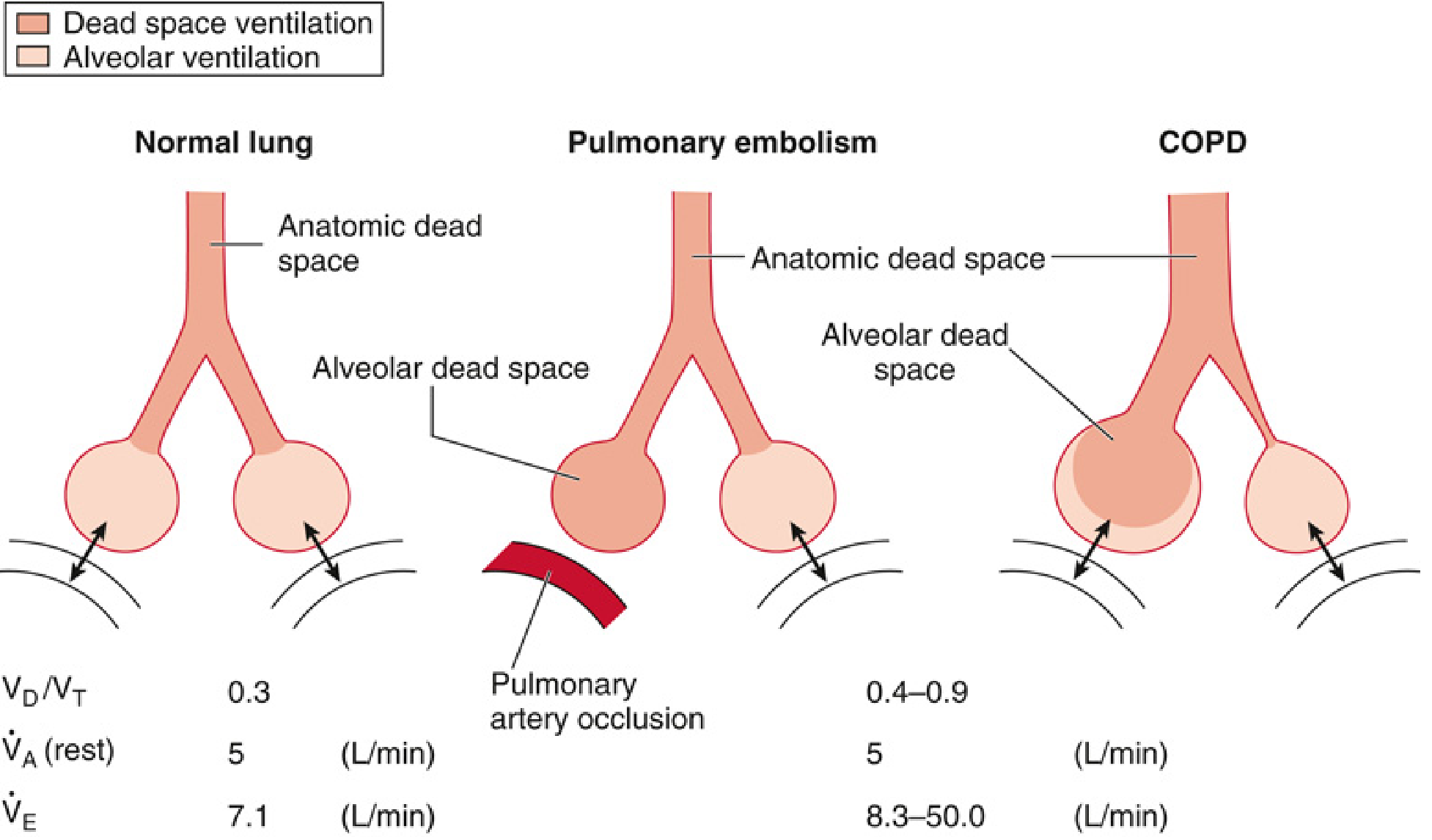
| Pulmonary embolism | Occlusion of pulmonary arteries | Large alveolar dead space; V_D/V_T can exceed 0.8 |
| COPD | High V/Q zones from airflow obstruction diverting air to poorly-perfused regions | V_D/V_T 0.4-0.9 |
| Rapid shallow breathing | Fixed anatomic dead space now a greater fraction of smaller V_T | Increased V_D/V_T ratio |
| Mechanical ventilation | Apparatus dead space + PEEP effects | Increased total dead space; guides ventilator management |
| Hypovolemia/low cardiac output | Reduced pulmonary perfusion pressure | More alveolar dead space |
Sources:
- Costanzo Physiology 7th Ed., pp. 199-200
- Guyton & Hall Textbook of Medical Physiology, pp. 498-499
- Murray & Nadel's Textbook of Respiratory Medicine, Chapters 45 & 46
- Miller's Anesthesia 10e, Chapter 12
- Fishman's Pulmonary Diseases and Disorders, Chapter on ventilation
- Medical Physiology (Boron & Boulpaep), Chapter 31
- Frameworks for Internal Medicine, Chapter 46
This is a shared conversation. Sign in to Orris to start your own chat.