Pulmonary edema
Reading File
Finding Sources
Searching PubMed
"pulmonary edema" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive, well-sourced response. Here is the full overview:
Pulmonary Edema
Definition and Pathophysiology
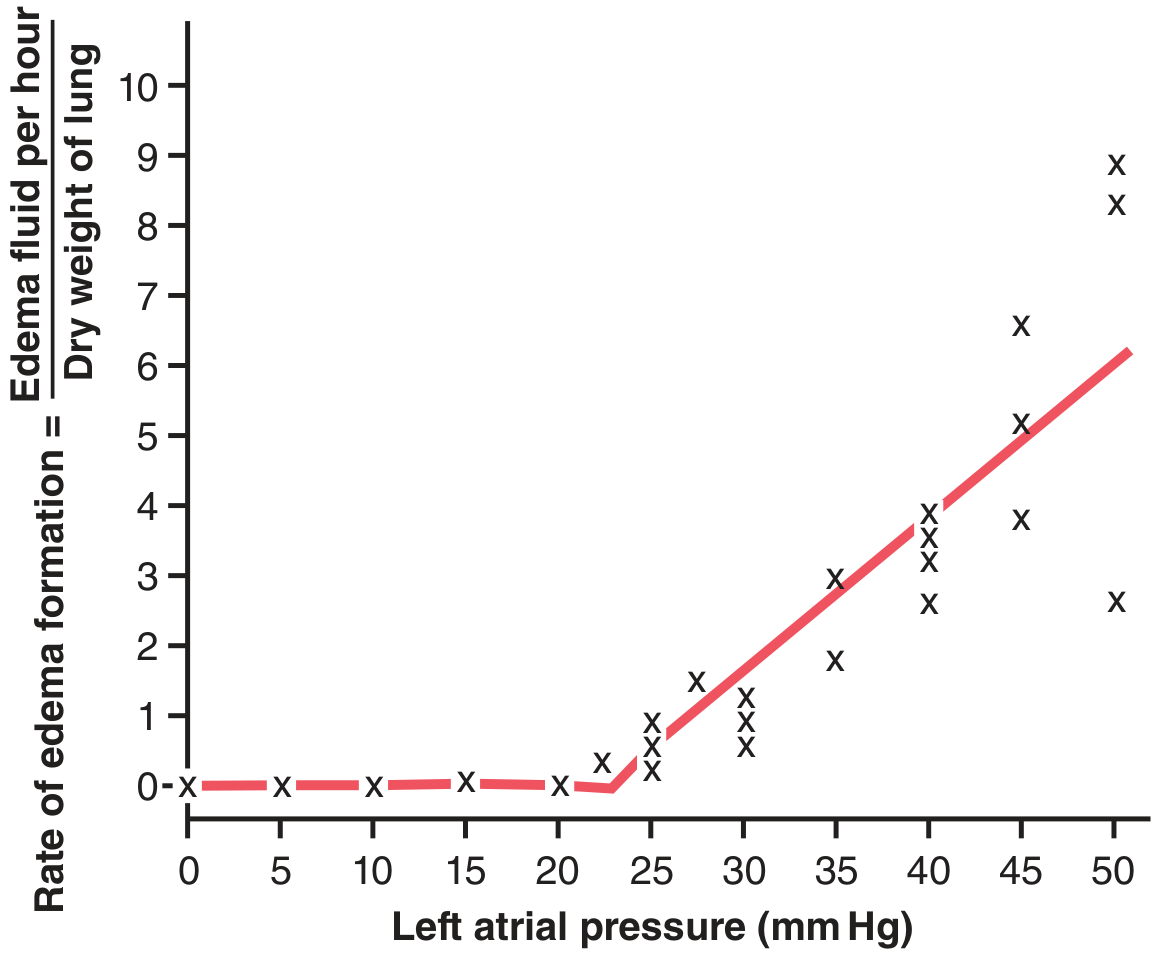
Pulmonary edema is excessive fluid accumulation in the pulmonary interstitium and alveoli. It results whenever factors that promote fluid filtration out of the pulmonary capillaries exceed lymphatic drainage capacity. The driving equation follows the Starling principle: when pulmonary capillary wedge pressure (PCWP) rises above the plasma colloid osmotic pressure (~28 mmHg), fluid floods the interstitium and then the alveoli. Normally, capillary pressure must rise above ~25 mmHg before significant edema occurs - this is the "safety factor." Death from acute pulmonary edema can occur within 20-30 minutes if capillary pressure rises 25-30 mmHg above this threshold.
- Guyton and Hall Textbook of Medical Physiology, p. 509
In chronic conditions (e.g., mitral stenosis), lymphatics expand up to 10-fold, allowing PCWP of 40-45 mmHg to be tolerated without lethal edema.
Classification
| Type | Mechanism | Common Causes |
|---|---|---|
| Hemodynamic (Cardiogenic) | Increased hydrostatic pressure | Left heart failure, volume overload, mitral stenosis, pulmonary vein obstruction |
| Hemodynamic (Low Oncotic) | Decreased plasma oncotic pressure | Hypoalbuminemia, nephrotic syndrome, liver disease |
| Lymphatic Obstruction | Impaired drainage | Lymphangitic carcinoma (rare) |
| Alveolar Wall Injury (Non-cardiogenic) | Increased capillary permeability | Sepsis (ARDS), pneumonia, aspiration, inhaled toxins, drugs (bleomycin, heroin, cocaine), pancreatitis, burns, blood transfusion (TRALI) |
| Undetermined | Mixed/unknown | High altitude (HAPE), neurogenic |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Table 15.1
Pathology
Cardiogenic (Hemodynamic) edema:
- Edema is initially dependent (basal lung zones)
- Histology: engorged alveolar capillaries, finely granular pale pink transudate in alveoli, microhemorrhages, hemosiderin-laden macrophages ("heart failure cells")
- Chronic congestion (e.g., mitral stenosis): abundant hemosiderin macrophages, fibrosis, thickened alveolar walls - "brown induration" - impairs gas exchange and predisposes to infection
Non-cardiogenic edema (alveolar wall injury):
- Inflammatory exudate leaks into interstitium and alveoli
- Protein-rich fluid (distinguishes from transudate)
- Severe form progresses to ARDS with hyaline membrane formation
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 631
Clinical Features
Symptoms:
- Dyspnea at rest, orthopnea, paroxysmal nocturnal dyspnea (PND)
- Pink frothy sputum (alveolar flooding)
- Anxiety, diaphoresis, sense of suffocation
Signs:
- Tachypnea, tachycardia
- Bilateral basal (inspiratory) crackles
- S3 gallop, elevated JVP, peripheral edema (in heart failure)
- Hypoxia (widened A-a gradient)
- In "flash" pulmonary edema: sudden onset, often hypertensive
Diagnosis
Chest X-ray findings (progressive severity):
- Vascular redistribution (upper lobe vessel prominence)
- Kerley B lines (interstitial phase)
- Bat-wing/"butterfly" perihilar alveolar opacities
- Pleural effusions, cardiomegaly (in cardiogenic)
BNP/NT-proBNP:
- BNP >500 pg/mL or NT-proBNP >900 pg/mL: moderately useful for establishing heart failure diagnosis
- Values 100-500 pg/mL are indeterminate
- Note: BNP can be falsely low in "flash" pulmonary edema settings
- Tintinalli's Emergency Medicine, p. 3552
Point-of-Care Ultrasound (POCUS):
- B-lines (comet-tail artifacts) on lung ultrasound indicate interstitial edema and are more sensitive than clinical exam, especially in CKD/ESRD patients where exam findings correlate poorly with edema severity
- Recent systematic review (2025, PMID 40845678) confirms utility of POCUS for diagnosing pulmonary edema
ABG: Hypoxemia, respiratory alkalosis early; respiratory acidosis late (fatigue).
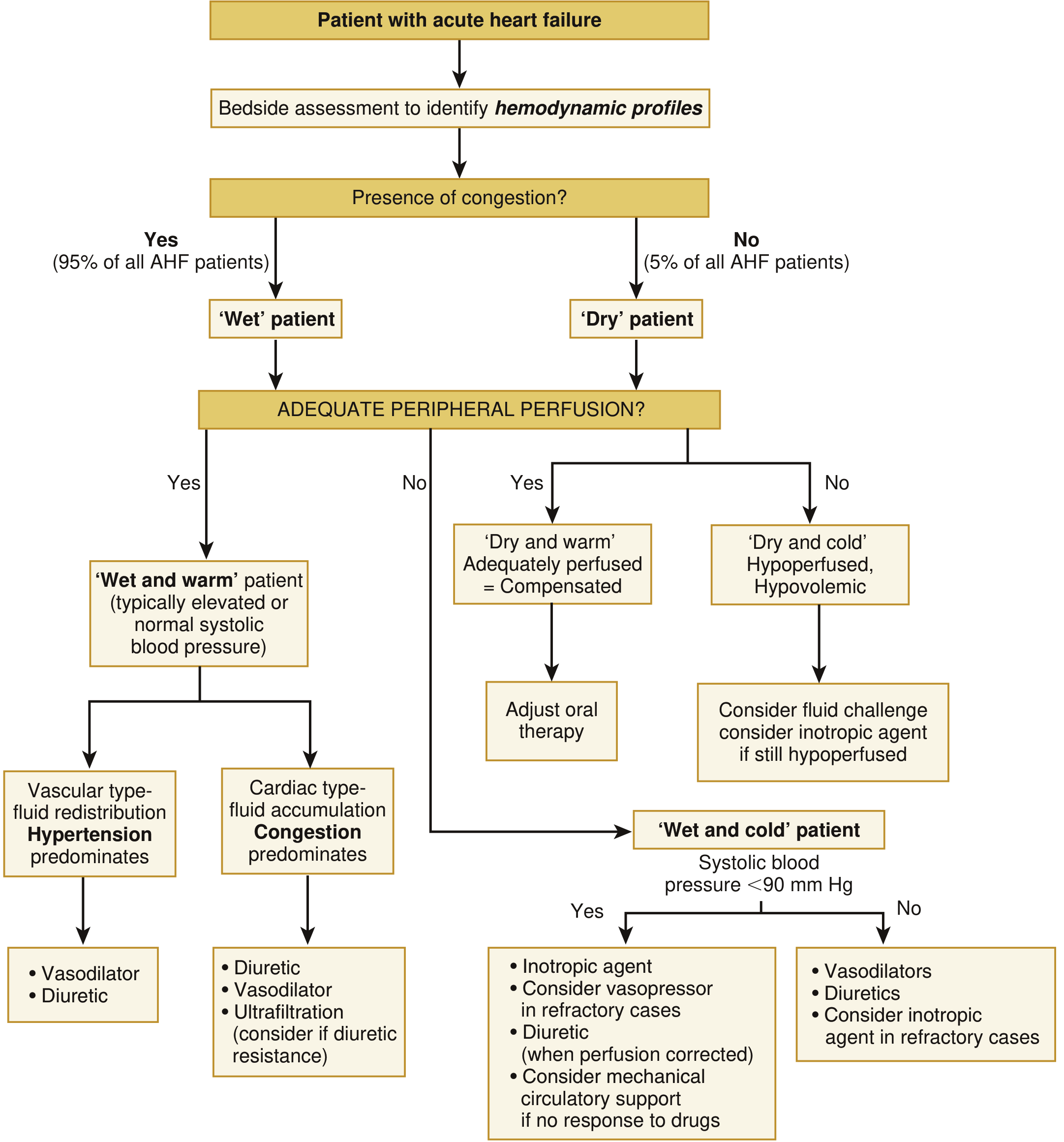
Management
The ESC/Braunwald hemodynamic profiling approach classifies patients as "wet/dry" and "warm/cold" to guide therapy:
1. Positioning and Oxygen
- Sit patient upright with legs dependent (reduces venous return)
- Supplemental O2 to target SpO2 ≥94%
2. Non-Invasive Ventilation (NIV)
- CPAP or BiPAP is a first-line intervention; reduces need for intubation, improves oxygenation, reduces preload, and decreases LV afterload by increasing intrathoracic pressure
- Meta-analyses show NIV (primarily CPAP) decreases intubation rate and improves mortality in cardiogenic pulmonary edema
- CPAP vs. BiPAP: no significant difference in clinical outcomes when directly compared
- Contraindications: inability to protect airway, life-threatening hypoxia requiring immediate intubation, altered sensorium, patient non-cooperation
- Fishman's Pulmonary Diseases and Disorders, p. 2630
3. Loop Diuretics
- Furosemide (0.5 mg/kg IV; up to 1 mg/kg if renal insufficiency/chronic diuretic use) is first-line - it acts as a venodilator rapidly before diuresis begins
- Over 75% of AHF emergency patients receive IV diuretics; mean door-to-diuretic time ~2.2 hours in the ADHERE registry
- Continuous infusion or combination diuretics for diuretic resistance
- If hypotensive or in cardiogenic shock: diuretics are of limited benefit; ultrafiltration preferred
- Harrison's Principles of Internal Medicine 22E, p. 2374; Braunwald's Heart Disease, p. 111
4. Vasodilators (Nitrates)
- Sublingual nitroglycerin 0.4 mg q5 min × 3 is first-line for acute cardiogenic pulmonary edema
- If persistent without hypotension: IV nitroglycerin starting at 5-10 μg/min (up to 300+ μg/min)
- Early IV nitrate therapy in severe cardiogenic pulmonary edema reduces need for mechanical ventilation and frequency of MI
- IV nitroprusside (0.1-5 μg/kg/min): potent arteriovenous dilator for pulmonary edema with hypertension; requires arterial line monitoring; avoid in reduced coronary perfusion states
- ACE inhibitors: reduce preload and afterload; beneficial in hypertensive patients and post-MI heart failure
- A 2025 systematic review (PMID 40506079) supports high-dose IV nitroglycerin in sympathetic crashing acute pulmonary edema
- Harrison's Principles of Internal Medicine 22E, p. 2374
5. Morphine - Controversial
- Historically used (2-4 mg IV) for vasodilation and dyspnea relief
- Retrospective registry data shows association with increased mortality (increased intubation, ICU admission, prolonged stay)
- European Society of Cardiology recommends against routine use; AHA/ACC discusses morphine only in palliative context
- Use with caution if at all; only in severe refractory dyspnea
- Murray & Nadel's Textbook of Respiratory Medicine, p. 3125; Braunwald's Heart Disease, p. 111
6. Inotropic/Inodilator Drugs (Cardiogenic Shock)
- Indicated when pulmonary edema accompanies hypotension/cardiogenic shock
- Dobutamine, dopamine (sympathomimetic amines): temporary inotropic support
- Milrinone (phosphodiesterase-3 inhibitor, 50 μg/kg load → 0.25-0.75 μg/kg/min): inotropic + vasodilator; useful in severe LV dysfunction
- Not recommended for patients with depressed EF and pulmonary edema but without hypotension or impaired perfusion (may be harmful)
- Harrison's Principles of Internal Medicine 22E, p. 2374; Murray & Nadel's, p. 3125
7. Renal Replacement Therapy
- Indicated for refractory volume overload, metabolic acidosis (pH <7.15-7.25), persistent hyperkalemia, or severe hypoxemia unresponsive to pharmacotherapy
- In CKD/ESRD: hemodialysis is the most rapidly effective treatment (peritoneal dialysis too slow)
- Continuous renal replacement therapy (CVVH) preferred when patient is hypotensive or requiring vasopressors
8. Intubation and Mechanical Ventilation
- Required in ~4-5% of all AHF patients
- Indications: failure of NIV, inability to protect airway, life-threatening hypoxia
Special Clinical Situations
High-Altitude Pulmonary Edema (HAPE)
- Non-cardiogenic, caused by hypoxic pulmonary vasoconstriction
- Treatment: descent + oxygen (definitive); nifedipine (calcium channel blocker) is useful pharmacologically; phosphodiesterase-5 inhibitors (sildenafil/tadalafil) are alternatives
- Furosemide and nitroglycerin are not first-line
Neurogenic Pulmonary Edema
- Follows CNS trauma/SAH; catecholamine surge causes massive increase in pulmonary capillary pressure and permeability
- Management: treat underlying CNS pathology; supportive care
CKD/ESRD-Associated Pulmonary Edema
- Etiology is often multifactorial: increased hydrostatic pressure (fluid overload/CHF) + reduced oncotic pressure (hypoalbuminemia) + increased permeability (uremia)
- Dialysis is the most effective treatment; standard diuretics often ineffective
- Physical exam findings (crackles, edema) correlate poorly with actual degree of interstitial edema in this population
Physiology Summary (Key Numbers)
| Parameter | Value |
|---|---|
| Normal PCWP | ~7 mmHg |
| Plasma colloid osmotic pressure | ~28 mmHg |
| Threshold for pulmonary edema | ~25-28 mmHg |
| Acute safety factor | ~21 mmHg |
| PCWP in chronic mitral stenosis (tolerated) | 40-45 mmHg |
| BNP threshold (supports HF diagnosis) | >500 pg/mL |
| NT-proBNP threshold | >900 pg/mL |
Key Sources:
- Guyton and Hall Textbook of Medical Physiology (physiology/safety factors)
- Robbins, Cotran & Kumar Pathologic Basis of Disease (classification/pathology)
- Harrison's Principles of Internal Medicine 22E (management/pharmacology)
- Braunwald's Heart Disease (AHF hemodynamic profiles/algorithm)
- Murray & Nadel's Textbook of Respiratory Medicine (pharmacologic therapy)
- Fishman's Pulmonary Diseases and Disorders (NIV evidence)
- Tintinalli's Emergency Medicine (BNP thresholds/CKD)
Recent Evidence Update:
This is a shared conversation. Sign in to Orris to start your own chat.