Ecg more details tell me
Reading File
Asking for Preferences
Finding Sources
Searching the Web
ECG interpretation systematic approach steps 2024
Reading File
Finding Sources
Searching Images
ECG interpretation 12-lead waveforms diagram
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive guide to ECG interpretation, drawn from Harrison's Principles of Internal Medicine (22nd ed., 2025) and Kaplan & Sadock's Comprehensive Textbook of Psychiatry.
ECG Interpretation — Systematic Approach
The Systematic Framework
Harrison's stresses that errors of omission are the most common mistakes in ECG reading. Always analyze these 14 parameters in every ECG:
- Standardization / calibration & technical quality
- Rhythm
- Heart rate
- PR interval / AV conduction
- QRS interval
- QT / QTc intervals
- Mean QRS electrical axis
- P waves
- QRS voltages
- Precordial R-wave progression
- Abnormal Q waves
- ST segments
- T waves
- U waves
Step 1 — Technical Check
Before interpreting anything:
- Confirm standard calibration: 10 mm = 1 mV; paper speed 25 mm/s
- Check for lead misplacement or artifact (baseline wander, noise)
- Artifact in certain leads can obscure P waves and T-wave morphology — compare good vs. noisy leads
Step 2 — Heart Rate
On standard ECG paper:
- Small box = 0.04 seconds
- Large box = 0.2 seconds
- 300 large boxes = 1 minute
Two calculation methods:
| Method | Use | Formula |
|---|---|---|
| Rate by squares | Regular rhythms | 300 ÷ (number of large boxes between R waves) |
| QRS count method | Irregular rhythms | Count QRS complexes on full strip × 6 |
- Bradycardia: HR < 60 bpm
- Tachycardia: HR > 100 bpm
Step 3 — Rhythm
Ask: Is it regular or irregular? Are there P waves before every QRS?
- Sinus rhythm: P wave positive in II, negative in aVR; P before every QRS; PR consistent
- Ectopic/retrograde P waves: Negative in II, positive in aVR (from lower atrial or AV junctional pacemaker)
- Irregular rhythms: Consider atrial fibrillation, flutter, ectopics, or heart blocks
Step 4 — The 12 Leads (Anatomy of the ECG)
The 12 leads are divided into two groups:
| Group | Leads | Plane |
|---|---|---|
| Limb leads | I, II, III, aVR, aVL, aVF | Frontal |
| Precordial leads | V1–V6 | Horizontal |
Each lead is like a camera angle — a positive deflection means depolarization is moving toward that lead; negative means moving away.
Step 5 — Electrical Axis
The axis represents the net vector of ventricular depolarization. Assessed using Lead I (0°) and aVF (+90°):
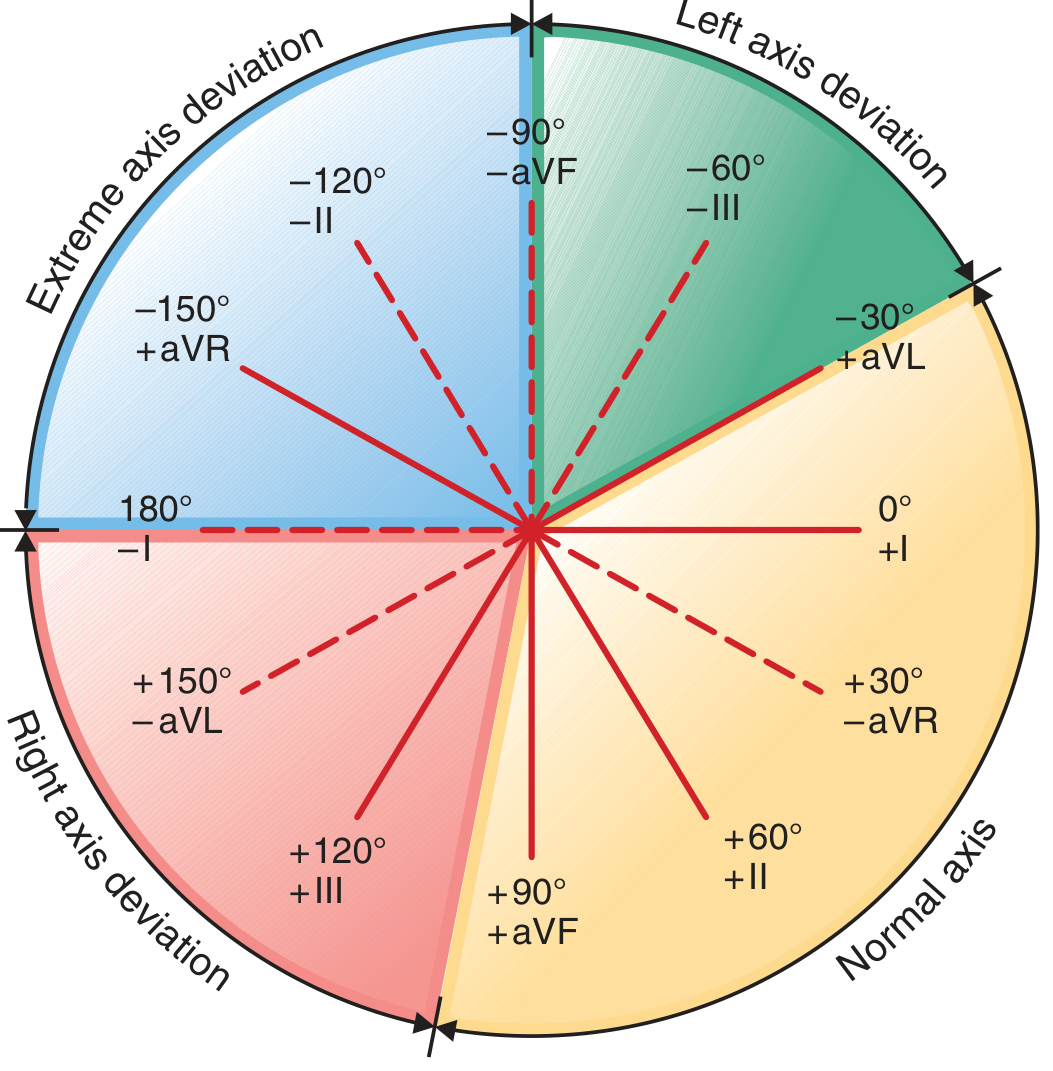
| Axis | Range | Common Causes |
|---|---|---|
| Normal | −30° to +90° | — |
| Left axis deviation (LAD) | More negative than −30° | LVH, left anterior fascicular block, inferior MI |
| Right axis deviation (RAD) | More positive than +110° | RVH, left posterior fascicular block, COPD |
| Extreme deviation | −90° to ±180° | Ventricular rhythms, lead misplacement |
Step 6 — Intervals
PR Interval
- Represents atrio-ventricular conduction time
- Normal: 0.12–0.20 s (3–5 small boxes)
- Short PR: Pre-excitation (WPW) or AV junctional rhythm
- Prolonged PR: 1st degree AV block, drugs, ischemia
- Progressive prolongation then dropped QRS: Mobitz Type 1 (Wenckebach)
- Fixed PR with intermittent dropped QRS: Mobitz Type 2
- No relationship between P and QRS: Complete (3rd degree) AV block
QRS Duration
- Normal: < 0.12 s (< 3 small boxes)
- Widened QRS (≥ 0.12 s): Bundle branch block, ventricular rhythm, hyperkalemia, drugs (class IA antiarrhythmics, TCAs)
QT / QTc Interval
- Represents ventricular depolarization + repolarization
- Must be corrected for HR: Bazett formula = QT ÷ √RR (default on most machines)
- More accurate at normal HR; tends to overcorrect at fast rates
- AHA recommends Framingham or Hodges formula for extremes of HR
| Sex | Normal QTc |
|---|---|
| Men | < 430 ms |
| Women | < 450 ms |
- Prolonged QTc: Risk of Torsades de Pointes (TdP); risk increases 1.052× for every 10 ms above 400 ms
- Causes: Hypokalemia, hypocalcemia, drugs (quinidine, sotalol, amiodarone, TCAs, phenothiazines, some antipsychotics), hypothermia, subarachnoid hemorrhage
Step 7 — P Waves
- Normal: Positive in II, negative in aVR
- Peaked P (>2.5 mm) in II: Right atrial enlargement ("P pulmonale")
- Broad, notched P: Left atrial enlargement ("P mitrale")
- In V1: biphasic — initial positive component = right atrium; terminal negative component (>1 mm²) = left atrial enlargement
Step 8 — QRS Morphology
Normal R-wave progression (precordial leads)
- Small r in V1 → progressively taller through V3–V5
- Poor R-wave progression = anterior MI or cardiomyopathy
Bundle Branch Blocks (RBBB vs LBBB)
- RBBB: rSR' ("rabbit ears") in V1; wide S in V6; secondary T-wave inversion in right precordial leads
- LBBB: broad notched R in V5/V6; QS in V1; discordant T waves
- T wave typically opposite in polarity to the last QRS deflection in bundle branch blocks
Ventricular Hypertrophy
- LVH: Tall R in V5/V6 + deep S in V1 (Sokolow-Lyon index: SV1 + RV5 > 35 mm)
- RVH: Right axis deviation + dominant R in V1
Step 9 — ST Segments
The ST segment sits between the end of S wave and start of T wave (the isoelectric J point).
| Finding | Meaning |
|---|---|
| ST elevation (transmural ischemia) | Acute epicardial injury — current of injury toward leads over the affected zone |
| ST depression (subendocardial ischemia) | ST vector shifts toward subendocardium — reciprocal changes |
| Diffuse ST elevation (saddle-shaped) | Pericarditis |
| "Scooped" ST | Digoxin effect |
| Convex ST elevation with bradycardia (Osborn wave) | Hypothermia |
In acute transmural ischemia: earliest sign is tall hyperacute T waves → ST elevation → Q wave formation → T-wave inversion.
Step 10 — T Waves & U Waves
- T-wave inversion: Ischemia, ventricular strain, bundle branch block, CNS events (intracranial bleeds → deep wide "CVA T-waves"), drug effects
- Tall, peaked ("tented") T waves: Hyperkalemia (earliest sign)
- Flattened T: Hypokalemia, nonspecific changes
- U wave (small deflection after T): Prominent in hypokalemia; normally most visible in V2–V3
Example: 12-Lead ECG
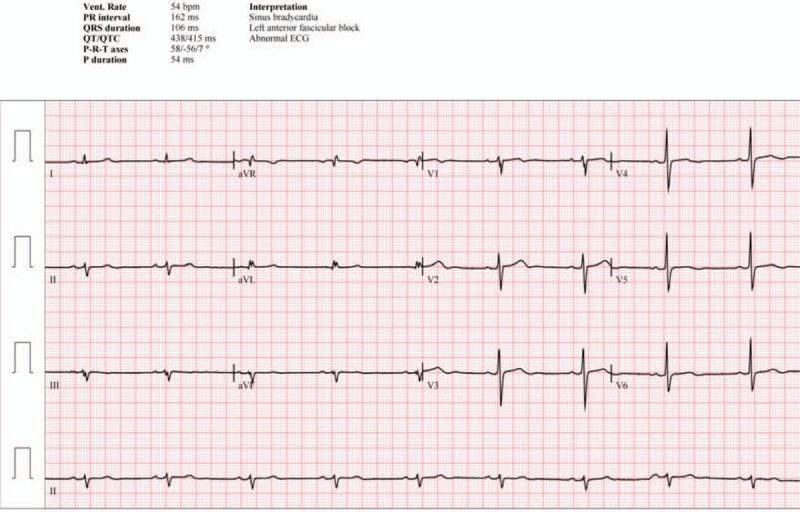
This tracing shows: ventricular rate 54 bpm (sinus bradycardia), PR 162 ms, QRS 106 ms, QTc 415 ms, left axis deviation (axis −56°) consistent with left anterior fascicular block — small q + tall R in I/aVL, small r + deep S in II/III/aVF.
Conditions That Make ECG Interpretation Difficult
- Bundle branch blocks (mask ischemia patterns)
- Pacemaker rhythms
- Pre-excitation (WPW)
- Ventricular hypertrophy
- Electrolyte abnormalities
- Hypothermia
- Early repolarization variants
Key Takeaway
A reliable systematic approach (rate → rhythm → axis → intervals → morphology → ST-T) prevents errors of omission. Always compare with previous ECGs — change over time is often more informative than any single tracing.
— Harrison's Principles of Internal Medicine, 22nd ed. (2025), Chapter 247; Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Ecg more details and image in tamil
Finding Sources
Searching Images
normal ECG waveform P QRS T wave labeled diagram
Searching Images
12-lead ECG heart electrical conduction system diagram
Loading Image
Loading Image
Loading Image
மேலே உள்ளது ECG பற்றிய முழுமையான தமிழ் வழிகாட்டி — 3 மருத்துவ படங்களுடன்:
- முதல் படம் — இதயம் + ECG இணைப்பு, அனைத்து intervals காட்டுகிறது
- இரண்டாம் படம் — P, QRS, ST, T, U அலைகளின் திட்டப்படம் (Harrison's)
- மூன்றாம் படம் — Normal, RBBB, LBBB QRS வடிவங்கள் ஒப்பீடு
உள்ளடக்கிய தலைப்புகள்:
- ECG காகித அளவீடு
- ஒவ்வொரு அலையின் (P, QRS, ST, T, U) விளக்கம்
- PR, QRS, QT இடைவெளிகள் — சாதாரண மதிப்புகள்
- 12-லீட் ECG — ஒவ்வொரு லீட்டின் இடம் மற்றும் நோக்கம்
- மின் அச்சு (Electrical Axis)
- இதய துடிப்பு கணக்கீடு
- Bundle Branch Block
- MI, AV Block, AF, Hyperkalemia ECG மாற்றங்கள்
- 14-படி முறையான ECG படிக்கும் வழிமுறை
This is a shared conversation. Sign in to Orris to start your own chat.