Brain injury
Reading File
Asking for Preferences
Brain injury
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Searching PubMed
"traumatic brain injury"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Searching PubMed
"traumatic brain injury"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full in-depth answer.
Traumatic Brain Injury (TBI): Mechanisms & Management
Definition and Epidemiology
Traumatic brain injury (TBI) occurs when a direct or indirect force to the brain disrupts normal brain function. It is one of the most common forms of neurological damage - in the United States alone, TBI results in more than 53,000 deaths per year, with young males disproportionately affected. Over 5.3 million Americans and 7.7 million Europeans live with persistent impairments from TBI. - Bradley and Daroff's Neurology in Clinical Practice
Severity Classification
TBI is classified by the Glasgow Coma Scale (GCS) at presentation:
| Severity | GCS Score | Loss of Consciousness | Amnesia |
|---|---|---|---|
| Mild (Concussion) | 13-15 | < 30 minutes | < 30 minutes |
| Moderate | 9-12 | > 30 min, < 24 h | > 30 min |
| Severe | ≤ 8 (coma) | > 24 hours | Prolonged |
The GCS assesses three domains: eye opening, best verbal response, and best motor response. Severe TBI (GCS ≤ 8) is defined as coma or progressive decline of consciousness and requires ICU management. - Goldman-Cecil Medicine
Pathophysiology: Primary vs. Secondary Brain Injury
Primary Brain Injury
This is the immediate, irreversible mechanical damage at the moment of impact. It cannot be reversed - outcomes depend entirely on how well secondary injury is prevented. Three main subtypes occur:
1. Skull Fractures
- Linear, comminuted, open/closed, or depressed
- Basilar skull fractures prompt assessment for cranial nerve injuries, vascular injuries, and CSF fistulas
- Classic signs: Battle's sign (postauricular ecchymosis), raccoon eyes (periorbital ecchymosis), hemotympanum, CSF rhinorrhea/otorrhea
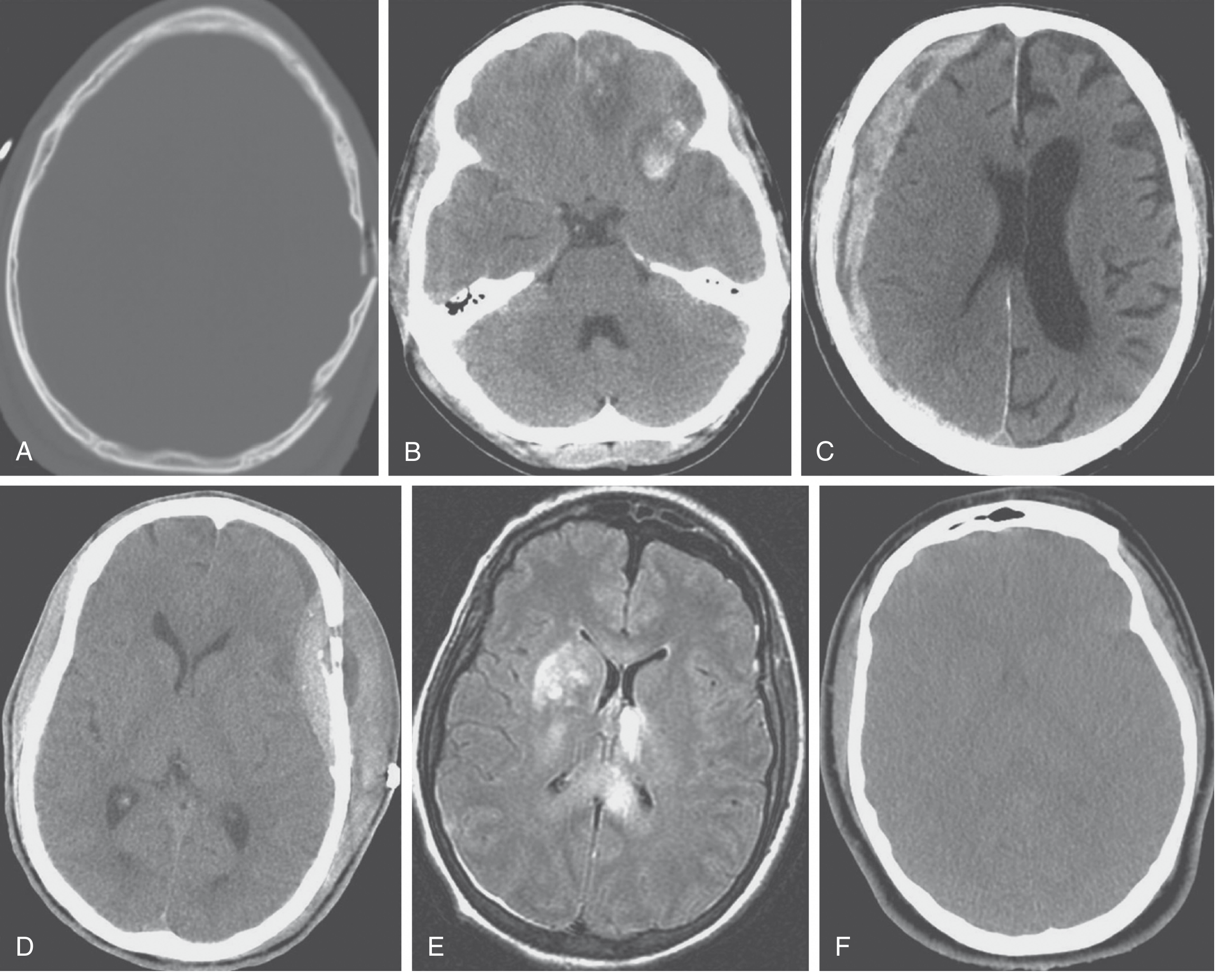
2. Intracranial Hemorrhage
All operate via the Monro-Kellie doctrine - the skull is a fixed space, and any new blood volume displaces brain tissue and CSF, ultimately causing herniation.
| Type | Source | CT Appearance | Key Features |
|---|---|---|---|
| Epidural (EDH) | Middle meningeal artery tear | Biconvex/lenticular hyperdensity | Classic "lucid interval"; rapidly fatal if missed |
| Subdural (SDH) | Tearing of bridging veins | Crescent-shaped hyperdensity | Common in elderly/anticoagulated; "talk and die" risk |
| Subarachnoid (SAH) | Small pial vessels | Hyperdensity in sulci/cisterns | Risk of cerebral vasospasm |
| Intraparenchymal | Coup-contrecoup mechanism | Focal hyperdensity in parenchyma | Contusions can "blossom" hours later |
| Intraventricular | Extension from parenchymal bleed | Hyperdensity in ventricles | Rarely in isolation |
3. Diffuse Axonal Injury (DAI)
- Caused by rotational acceleration-deceleration forces acting on white matter tracts
- Results in primary axotomy (immediate) followed by secondary axotomy over 6-12 hours (apoptosis/degeneration)
- Often not visible on initial CT - MRI shows multifocal hyperintense lesions at gray-white matter interfaces, in the corpus callosum, and brainstem
- Graded by severity: mild (axonal stretching, concussion) to severe (coma with brainstem involvement)
- Diagnosis suspected when patient remains unconscious despite no CT hemorrhage, or fails to improve after surgical decompression
Sabiston Textbook of Surgery
Secondary Brain Injury
After the primary insult, a cascade of cellular and biochemical events continues for hours to weeks causing further neuronal death. This is the main target of clinical management. Mechanisms include:
- Excitotoxicity - excessive glutamate release causes calcium influx and Na+/K+-ATPase failure
- Calcium dysregulation - activates destructive intracellular enzymes (caspases, lipases, proteases)
- Free radical generation - overwhelms endogenous antioxidant defenses
- Blood-brain barrier (BBB) disruption - leads to vasogenic edema
- Cerebral edema and intracranial hypertension (ICP elevation)
- Ischemia - from impaired cerebral autoregulation + systemic hypotension
Key systemic secondary insults that dramatically worsen outcomes:
| Insult | Threshold | Effect |
|---|---|---|
| Hypotension | SBP < 90 mmHg | Nearly doubles TBI mortality |
| Hypoxia | PaO₂ < 60 mmHg | Doubles mortality in severe TBI |
| Hyperpyrexia | Fever | Increases metabolic demand |
| Hypocarbia | PaCO₂ < 35 mmHg | Causes vasoconstriction, ischemia |
| Hypercarbia | PaCO₂ > 45 mmHg | Raises ICP via vasodilation |
Rosen's Emergency Medicine; Sabiston Textbook of Surgery
Clinical Presentation
Mild TBI (Concussion)
- Brief LOC (< 30 min) or transient amnesia/confusion
- Headache, dizziness, difficulty with memory/concentration, balance problems, fatigue
- Physical exam: abnormal smooth pursuit/saccadic eye movements, convergence insufficiency, unsteady gait
- No signs of raised ICP or herniation
Moderate-Severe TBI
- GCS 9-12 (moderate): confusion to agitation to somnolence persisting ≥ 24 hours
- GCS ≤ 8 (severe): coma, focal deficits, decorticate/decerebrate posturing
Signs of raised ICP:
- Cushing's reflex: hypertension + bradycardia + irregular respirations (late, ominous sign)
- Vomiting, papilledema
Signs of herniation:
- Uncal herniation: ipsilateral fixed dilated pupil + contralateral motor paralysis (CN III compression)
- Tonsillar herniation: pinpoint or midsized unreactive pupils + flaccid paralysis
Goldman-Cecil Medicine; Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Management
Primary Survey (ABCDE - minutes)
The goal is identifying and treating immediately life-threatening conditions first.
Airway:
- Assume cervical spine instability in all trauma patients until ruled out - in-line manual stabilization, hard neck collar
- "Chin-lift" and "head-tilt" maneuvers are contraindicated (risk of spinal injury)
- Rapid sequence intubation (RSI) recommended - all trauma patients are at aspiration risk
- Nasotracheal intubation preferred in spontaneously breathing patients; orotracheal for apneic patients
- Avoid blind nasal intubation if basilar skull fracture suspected
Breathing:
- Tension pneumothorax: absent breath sounds + hyperresonance + hemodynamic shock → needle decompression (2nd ICS, midclavicular) + chest tube
Circulation:
- Hemorrhagic shock is most common cause of hypotension in trauma
- Initial crystalloid + compression of bleeding sites; proactive blood product replacement
- Avoid SBP < 90 mmHg - consider targeting higher MAP in TBI to maintain cerebral perfusion
Neurological exam:
- GCS assessment
- Pupillary responses, corneal reflex, cough/gag, motor posturing
- Note: do NOT perform doll's eyes maneuver until cervical spine cleared
Risk Stratification and CT Indications
| Risk Group | Features | Management |
|---|---|---|
| Low risk | Normal neuro exam, no concussion, no intoxication, reliable observer available | Discharge with return precautions; no mandatory CT |
| Moderate risk | Concussion, GCS 9-14, basilar fracture signs, seizures, age < 2 or > 65, alcohol/drug intoxication | CT head required; consider admission |
| Severe | GCS ≤ 8, focal neuro deficits, penetrating injury, palpable depressed fracture | ICU admission; urgent neurosurgical evaluation |
ICP Management (Severe TBI)
Target: ICP < 20-22 mmHg; Cerebral Perfusion Pressure (CPP) = MAP - ICP, target CPP 60-70 mmHg
Stepwise approach:
- Head of bed elevation 30°, neutral head positioning
- Adequate sedation and analgesia (reduces metabolic demand)
- Osmotherapy: Mannitol (0.25-1 g/kg IV) OR hypertonic saline (3% NaCl) - both reduce cerebral edema; hypertonic saline is preferred when hemodynamically unstable
- Controlled ventilation: target PaCO₂ 35-45 mmHg (avoid hyperventilation except as brief bridge)
- Neuromuscular blockade if refractory
- Surgical decompression: hemicraniectomy or bifrontal craniotomy for refractory ICP; epidural hematomas require emergent evacuation
Operative Indications
- EDH: surgical evacuation is urgently indicated (classic lucid interval followed by rapid decline)
- Acute SDH with significant mass effect or midline shift
- Depressed skull fracture > one skull thickness deep, or open/contaminated fracture
- Refractory ICP: decompressive craniectomy
Secondary Survey and Ongoing Care
- CT head, CT cervical spine, full trauma imaging
- Seizure prophylaxis: levetiracetam or phenytoin in severe TBI (short-term, 7 days)
- Glucose control: avoid hypoglycemia AND hyperglycemia
- Temperature management: treat fever aggressively; therapeutic hypothermia remains investigational
- Nutrition: early enteral nutrition within 24-48 hours
Neurocognitive Sequelae
After moderate-severe TBI, patients commonly experience impairments across multiple domains:
| Cognitive Domain | Manifestations |
|---|---|
| Attention | Difficulty with sustained attention, poor concentration |
| Memory | Problems acquiring new verbal/nonverbal information |
| Processing speed | Slowed sensorimotor response |
| Executive function | Poor judgment, difficulty planning, impulsivity |
| Language | Word comprehension problems, impaired reading/writing |
| Awareness | Difficulty recognizing own deficits ("anosognosia") |
Frontal lobe damage is especially common due to skull morphology - this combination of executive dysfunction, behavioral dysregulation, and social cognition impairment is called frontal lobe syndrome.
Bradley and Daroff's Neurology in Clinical Practice
Prognosis
- Mild TBI: most patients recover fully within weeks to months; a minority develop persistent post-concussion syndrome
- Moderate-severe TBI: significant morbidity; recovery can continue for 1-2 years with intensive rehabilitation
- Worst prognostic factors: GCS motor score of 1 (no response), bilateral fixed pupils, older age, sustained hypotension/hypoxia, large volume EDH/SDH with midline shift, brainstem injury on MRI
Key Sources:
- Sabiston Textbook of Surgery, Chapter 41 - TBI Pathophysiology and Management
- Goldman-Cecil Medicine - Traumatic Brain Injury
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma - TBI Management Protocols
- Rosen's Emergency Medicine - Primary and Secondary Brain Injuries
- Bradley and Daroff's Neurology in Clinical Practice - Neurocognitive Sequelae of TBI
This is a shared conversation. Sign in to Orris to start your own chat.