Bartholin gland
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Bartholin Gland
Anatomy
The Bartholin glands (greater vestibular glands) are a pair of pea-sized mucus-secreting glands located posterolaterally in the vulva, between the hymen and the labia minora. Their ducts drain into the posterior vestibule at the 4 o'clock and 8 o'clock (or 5 and 7 o'clock) positions.
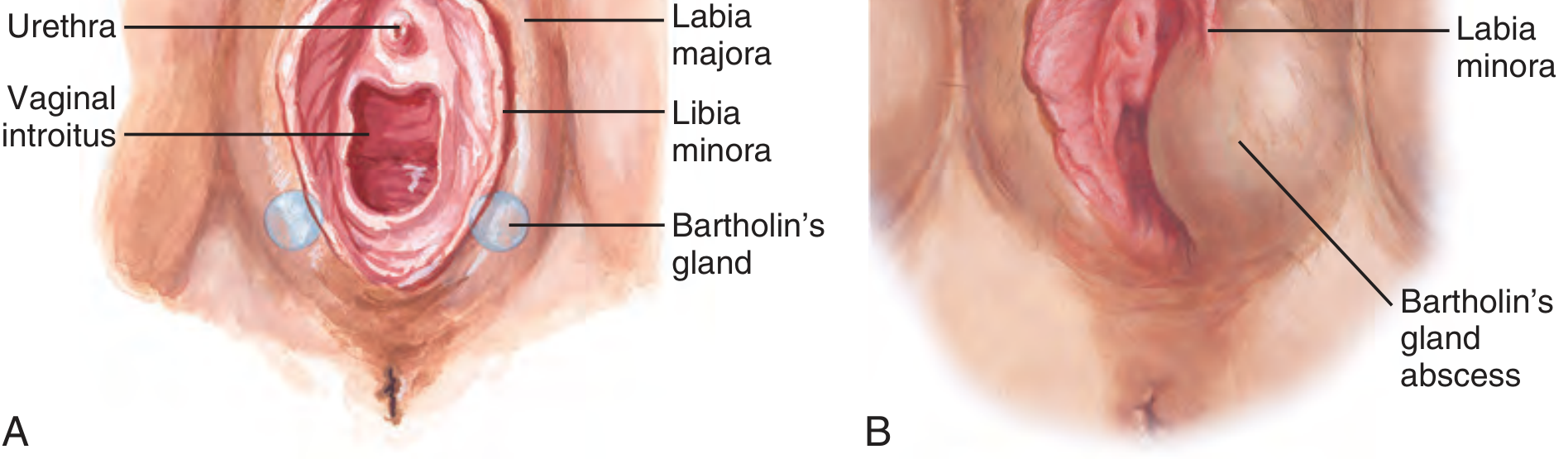
Figure: Normal anatomy (A) showing bilateral Bartholin glands at the posterior vestibule; (B) Bartholin gland abscess appearance. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
- The glands begin functioning at puberty, providing lubrication/moisture to the vestibule
- They involute with age (postmenopausal women)
- Histologically, the main duct is lined with stratified squamous epithelium, transitioning to transitional epithelium toward the terminal ducts; the gland itself produces mucus
Bartholin Duct Cyst
Pathogenesis: Obstruction of the duct (from trauma, inflammation, or edema) leads to accumulation of secretions and cyst formation. Cysts are typically sterile.
Clinical features:
- Painless or mildly uncomfortable swelling at the posterior vestibule (4 or 8 o'clock)
- Variable size - from small and asymptomatic to several centimeters
- Small, asymptomatic cysts do not require treatment
Bartholin Gland Abscess
Pathogenesis: Retained secretions become infected, or obstruction is followed by superinfection. A pre-existing cyst need not be present - an abscess can develop de novo.
Microbiology:
- Most commonly polymicrobial
- E. coli is the single most common isolate
- Neisseria gonorrhoeae and Chlamydia trachomatis are less common but important to consider
- Culture is obtained but rarely changes initial management
Diagnosis:
- Fluctuant, tender, hyperemic mass at the posterior introitus (4 or 8 o'clock position), developing over several days
- Systemic symptoms (fever, chills) are rarely present
- Ultrasound can confirm a discrete fluid collection when the diagnosis is unclear
- If poorly defined, treat with broad-spectrum antibiotics + analgesics + warm sitz baths with close follow-up before drainage
Treatment
1. Incision and Drainage + Word Catheter (first-line)
The Word catheter is the standard approach for both cysts and abscesses. The goal is not just drainage but creation of a new epithelialized tract to allow ongoing gland drainage and prevent recurrence.
Procedure (Pfenninger & Fowler; Tintinalli; Roberts & Hedges):
- Patient in dorsal lithotomy position
- Local anesthesia: 2% lidocaine with epinephrine at the incision site (or pudendal block); IV opioids/sedation for very uncomfortable patients
- Incision site: mucosal surface of the vestibule, just inside/lateral to the hymenal ring, where fluctuation is maximal - not the external skin
- Stab incision with a #11 scalpel blade - just 3-5 mm (large enough for the Word catheter, no more)
- Allow drainage; culture contents if indicated
- Insert the Word catheter (similar in size to a #10 Foley, with a 1-inch stem and inflatable balloon) into the cavity
- Inflate the balloon with 2-3 mL normal saline (not air)
- Tuck the catheter stem into the vagina for comfort
- Leave in place for 4-6 weeks to allow epithelialization of the new tract
Post-procedure: Analgesics, broad-spectrum antibiotics; targeted STI coverage if N. gonorrhoeae / C. trachomatis suspected.
2. Marsupialization (for recurrent cysts/abscesses)
Preferred for recurrences or when a Word catheter is unavailable/fails.
Procedure:
- Lithotomy position; local anesthetic (2% lidocaine + epinephrine) or pudendal block; spinal/general anesthesia possible
- Longitudinal fusiform incision 1-2 cm wide on the vaginal mucosa inside the hymenal ring
- Excise an ellipse of the cyst wall; remove loculated portions; irrigate with normal saline
- Suture the cyst wall edges to the mucosal edges with 4-0 Vicryl to create a permanent opening
- Note: In patients >40 years, inspect excised tissue for signs of neoplasm - send for histology
3. Complete Excision
Reserved for recurrent gland disease not amenable to the above, or if malignancy is suspected. More morbid, with risk of scarring and hematoma.
Bartholin Gland Carcinoma
A rare but important consideration, especially in older women.
Epidemiology
- Accounts for 2-7% of all vulvar malignancies
- 5x more common in postmenopausal than premenopausal women
- Median age at presentation: ~57 years (younger than non-Bartholin vulvar carcinoma)
Histopathology
Because tumors may arise from the gland or from different parts of the duct, multiple histologic types occur:
- Squamous carcinoma - most common (~88% in the MD Anderson series)
- Adenocarcinoma
- Adenoid cystic carcinoma (~15% of Bartholin carcinomas) - slow-growing, perineural infiltration, marked local recurrence tendency, less lymph node metastasis, better overall prognosis
- Rarely: transitional cell, adenosquamous
Honan's criteria for classifying a tumor as Bartholin gland carcinoma:
- Tumor in the correct anatomic position
- Located deep in the labium majus
- Overlying skin is intact
- Some recognizable normal gland tissue present
(Strict adherence leads to underdiagnosis - large tumors may ulcerate through skin)
Signs and Symptoms
- Most common presentation: vulvar mass or perineal pain
- ~10% have a prior history of Bartholin gland inflammation
- Malignancy is frequently mistaken for benign cysts or abscesses, leading to diagnostic delay
- Key rule: Biopsy is indicated for any solid component within a Bartholin cyst or abscess, and for any cyst/abscess that fails to respond to treatment - Berek & Novak's Gynecology
Treatment
- Historically: radical vulvectomy with bilateral groin and pelvic node dissection
- Current approach (individualized): hemivulvectomy or radical local excision for the primary tumor
- Pelvic node dissection only if groin nodes are positive
- Extensive dissection in the ischiorectal fossa is required; margins are often close
- Postoperative radiation significantly reduces local recurrence (27% → 7%)
- If tumor is fixed or involves adjacent structures (anal sphincter, rectum): preoperative chemoradiation followed by limited surgery
- Radiation/chemoradiation alone: 3- and 5-year survival rates of 72% and 66%, respectively
Prognosis
- Due to deep location, disease tends to present at a more advanced stage than squamous vulvar carcinoma
- Stage for stage, however, prognosis is similar to other vulvar carcinomas
- At the MD Anderson Cancer Center, Bartholin gland carcinoma patients had higher rates of stage III/IV disease (61% vs. 36%) but no significant difference in recurrence-free or overall survival compared with non-Bartholin vulvar carcinoma
Clinical Pearls
| Feature | Detail |
|---|---|
| Location | 4 and 8 o'clock (posterior vestibule) |
| Normal size | Pea-sized; not palpable |
| Cyst vs abscess | Cyst = duct obstruction (sterile); abscess = infected (polymicrobial) |
| Most common organism | E. coli |
| Word catheter duration | 4-6 weeks |
| Malignancy risk | Higher in women >40; biopsy any solid mass or treatment failure |
| Carcinoma frequency | 2-7% of vulvar malignancies |
| Most common carcinoma type | Squamous (~88%) |
| Adenoid cystic variant | Perineural invasion, local recurrence, better prognosis than other types |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
- Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Berek & Novak's Gynecology
- Textbook of Family Medicine, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.