Osmotic diarrhoea
Reading File
Finding Sources
Searching PubMed
"osmotic diarrhea" mechanisms causes
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive material from multiple authoritative gastroenterology textbooks. Here is the complete, structured answer:
Osmotic Diarrhoea
Definition and Mechanism
Osmotic diarrhea occurs when non-absorbable, osmotically active solutes accumulate in the intestinal lumen, creating an osmotic gradient that draws water into the gut. Because neither the small intestine nor the colon can maintain an osmotic gradient against plasma, unabsorbed solutes (and their counter-ions) obligate water retention to maintain intraluminal osmolality equal to body fluids (~290 mOsm/kg). Approximately 3.5 mL of water are retained for every 1 mOsm of retained ions or molecules.
The three root mechanisms are:
- Ingestion of non-absorbable substances (osmotic laxatives, sugar alcohols)
- Maldigestion - failure to break down substrates (disaccharidase deficiency)
- Malabsorption - failure to absorb breakdown products (mucosal disease, pancreatic insufficiency, SIBO)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 226
Causes
1. Poorly Absorbed Ions / Medications
These ions are transported by mechanisms that are easily saturated, so a significant fraction remains unabsorbed:
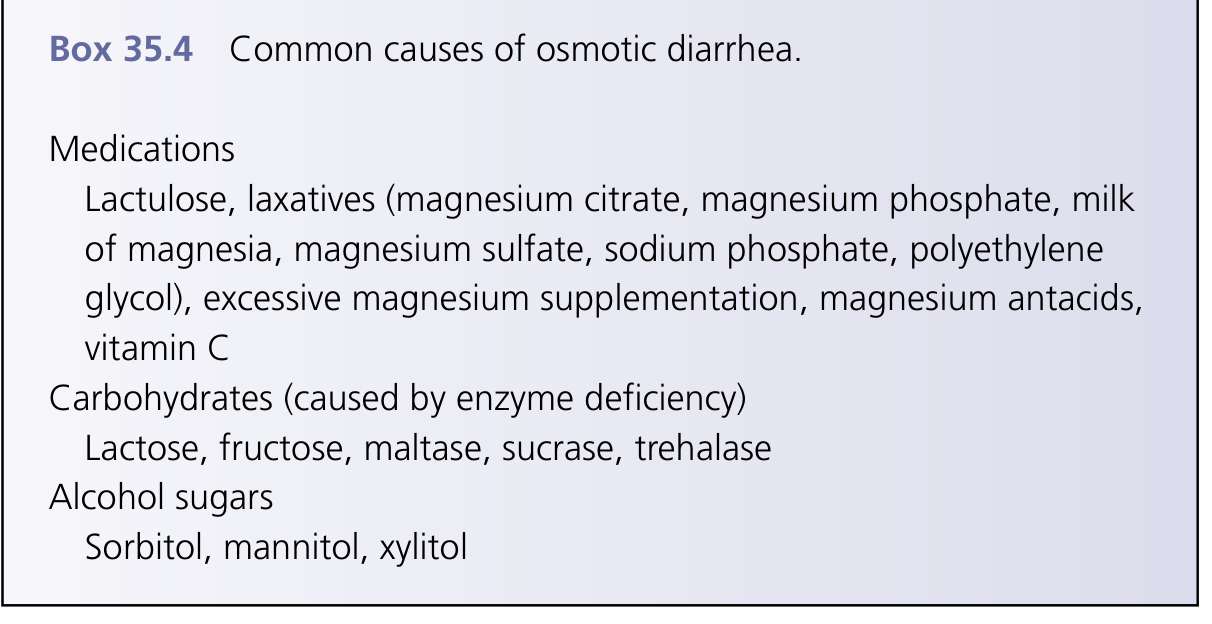
- Magnesium salts - magnesium citrate, magnesium phosphate, milk of magnesia, magnesium sulfate (used as laxatives or antacids - a common accidental cause in patients overusing Mg-antacids for dyspepsia/reflux)
- Phosphate/sulfate salts, polyethylene glycol (PEG), sodium phosphate bowel prep
- Lactulose - a synthetic disaccharide not hydrolyzable by human disaccharidases
- Vitamin C (high doses)
- Other drugs: antibiotics (ampicillin, clindamycin), methyldopa, quinidine, propranolol, hydralazine, ACE inhibitors, procainamide
2. Poorly Absorbed Carbohydrates (Disaccharidase Deficiency)
Monosaccharides can be absorbed intact across the enterocyte apical membrane, but disaccharides require prior enzymatic hydrolysis at the brush border. Deficiency of the relevant enzyme leaves the disaccharide unhydrolyzed and unabsorbed.
| Deficiency | Substrate | Notes |
|---|---|---|
| Lactase (most common) | Lactose (dairy) | Down-regulated in ~70% of adult humans; maintained in northern European and some African gene pools |
| Sucrase | Sucrose (table sugar) | Rare congenital deficiency |
| Trehalase | Trehalose (mushrooms, processed foods) | Rare |
| Maltase | Maltose |
Undigested carbohydrates are fermented by colonic bacteria into short-chain fatty acids, CO2, and H2, explaining the characteristic symptoms of bloating, flatulence, abdominal cramps, and low stool pH (<6).
3. Sugar Alcohols (Polyols)
Sorbitol, mannitol, xylitol, erythritol, lactitol, maltitol, glycerol - widely used as artificial sweeteners. As little as 10 g/day of sorbitol can cause diarrhea. Found in sugar-free gum, low-calorie sodas, diabetic foods, and many pharmaceutical excipients.
4. FODMAPs
A recognized group of Fermentable Oligo-, Di-, Monosaccharides And Polyols (fructose, lactose, fructans, polyols) found in many foods. Incompletely absorbed by many people; implicated in causing symptoms in IBS patients.
5. Generalized Malabsorption States
| Condition | Mechanism |
|---|---|
| Celiac disease | Villous atrophy → reduced absorptive surface |
| Pancreatic exocrine insufficiency | Deficient digestive enzymes (maldigestion) |
| Small intestinal bacterial overgrowth (SIBO) | Bacterial deconjugation of bile acids, carbohydrate fermentation |
| Short bowel syndrome | Reduced absorptive surface |
| Tropical sprue | Mucosal damage |
| Acarbose therapy | Inhibits carbohydrate absorption |
- Sleisenger and Fordtran's, p. 228-229; Frameworks for Internal Medicine, p. 205-206; Yamada's Textbook of Gastroenterology, p. 720
Clinical Features
- Stops with fasting - the hallmark of osmotic diarrhea; differentiates it from secretory diarrhea (which continues during fasting)
- No nocturnal diarrhea - diarrhea improves or stops overnight when patient is not eating; patients may avoid eating before long trips
- Watery stools with low electrolyte concentrations
- Steatorrhea (greasy, bulky, malodorous, hard-to-flush stools) if fat malabsorption is also present
- Weight loss when underlying malabsorption is present
- Bloating, flatulence, borborygmi when carbohydrate fermentation is the mechanism
Stool Osmotic Gap - The Key Diagnostic Test
Formula:
Stool Osmotic Gap = 290 mOsm/kg - 2 × (stool Na⁺ + stool K⁺)
Or if osmolality is directly measured:
Stool Osmotic Gap = Measured osmolality - 2 × (stool Na⁺ + stool K⁺)
| Gap | Interpretation |
|---|---|
| >100 mOsm/kg (or >125 by some sources) | Osmotic diarrhea - non-electrolyte solutes dominate |
| 50-100 mOsm/kg | Borderline |
| <50 mOsm/kg | Secretory diarrhea - electrolytes account for virtually all osmolality |
Why stool Na⁺ is low in osmotic diarrhea: Active Na⁺ absorption at the colon continues normally; the retained water is driven by non-electrolyte solutes, so stool Na⁺ is characteristically <60 mmol/L.
Note on factitious diarrhea: If surreptitious dilution of the stool sample is suspected, directly measure stool osmolality - unexpectedly high osmolality (>600 mOsm/kg) suggests contamination with urine.
- Yamada's Textbook of Gastroenterology, p. 720; Frameworks for Internal Medicine, p. 205
Osmotic vs. Secretory Diarrhea - Comparison
| Feature | Osmotic | Secretory |
|---|---|---|
| Response to fasting | Stops | Continues |
| Nocturnal symptoms | Rare | Present |
| Stool osmotic gap | >100 mOsm/kg | <50 mOsm/kg |
| Stool Na⁺ | <60 mmol/L | >90 mmol/L |
| Stool electrolytes | Normal absorption intact | Impaired |
| Volume | Moderate (related to intake) | Often large |
Diagnostic Approach
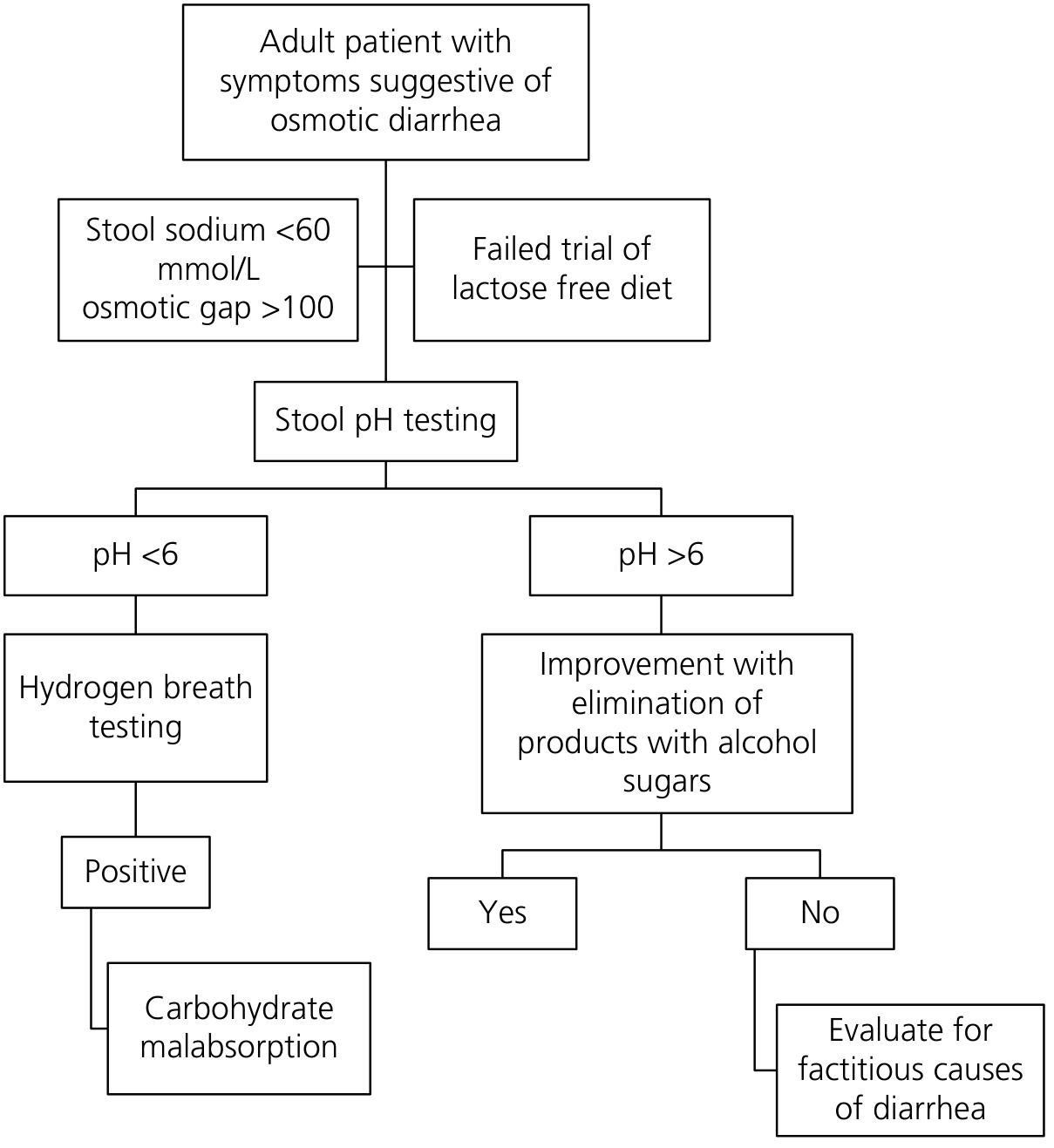
Step-by-step workup (Yamada's algorithm):
- Confirm osmotic diarrhea: stool Na⁺ <60 mmol/L + osmotic gap >100 mOsm/kg
- Trial of lactose-free diet - if no improvement:
- Check stool pH:
- pH <6 → Hydrogen breath testing (positive = carbohydrate malabsorption)
- pH >6 → Trial of elimination of products with alcohol sugars (sorbitol, mannitol, xylitol)
- Improves → sugar alcohol ingestion confirmed
- No improvement → evaluate for factitious causes
Additional tests:
- D-xylose absorption test: Detects small intestinal mucosal malabsorption (not useful for pancreatic insufficiency, as xylose doesn't need pancreatic enzymes); false positives in renal dysfunction and SIBO
- Hydrogen breath test: Patient fasts 8-12 h, ingests lactose or fructose, expired H₂/CH₄ measured every 15-30 min for 2-3 hours - elevation indicates bacterial fermentation of unabsorbed carbohydrate
- Stool magnesium: >15 mmol/day (or >44 mmol/L) strongly suggests magnesium-induced diarrhea
- Stool phosphate: >15 mmol/day suspicious for phosphate-induced diarrhea
Management
Principle: identify and eliminate the causative agent.
-
Dietary modification: lactose-free diet (lactase deficiency), low-FODMAP diet, elimination of sugar alcohols, reduced fructose intake
-
Stop the offending medication/supplement (Mg antacids, lactulose, PEG)
-
Treat underlying malabsorption:
- Celiac disease: gluten-free diet
- Pancreatic exocrine insufficiency: pancreatic enzyme replacement
- SIBO: antibiotics (rifaximin, metronidazole) + treat underlying anatomic/motility cause + correct nutritional deficiencies
- Short bowel syndrome: dietary optimization, octreotide, intestinal rehabilitation
-
Sleisenger and Fordtran's, p. 228-229; Yamada's Textbook of Gastroenterology, p. 720
Key take-home points:
- Osmotic diarrhea stops with fasting - this is the most reliable clinical clue
- Stool osmotic gap >100 mOsm/kg confirms osmotic mechanism
- Low stool Na⁺ (<60 mmol/L) and low stool pH (<6 in carbohydrate malabsorption) are supporting findings
- The three broad causes are: osmotic laxatives/ions, poorly absorbed carbohydrates/polyols, and generalized malabsorption
- Treatment is always directed at eliminating or correcting the underlying cause
What is stool osmotic gap
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Excellent - comprehensive detail from three authoritative sources. Here is the full explanation:
Stool Osmotic Gap
The Core Concept
Normal stool fluid is in osmotic equilibrium with plasma, which has an osmolality of approximately 290 mOsm/kg. This total osmolality must be "explained" by the solutes present. The question the osmotic gap answers is:
Are the solutes in stool mostly electrolytes (Na⁺, K⁺, and their anions), or are there significant non-electrolyte solutes present that we haven't directly measured?
Formula
Stool Osmotic Gap = 290 mOsm/kg − 2 × (Stool Na⁺ + Stool K⁺)
- 290 mOsm/kg is used as a fixed assumed value for stool osmolality (equal to plasma), because stool is always in osmotic equilibrium with body fluids
- 2 × accounts for the paired anions (Cl⁻, HCO₃⁻, etc.) that accompany each cation - stool fluid is electrically neutral, so each cation has an accompanying anion
- The result represents the osmolality not explained by electrolytes - i.e., the "gap" filled by unmeasured, non-electrolyte solutes
Why NOT measure stool osmolality directly?
Because bacterial fermentation continues in vitro after collection, causing stool osmolality to rise artificially. The directly measured value is therefore unreliable. The assumed value of 290 mOsm/kg is used instead. The one exception: direct measurement is useful to detect factitious diarrhea - if osmolality is unexpectedly <290 mOsm/kg, the sample has been diluted with water or hypotonic urine.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 235
Interpretation
| Stool Osmotic Gap | Interpretation |
|---|---|
| >125 mOsm/kg | Clearly osmotic - large amount of non-electrolyte solutes present |
| >100 mOsm/kg | Osmotic (Yamada's cutoff) |
| >50 mOsm/kg | Consistent with osmotic etiology (Tietz/Frameworks cutoff) |
| 50-125 mOsm/kg | Normal range |
| <50 mOsm/kg | Secretory diarrhea - electrolytes dominate stool osmolality |
Note: Different textbooks use slightly different cutoffs (50, 100, or 125 mOsm/kg) for the upper threshold. The Goldman-Cecil Medicine states the normal gap is 50-125 mOsm/kg. The key principle is directional: high gap = osmotic; low gap = secretory.
Why the Gap Differs Between Osmotic and Secretory Diarrhea
Secretory Diarrhea
The colon's normal electrolyte-absorbing capacity is overwhelmed. Stool water is rich in electrolytes, closely resembling plasma:
- Stool Na⁺ usually >90 mmol/L
- Stool K⁺ usually <10 mmol/L
- Stool HCO₃⁻ usually >50 mmol/L
- 2 × (Na⁺ + K⁺) approaches 290 mOsm/kg → gap is small (<50)
Osmotic Diarrhea
Normal electrolyte absorption continues at the colon. The water in the lumen is being held there by non-electrolyte solutes (unabsorbed Mg²⁺, sorbitol, undigested lactose, etc.). Electrolytes are actively reabsorbed, so:
- Stool Na⁺ is low (<60 mmol/L)
- The "unmeasured osmoles" (non-electrolyte solutes) explain the gap
- 2 × (Na⁺ + K⁺) is far less than 290 → gap is large (>100)
Worked Example
A patient with watery diarrhea has:
- Stool Na⁺ = 40 mmol/L
- Stool K⁺ = 25 mmol/L
Osmotic Gap = 290 − 2 × (40 + 25) = 290 − 130 = 160 mOsm/kg
→ Gap of 160 mOsm/kg → Osmotic diarrhea. There are 160 mOsm/kg of non-electrolyte solutes (e.g., sorbitol, Mg²⁺, undigested sugars) holding water in the lumen.
Additional Clues from Stool Chemistry
Once an elevated osmotic gap confirms osmotic diarrhea, further stool tests help identify the cause:
| Test | Finding | Implication |
|---|---|---|
| Stool pH | <5.5-6.0 | Carbohydrate malabsorption (colonic fermentation of unabsorbed sugars → short-chain fatty acids) |
| Stool pH | >6.0 | Osmotic laxatives (Mg, phosphate, sulfate) or generalized malabsorption |
| Stool Mg²⁺ | >45 mmol/L (>110 mg/dL) | Magnesium-induced diarrhea likely |
| Stool phosphate | >33 mmol/L (>102 mg/dL) | Phosphate laxative-induced diarrhea |
| Osmotic gap | Strongly negative | Sodium phosphate or sodium sulfate ingestion |
| Stool Cl⁻ | >100 mmol/L (adults) | Chloridorrhea |
| Stool osmolality (direct) | <290 mOsm/kg | Sample diluted with water/urine (factitious diarrhea) |
- Tietz Textbook of Laboratory Medicine 7th Edition, p. 1651; Goldman-Cecil Medicine, p. 1466
Summary Diagram (Conceptual)
Total stool osmolality = 290 mOsm/kg (fixed)
│
├── Explained by electrolytes: 2 × (Na⁺ + K⁺)
│
└── Unexplained = OSMOTIC GAP
│
├── Gap HIGH (>100): Non-electrolyte solutes dominant
│ → OSMOTIC diarrhea
│
└── Gap LOW (<50): Electrolytes dominant
→ SECRETORY diarrhea
Bottom line: The stool osmotic gap is a simple bedside calculation that separates osmotic from secretory diarrhea based on whether stool water osmolality is driven by electrolytes (secretory) or by unabsorbed non-electrolyte solutes (osmotic). It directly follows from the principle that stool is always isotonic with plasma.
This is a shared conversation. Sign in to Orris to start your own chat.