Say about hernia
Reading File
Finding Sources
Searching PubMed
hernia repair surgery
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of hernia, synthesized from Bailey and Love's Short Practice of Surgery (28th ed.), Roberts and Hedges' Clinical Procedures in Emergency Medicine, and Sleisenger and Fordtran's Gastrointestinal and Liver Disease.
Hernia
Definition
A hernia is the protrusion of any viscus from its normal cavity through an abnormal opening. Abdominal hernias involve intraabdominal contents (usually bowel or omentum) protruding through a defect in the abdominal wall musculature. The weakness may be congenital (a tract that failed to close) or acquired (age-related tissue laxity, raised intraabdominal pressure, wound healing failure, or trauma).
- Hernias develop in approximately 5% of men and 2% of women
- 75% of all hernias occur in the groin
Types of Hernia
Groin (Inguinal) Hernias
The most common hernia overall, about 10 times more common in men than women.
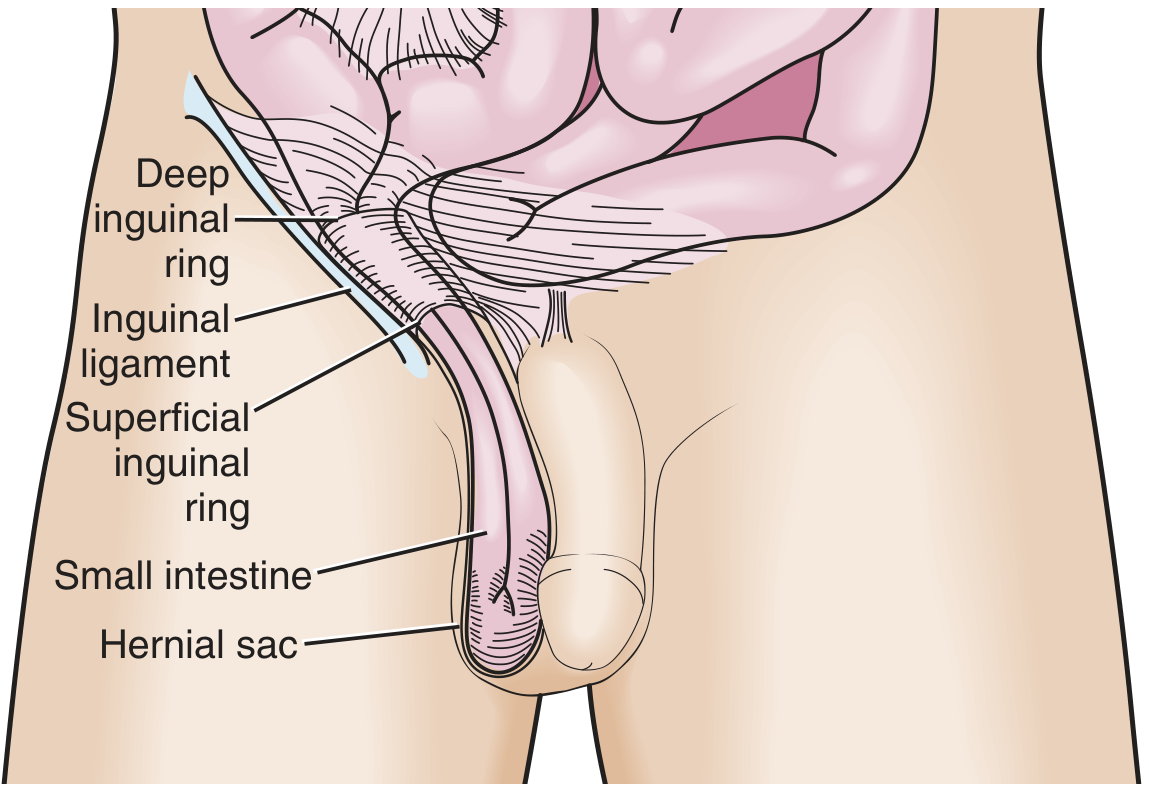
1. Indirect Inguinal Hernia (Lateral)
- Passes through the deep inguinal ring, travels along the inguinal canal, and may descend into the scrotum
- Can be congenital (patent processus vaginalis) or acquired
- On examination: controlled by pressure over the deep inguinal ring (midpoint of inguinal ligament)
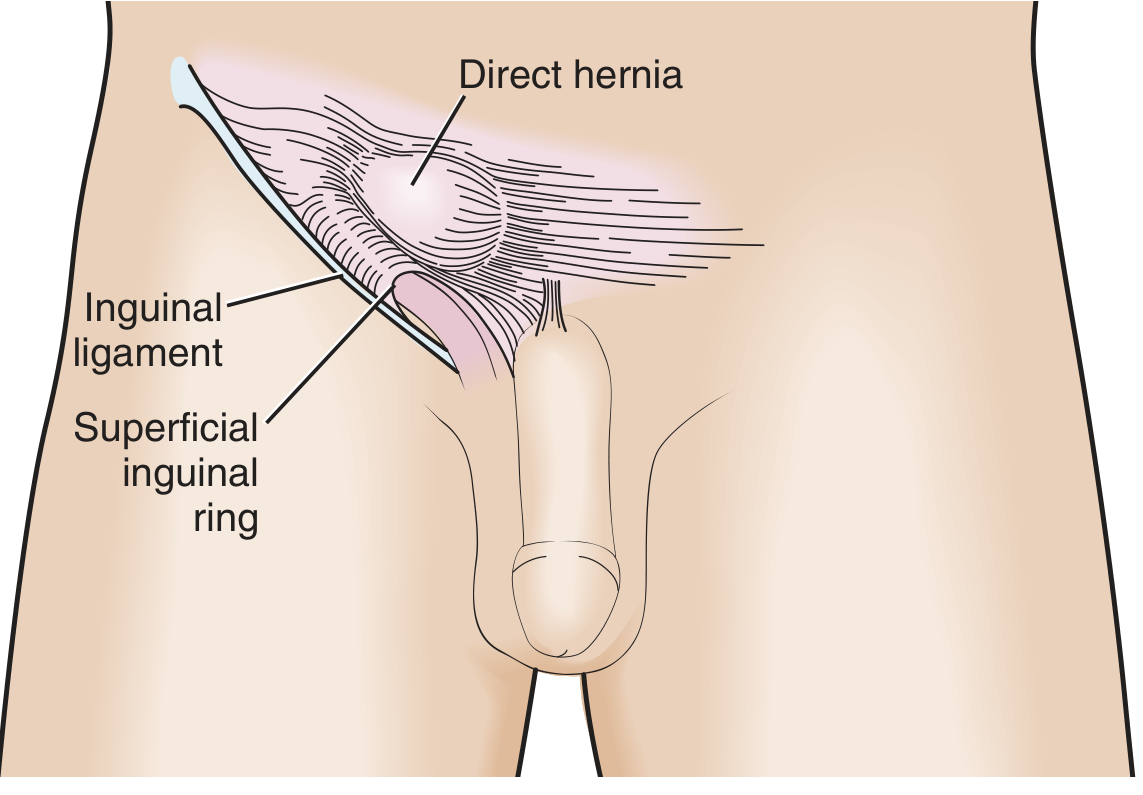
2. Direct Inguinal Hernia (Medial)
- Protrudes through the posterior wall of the inguinal canal medial to the inferior epigastric vessels (Hesselbach's triangle)
- Always acquired; caused by weakening of the transversalis fascia
- Does not descend into the scrotum and has a lower strangulation risk
- On examination: bulges medial to the deep inguinal ring despite finger pressure there
3. Pantaloon Hernia
- A combined direct + indirect hernia straddling the inferior epigastric vessels
- Difficult to diagnose in the ED and to sustain manual reduction; often only confirmed surgically
Femoral Hernia
- Passes inferior to the inguinal ligament through the femoral canal (medial to femoral vein, lateral to lacunar ligament)
- More common in women; presents as a medial thigh mass below the groin crease
- Has a small fascial defect - incarceration occurs in up to 45% of cases, making early repair important
Ventral (Abdominal Wall) Hernias
| Type | Key Feature |
|---|---|
| Incisional | Occurs in ~1 in 5 patients after abdominal surgery; 20-50% recurrence after repair |
| Umbilical | Traverses the fibrous tissue at the umbilicus; accounts for ~15% of emergency hernia surgery, with up to 60% showing strangulation at operation |
| Epigastric | Through the linea alba above the umbilicus |
| Spigelian | Through the semilunar line at the lateral border of rectus abdominis |
| Paraumbilical | Just above or below the umbilicus; distinct from true umbilical hernias |
Internal Hernias
- Hernias at an opening in the peritoneum, mesentery, or omentum
- Congenital types: mostly paraduodenal or through the foramen of Winslow
- Most common type is iatrogenic - following Roux-en-Y gastric bypass, colectomy, or pancreaticoduodenectomy
- May also herniate into the obturator canal or sciatic notch (rare)
Pathological States of a Hernia
| State | Description |
|---|---|
| Reducible | Contents can be returned to the abdominal cavity spontaneously or manually |
| Irreducible / Incarcerated | Contents cannot be reduced; does not automatically imply strangulation |
| Obstructed | Bowel in the sac is obstructed but blood supply is intact |
| Strangulated | Blood supply is compromised - a surgical emergency |
- Smaller hernia necks carry a greater strangulation risk (more constriction)
- Up to 40% of femoral hernias are strangulated at first presentation vs only ~2% of incisional hernias
- Among all SBO patients taken to surgery, incarcerated hernia causes intestinal ischemia in up to 75% and necrosis in over 25%
Diagnosis
Clinical - most hernias are diagnosed by history and examination:
- A reducible lump that appears on standing/Valsalva and disappears on lying
- Cough impulse is a hallmark
- Pain and tenderness suggest incarceration or strangulation
Imaging (when clinical diagnosis is uncertain):
- Ultrasound: useful for inguinal hernias, high PPV for inguinal location
- CT scan: best for obese patients, internal hernias, and cases of bowel obstruction where the cause is unclear
Key ED questions to answer (Roberts & Hedges):
- Is the palpable mass truly a hernia?
- Is it reducible or incarcerated?
- Is the bowel strangulated?
Differential Diagnosis (groin swellings)
- Lymphadenopathy
- Femoral artery aneurysm / psoas abscess
- Saphena varix (has cough impulse - can mimic hernia)
- Lipoma
- Hydrocele / testicular swelling
Treatment
Conservative
- Asymptomatic or minimally symptomatic hernias in elderly/frail patients may be observed
- A chronically incarcerated hernia without obstruction or change in symptoms is not necessarily an emergency
Manual Reduction (ED)
- Applicable to easily incarcerated (non-strangulated) hernias
- More reliable in groin and umbilical hernias
- Contraindicated if there is severe tenderness, skin erythema, or other signs of strangulation
Surgical Repair
Surgery is the definitive treatment. Approaches:
Open techniques:
- Bassini / Shouldice repair - tissue repair, reapproximating the posterior wall without mesh; Shouldice is currently considered equivalent to mesh in certain settings
- Lichtenstein tension-free mesh repair - the most widely performed open operation for inguinal hernia in high-income countries; 8×15 cm polypropylene mesh placed behind the spermatic cord; lower recurrence than tissue repair but chronic pain reported in up to 20% of patients
Laparoscopic techniques:
- TEP (Totally ExtraPeritoneal) - mesh placed extraperitoneally without entering the peritoneal cavity
- TAPP (TransAbdominal PrePeritoneal) - peritoneal cavity entered, then mesh placed preperitoneally
- Both use a 10×15 cm (or larger) mesh; advantages include reduced chronic pain and faster return to activity vs open repair
- A 2024 Cochrane review (PMID 38963034) compared TAPP vs TEP and found both to be effective; TAPP had slightly higher risk of port-site hernia while TEP had slightly higher conversion rates
Mesh types:
- Synthetic non-absorbable (polypropylene) - workhorse
- Biological (e.g., porcine/bovine derived) - for contaminated fields
- Slowly absorbable synthetic - emerging; long-term outcomes not yet established
- Intraperitoneal mesh placement is now avoided where possible due to adhesion, erosion, and fistula risk
European Hernia Society Classification (for operative planning):
- Primary (P) or Recurrent (R)
- Lateral (L), Medial (M), or Femoral (F)
- Defect size in fingerbreadths: 1 = <1.5 cm, 2 = 1.5-4.5 cm, 3 = >4.5 cm
- Example: primary indirect inguinal hernia with 3-cm defect = PL2
Key Epidemiological Points
- Hernia repair is among the most common surgical procedures worldwide
- Routine elective repair has significantly reduced the proportion of SBO cases caused by incarcerated hernias in Western countries
- Hernia accounts for 44.5% of all operations performed for acute small bowel obstruction in some series
Sources: Bailey and Love's Short Practice of Surgery (28th ed.), p. 1087-1092; Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1038-1042; Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 2495
This is a shared conversation. Sign in to Orris to start your own chat.