Collapse of lung lobes and thier findings in x ray and ct
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
I have everything needed for a comprehensive, well-illustrated answer. Here it is:
Collapse of Lung Lobes: X-Ray and CT Findings
Source: Grainger & Allison's Diagnostic Radiology; Goldman-Cecil Medicine
General Principles of Lobar Collapse
Direct signs of volume loss:
- Displacement of fissures (the most reliable early sign)
- Crowding of pulmonary vessels and bronchi within the collapsed lobe
- Hilar elevation (upper lobe collapse) or hilar "smallness" (lower lobe collapse)
- Bronchial reorientation: the ipsilateral main bronchus becomes more horizontal in upper lobe collapse; more vertical in lower lobe collapse
Indirect signs:
- Compensatory hyperinflation of adjacent lobes (fewer, more widely spaced vessels)
- Mediastinal shift toward the collapsed lobe
- Diaphragmatic elevation (especially with lower lobe collapse)
- Displacement of the anterior junctional line contralaterally
A collapsed lobe appears dense due to retained secretions/fluid plus loss of aeration. Near-complete collapse is needed before the lobe becomes radiographically opaque.
Schematic Overview
This diagram shows the position of each collapsed lobe on frontal and lateral projections:
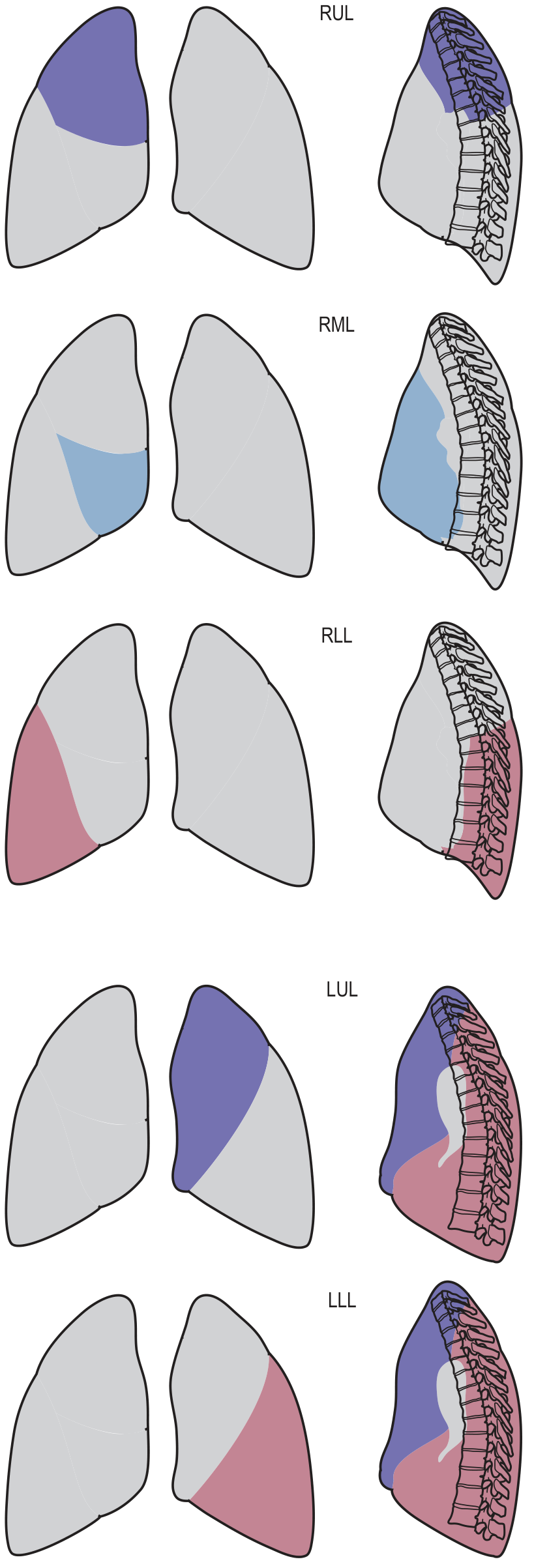
1. Right Upper Lobe (RUL) Collapse
X-Ray (PA):
- Upward displacement of the horizontal (minor) fissure
- Increased density in the right upper zone
- Right hilum elevation
- Tracheal deviation to the right
- Loss of right mediastinal border silhouette
- In "tight" collapse: a triangular wedge of soft tissue abuts the right mediastinum with a concave inferior margin (due to lower lobe hyperinflation) - the "Golden S-sign" when an underlying central mass causes the concavity
X-Ray (Lateral):
- Upward displacement of the horizontal fissure
- Anterior displacement of the upper part of the oblique fissure
CT:
- Triangular wedge of soft tissue anteriorly in the right hemithorax adjacent to the right mediastinum
- The collapsed lobe wraps around the superior mediastinum
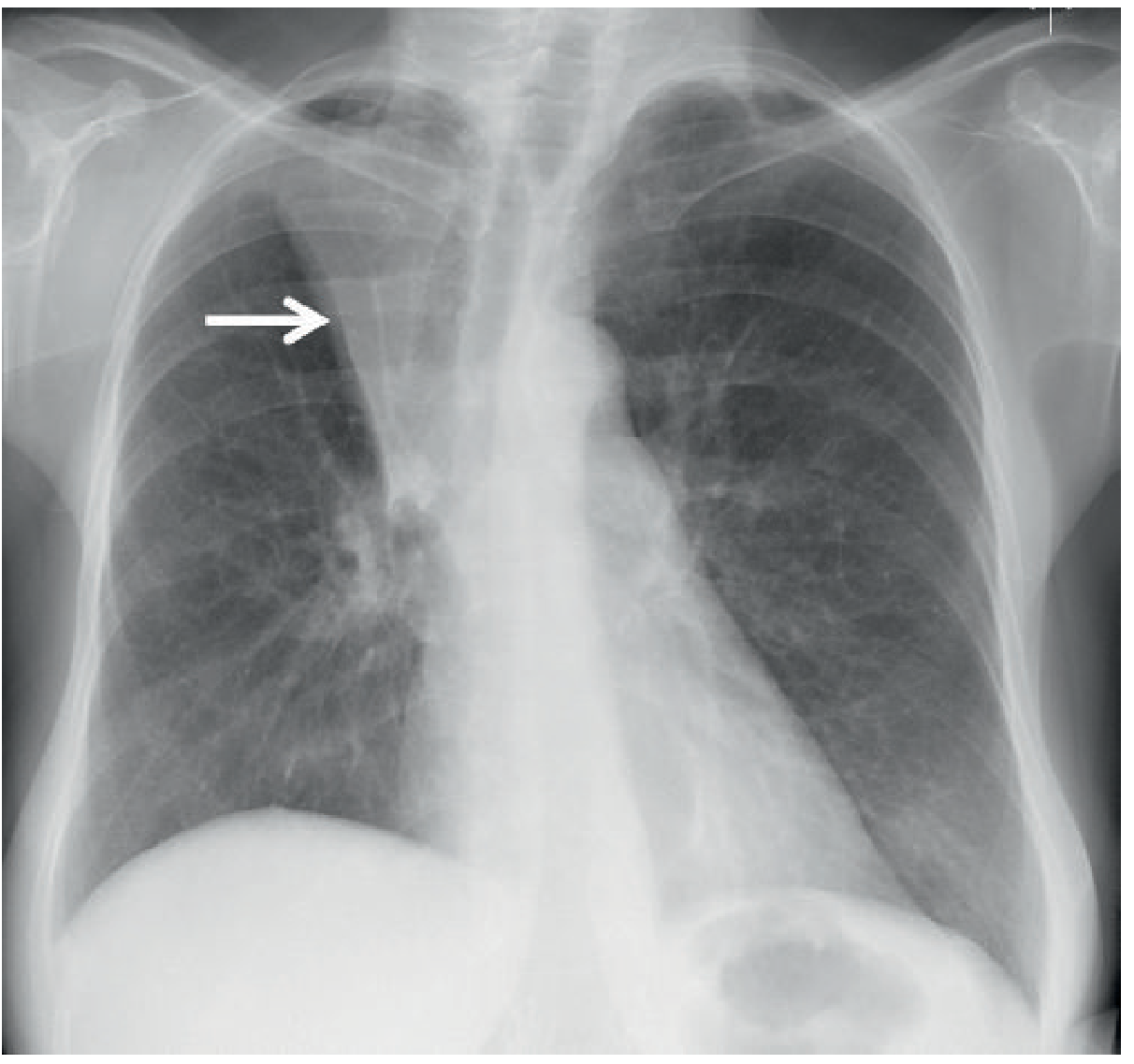
Fig. 7.19 - Tight Right Upper Lobe Collapse. The collapsed lobe (central bronchogenic carcinoma) results in increased right paramediastinal density (arrow).
2. Right Middle Lobe (RML) Collapse
X-Ray (PA):
- Ill-defined density at the right heart border (loss of right heart border silhouette - positive silhouette sign)
- Often subtle and easily missed
- Small triangular opacity in the right lower zone adjacent to the right heart border
X-Ray (Lateral):
- Wedge-shaped opacity between the horizontal and oblique fissures that converge anteriorly - the classic "bowtie" or "triangular" opacity with an anterior apex
CT:
- Band-like or wedge of soft tissue at the right cardiophrenic angle
- Fissures bow toward each other medially/anteriorly
3. Right Lower Lobe (RLL) Collapse
X-Ray (PA):
- Triangular density in the right lower zone medially, behind the heart
- Loss of silhouette of the medial right hemidiaphragm
- Right hilum "appears small" (interlobar artery obscured by opaque lobe)
- Right hemidiaphragm may be elevated
X-Ray (Lateral):
- Triangular density posteriorly
- Loss of the posterior right hemidiaphragm silhouette
- Vertebral column appears progressively denser inferiorly (important sign - normally the reverse is true)
- Posterior displacement of the oblique fissure
CT:
- Collapsed lobe lies in the posteromedial right hemithorax
- CT mucous bronchogram sign: tubular, low-attenuation branching airways within the enhancing collapsed lobe (on contrast-enhanced CT)
4. Left Upper Lobe (LUL) Collapse
This is distinctly different from RUL collapse because the left lung has no horizontal fissure.
X-Ray (PA):
- "Veil-like" increased density over the entire left hemithorax, greatest at the hilum (not a sharp margin)
- Loss of left heart border silhouette (lingula collapses anteriorly)
- Variable loss of the aortic knuckle silhouette
- Tracheal deviation to the left
- Left hilum elevation with increased angulation of the left main bronchus
- Luftsichel sign: a crescent of lucency (aerated superior segment of the left lower lobe) alongside the aortic knuckle, separating the aortic arch from the collapsed upper lobe
X-Ray (Lateral):
- Anterior displacement of the oblique fissure (toward the sternum)
- Increased retrosternal lucency (lower lobe hyperinflates anteriorly)
CT:
- Collapsed lobe forms a flat, broad band of soft tissue anteriorly against the chest wall and mediastinum
- Oblique fissure sweeps anteriorly
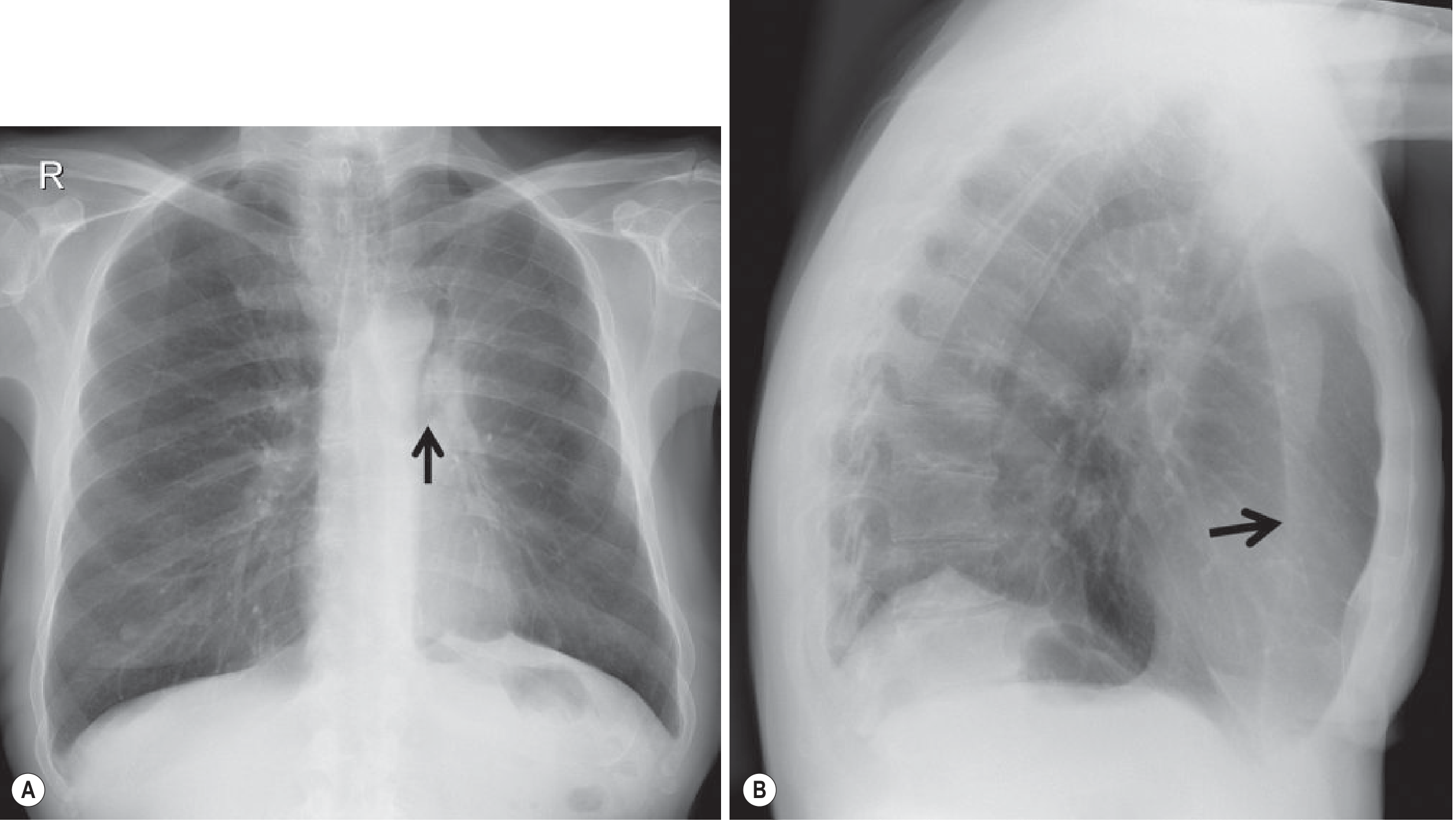
Fig. 7.21 - Left Upper Lobe Collapse. (A) Frontal view: increased angulation of left main bronchus (arrow). (B) Lateral view: anterior displacement of the oblique fissure (arrow) with increased retrosternal lucency.
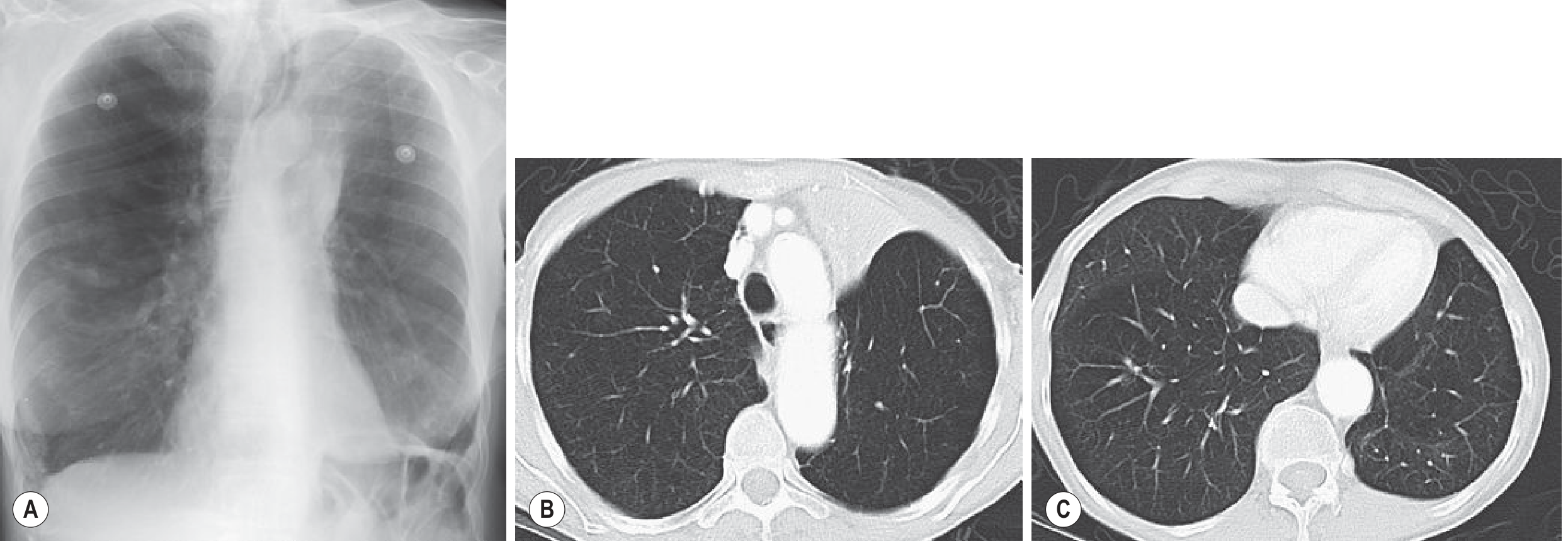
Fig. 7.22 - Atypical LUL Collapse on CXR and CT.
5. Left Lower Lobe (LLL) Collapse
Very similar in appearance to RLL collapse.
X-Ray (PA):
- Triangular density medially in the left lower zone (behind the heart)
- Loss of silhouette of the medial left hemidiaphragm
- Left hemidiaphragm may be elevated
- Loss of the descending aorta outline in severe collapse
X-Ray (Lateral):
- Triangular density posteriorly
- Loss of the posterior left hemidiaphragm silhouette
- Vertebral column appears progressively denser inferiorly
CT:
- Collapsed lobe in the posteromedial left hemithorax
- Oblique fissure displaced posteriorly and medially
6. Whole Lung Collapse
X-Ray:
- Complete opacification ("white-out") of the hemithorax
- Marked volume loss - ipsilateral mediastinal shift (this helps distinguish it from large pleural effusion, which shifts the mediastinum away)
- Contralateral lung expands across the midline anteriorly
- On lateral: marked anterior hyperlucency (contralateral lung displacement greatest anteriorly)
CT-Specific Signs Across All Lobes
| Sign | Significance |
|---|---|
| CT mucous bronchogram | Tubular low-attenuation airways in collapsed lobe - often indicates obstructive cause |
| Strong homogeneous enhancement | Favors atelectasis over consolidation/pneumonia (pneumonia shows less enhancement with air bronchograms) |
| Air bronchogram on CT | Does NOT exclude obstructive collapse (unlike plain film rules) |
| Fissure displacement | Best appreciated on coronal/sagittal reformats |
| Mediastinal anatomy | CT clarifies lymphadenopathy and causative masses |
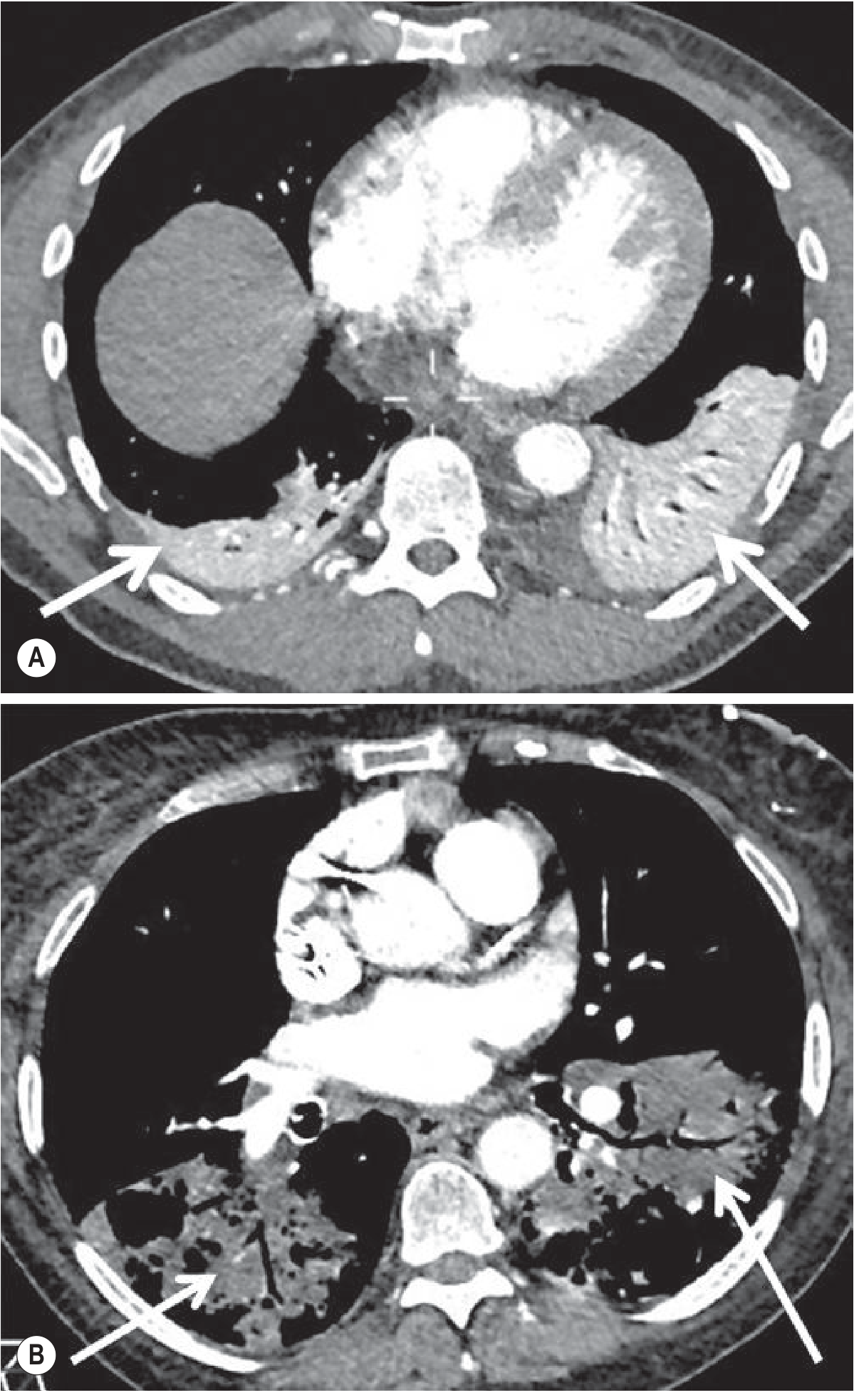
Fig. 7.12 - Enhancement pattern on contrast CT: Atelectasis (A) = dense homogeneous enhancement; Pneumonia (B) = relative lack of enhancement with air bronchograms.
Quick Summary Table
| Lobe | Fissure Movement | Opacity Location (PA) | Key Signs |
|---|---|---|---|
| RUL | Horizontal fissure - upward; upper oblique - anterior | Right upper zone / paramediastinal | Golden S-sign, hilar elevation, tracheal shift right |
| RML | Horizontal fissure - down; oblique - anterior/up | Right heart border (lateral wedge) | Right heart border silhouette loss, lateral wedge sign |
| RLL | Oblique fissure - posterior/medial | Behind heart, medial right lower zone | Medial diaphragm loss, vertebrae denser inferiorly |
| LUL | Oblique fissure - anterior | Veil over left hemithorax | Luftsichel sign, anterior fissure shift, retrosternal lucency |
| LLL | Oblique fissure - posterior/medial | Behind heart, medial left lower zone | Medial diaphragm loss, vertebrae denser inferiorly |
| Whole lung | All fissures invisible | Total hemithorax white-out | Ipsilateral mediastinal shift, anterior hyperlucency on lateral |
Grainger & Allison's Diagnostic Radiology, pp. 181-194; Goldman-Cecil Medicine, pp. 918-919
This is a shared conversation. Sign in to Orris to start your own chat.