Explain internuclear opthalmoplegia to me in clear English
Reading File
Finding Sources
Finding Sources
Searching Images
internuclear ophthalmoplegia eye movement diagram
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have comprehensive information from multiple authoritative textbooks and excellent images. Here's a clear explanation:
Internuclear Ophthalmoplegia (INO)
The Simple Version
INO is a disconnection syndrome — the "cable" linking the two halves of your horizontal gaze system gets cut. The result: one eye can't follow the other when you look sideways.
The Normal Wiring First
To move both eyes together to the right, your brain does this:
- The frontal eye fields (cortex) send a signal down to the brainstem
- It reaches the PPRF (paramedian pontine reticular formation) in the pons — the horizontal gaze centre
- The PPRF activates the abducens nucleus (CN VI) on the right, which pulls the right eye outward (abduction) via the right lateral rectus
- At the same time, a branch of that same signal crosses over and travels up through a tract called the medial longitudinal fasciculus (MLF) to the oculomotor nucleus (CN III) in the midbrain, which pulls the left eye inward (adduction) via the left medial rectus
Both eyes move right simultaneously — conjugate gaze.
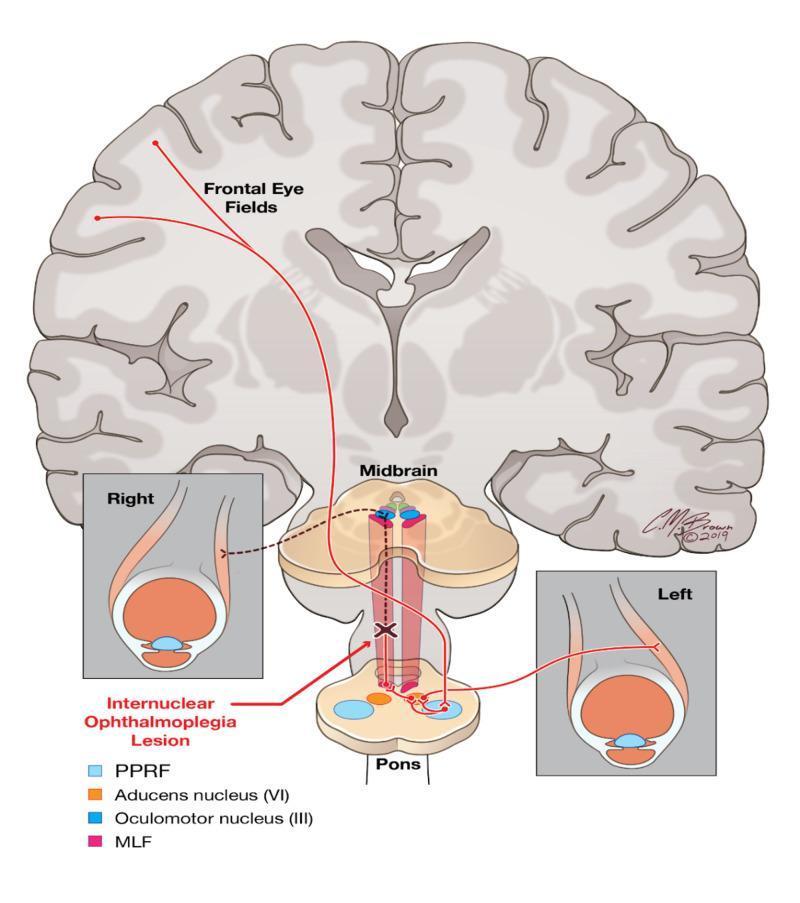
What Goes Wrong in INO
The MLF gets damaged — usually by MS or a small stroke. The abducens nucleus fires normally, the outer eye abducts fine, but the internuclear message never reaches the opposite oculomotor nucleus. The inner eye fails to adduct (move toward the nose), while the outer eye often develops a jerky nystagmus as it reaches full abduction.
The lesion is named for the side of the adduction failure. So a left INO means the left MLF is damaged, and the left eye won't adduct when looking right.
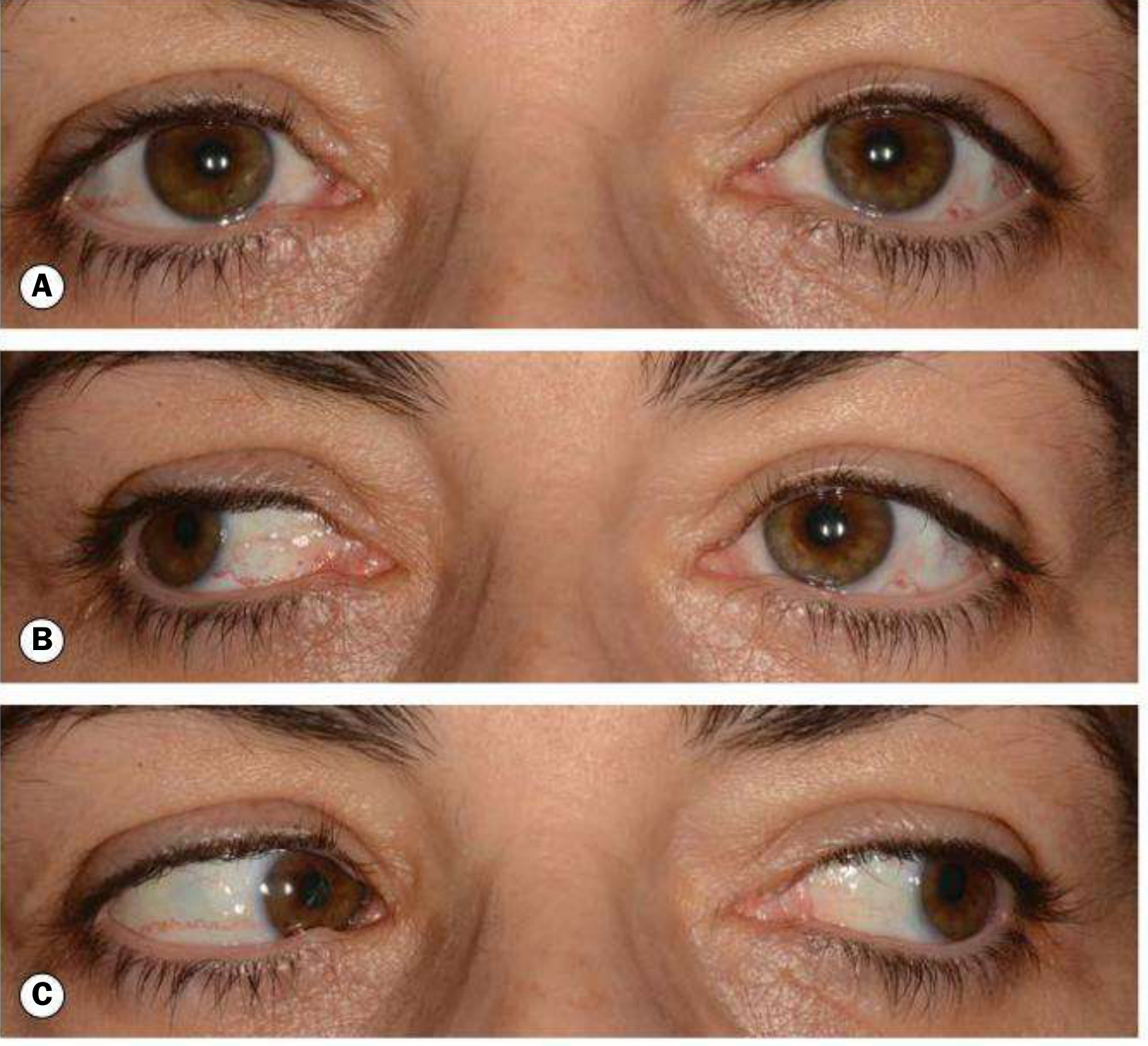
Key Clinical Features
| Feature | What you see |
|---|---|
| Primary position | Eyes usually straight |
| Lateral gaze to opposite side | Adduction failure of the affected eye |
| Abducting eye | Nystagmus (compensatory overshoot) |
| Convergence | Often preserved if the lesion is discrete and anterior (the convergence pathway uses a different route) |
| Symptoms | Often none — many patients don't notice. Some get diplopia or oscillopsia (visual jiggling) |
Variants
- Bilateral INO: Both MLFs are damaged — adduction fails in both directions. Classic in MS in young adults. The presence of bilateral INO in a young person is considered virtually diagnostic of MS.
- WEBINO (Wall-Eyed Bilateral INO): A rostral lesion also knocks out convergence, leaving both eyes drifted outward.
- One-and-a-half syndrome: The MLF and the ipsilateral PPRF are both damaged. The result is a gaze palsy to one side plus an INO — only one movement remains: abduction of the opposite eye.
Causes
| Age group | Common causes |
|---|---|
| Young adults | Multiple sclerosis (demyelination of the MLF) |
| Older adults | Brainstem stroke (small perforating artery infarct) |
| Any age | Trauma, tumour, vasculitis, Wernicke's encephalopathy |
About one-third of cases are each: stroke, MS, and other causes. — Bradley and Daroff's Neurology in Clinical Practice
Mimics to Rule Out
INO can be mimicked by things that weaken the medial rectus without damaging the MLF:
- Myasthenia gravis — fatigable weakness of the medial rectus
- Third nerve palsy — but usually comes with ptosis and pupil changes
- Thyroid eye disease — restrictive myopathy
- Miller Fisher / Guillain-Barré syndrome
The key distinguishing feature: in true MLF-INO, convergence is intact (both medial recti work on the convergence pathway). In myasthenia or CN III palsy, convergence is also impaired.
Investigation & Management
- MRI with thin brainstem cuts is the imaging of choice (the MLF lesion can be tiny and easily missed on standard cuts)
- Treat the underlying cause (MS disease-modifying therapy, stroke management)
- Most INO from MS resolves partially or fully with time
- Persistent diplopia can be managed with prism glasses or, in some cases, strabismus surgery
Sources: Bradley and Daroff's Neurology in Clinical Practice; Kanski's Clinical Ophthalmology, 10th ed.; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.