pseudomonas eradication therapy in bronchiectasis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Pseudomonas aeruginosa" AND "bronchiectasis" AND eradication
Reading File
Reading Article
PMID: 38296344
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Loading Image
Reading Article
PMID: 40339664
Reading File
Reading File
Reading File
I now have sufficient content from both the textbook and recent meta-analyses. Let me compile the comprehensive answer.
Pseudomonas aeruginosa Eradication Therapy in Bronchiectasis (non-CF)
Why Eradication Matters
P. aeruginosa is the most frequently isolated pathogen in bronchiectasis and is independently associated with accelerated lung function decline, increased exacerbation frequency, greater disease severity (higher FACED and Bronchiectasis Severity Index scores), and increased mortality. Because P. aeruginosa can rapidly form biofilms and adopt a mucoid phenotype once established, early eradication at first or new isolation offers the best window for clearance. Once chronic colonization is established, eradication becomes far less likely.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 1590
When to Attempt Eradication
Eradication therapy is indicated at:
- First isolation of P. aeruginosa from sputum
- New isolation after a period of culture negativity
- New mucoid conversion (even in established colonization, aggressive eradication strategies may be considered)
A repeat sputum sample to confirm true persistent infection is reasonable before committing to a full course, since a single positive culture may represent transient colonization.
The Three Eradication Pathways (ERS-Based Algorithm)
The ERS guideline (Polverino et al., 2017) outlines three stepwise pathways, each with an initial phase of 2 weeks and a total course of 3 months:
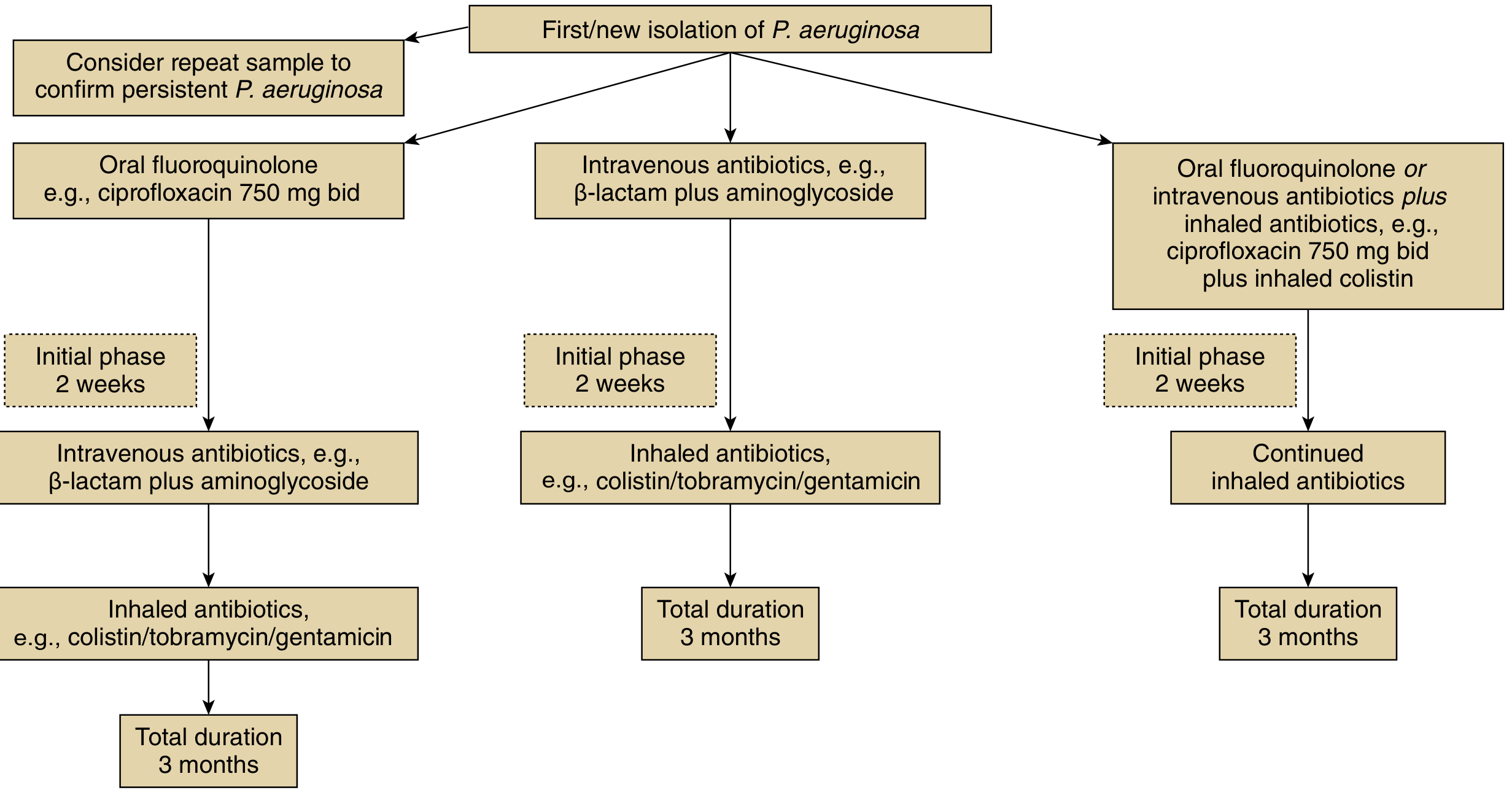
eFigure 69.14 - Murray & Nadel's Textbook of Respiratory Medicine
| Pathway | Initial phase (2 weeks) | Then (to complete 3 months) |
|---|---|---|
| A (Least intensive) | Oral fluoroquinolone - e.g., ciprofloxacin 750 mg BD | IV antibiotics (beta-lactam + aminoglycoside), then inhaled antibiotic (colistin/tobramycin/gentamicin) |
| B (Intermediate) | IV antibiotics - beta-lactam + aminoglycoside | Inhaled antibiotic (colistin/tobramycin/gentamicin) |
| C (Most intensive / preferred for resistant/recurrent) | Oral fluoroquinolone or IV antibiotics + inhaled antibiotic (e.g., ciprofloxacin 750 mg BD + inhaled colistin) | Continued inhaled antibiotics |
After each step, sputum culture is repeated; if still positive, escalation to the next pathway is recommended.
Antibiotic Choices in Detail
Systemic agents:
- Oral ciprofloxacin 750 mg BD - the most practical initial option; good pseudomonal activity and bioavailability
- IV beta-lactam + aminoglycoside (e.g., piperacillin-tazobactam or ceftazidime + tobramycin/gentamicin) - for severe disease, resistant strains, or when oral therapy has failed
- Sensitivity testing should always guide selection
Inhaled agents (for suppression/combination phase):
- Inhaled colistin (1 million IU nebulised)
- Inhaled tobramycin (300 mg/5 mL BD in alternating months, or continuous)
- Inhaled gentamicin (80 mg BD)
- Inhaled aztreonam and inhaled ciprofloxacin (liposomal) have been studied but are not currently approved for this indication
Evidence: How Well Does Eradication Work?
A 2024 systematic review and meta-analysis (Conceição et al., Eur Respir Rev, PMID: 38296344) - the most rigorous current evidence - found:
| Treatment | 12-month eradication rate |
|---|---|
| All eradication regimens (6 studies, n=289) | ~40% (95% CI 34-45%) |
| Combined systemic + inhaled antibiotics | ~48% (95% CI 41-55%) |
| Systemic antibiotics alone | ~27% (95% CI 13-45%) |
Key takeaway: Combined systemic + inhaled antibiotic therapy achieves meaningfully higher eradication rates than systemic alone. Even so, roughly 60% of patients remain culture-positive at 12 months, highlighting the difficulty of true eradication once P. aeruginosa is detected.
A 2025 meta-analysis of 9 RCTs (Zhong et al., Respir Med, PMID: 40339664) found inhaled tobramycin specifically:
- Significantly increased eradication rates (RR 2.42, 95% CI 1.57-3.74)
- Reduced hospital admissions (WMD -0.52)
- Did not significantly reduce exacerbation rates
- Was associated with higher adverse event-related discontinuation (RR 1.97) - mainly bronchoconstriction
After Eradication Attempt: Long-Term Management
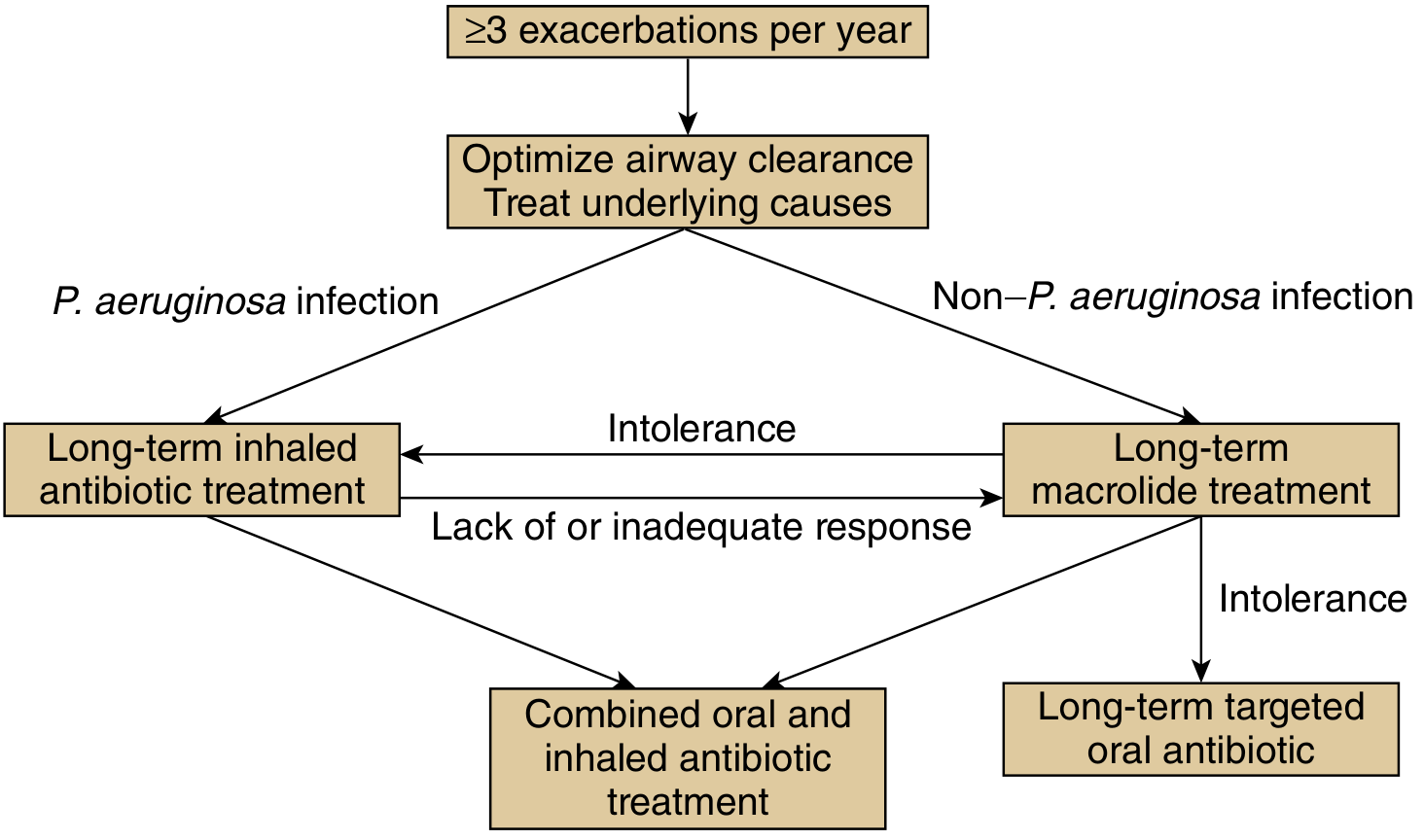
Figure 69.15 - Murray & Nadel's Textbook of Respiratory Medicine
For patients with >=3 exacerbations/year and P. aeruginosa infection, guidelines recommend:
- Long-term inhaled antibiotic treatment as first-line
- If inadequate response: add oral antibiotics (combined oral + inhaled)
- Macrolides are primarily used for non-P. aeruginosa organisms (given concerns about NTM activation and resistance selection with macrolides in Pa-positive patients)
Practical Considerations
| Issue | Guidance |
|---|---|
| Sensitivity testing | Mandatory before starting; use local antibiogram to guide choice |
| Bronchoconstriction | Pre-treat with inhaled bronchodilator before nebulised antibiotics; monitor first dose |
| Nephrotoxicity/ototoxicity | Monitor renal function and audiometry with aminoglycosides |
| Resistance emergence | Reassess cultures after each treatment phase; mucoid phenotype and multi-drug resistance are common failure modes |
| Vitamin D | Deficiency is associated with more frequent P. aeruginosa colonisation and faster decline - supplementation is reasonable |
| Repeat cultures | At 3 months post-treatment; sustained negativity over 12 months is the standard benchmark |
Summary
Eradication therapy is recommended at first/new isolation of P. aeruginosa in non-CF bronchiectasis, using a 3-month protocol combining initial systemic antibiotics (oral ciprofloxacin or IV beta-lactam + aminoglycoside) with inhaled antibiotics (colistin, tobramycin, or gentamicin). Combined systemic + inhaled regimens achieve ~48% 12-month eradication vs ~27% with systemic alone. Patients who remain colonised should transition to long-term inhaled antibiotic suppression therapy.
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 1590-1601
- Conceição et al. Eur Respir Rev 2024 [PMID 38296344]
- Zhong et al. Respir Med 2025 [PMID 40339664]
This is a shared conversation. Sign in to Orris to start your own chat.