Here is the fully elaborated, diagram-integrated answer for both questions.
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
QUESTION 1
Weight-Bearing & Resistance Exercises for Women with Osteoporosis — With Precautions
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
📌 INTRODUCTION
Osteoporosis is a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, leading to increased bone fragility and susceptibility to fractures. It is most prevalent in postmenopausal women due to estrogen deficiency, which disrupts the balance between bone formation (osteoblasts) and bone resorption (osteoclasts), tipping it in favor of net bone loss.
The fundamental biological principle governing exercise therapy is Wolff's Law: bone remodels and adapts its architecture in response to mechanical stresses placed upon it. When bone is mechanically loaded — whether through ground reaction forces during weight-bearing or through muscle tension during resistance training — osteoblasts are activated, collagen matrix is laid down, and mineralization follows, resulting in denser, stronger bone.
According to Harrison's Principles of Internal Medicine (21st ed., p. 11631): "Increased sex hormone production at puberty is required for skeletal maturation" — and conversely, its loss after menopause precipitates the bone remodeling imbalance central to osteoporosis.
Exercise is therefore not merely a lifestyle recommendation — it is a mechanobiological therapy that directly addresses the pathophysiology of osteoporosis.
🦴 THE OSTEOPOROTIC BONE — What Exercise Must Address
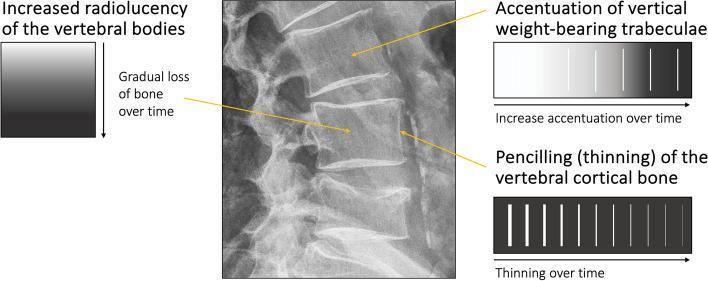
The X-ray below demonstrates the classic features of osteoporotic bone at the lumbar spine — including loss of horizontal trabeculae, increased radiolucency, and cortical thinning ("pencilling"). These are the structural changes that exercise aims to slow, halt, or partially reverse.
Lateral lumbar spine X-ray demonstrating osteopenia/osteoporosis: vertical trabecular accentuation (loss of horizontal trabeculae), generalized radiolucency, and cortical pencilling — structural changes targeted by weight-bearing and resistance exercise.
PART A: WEIGHT-BEARING EXERCISES
🔷 Definition
Weight-bearing exercises are performed in an upright position where the skeleton bears body weight against gravity. The ground reaction force (GRF) generated compresses the long bones of the lower limb, hip, and vertebral column — stimulating periosteal osteoblast activity and bone remodeling at the most fracture-vulnerable sites.
🔷 Classification by Impact Level
Weight-bearing exercises are classified according to the magnitude of ground reaction force generated — the greater the GRF, the more potent the osteogenic stimulus.
1. HIGH-IMPACT WEIGHT-BEARING EXERCISES
GRF > 1.5–3× body weight | Greatest osteogenic stimulus
Indication: Women with mild osteoporosis (T-score −1.0 to −2.5), NO vertebral fracture, good balance
| Exercise | Technique | Bone Site Targeted | Clinical Note |
|---|
| Jogging / Running | Light jog on flat surface, correct footwear, controlled pace | Hip, femoral neck, tibia, lumbar spine | Avoid uneven terrain; reduce pace if balance is impaired |
| Jumping / Skipping | Rope jumping, jumping jacks | Femoral neck, calcaneus, tibia | Even 10–50 jumps/day shown to improve hip BMD in controlled studies |
| Heel Drops | Stand erect, rise on tiptoes, then drop heels firmly to floor | Lumbar spine, hip | Simple, safe, evidence-based; 50 drops/day in protocol studies |
| Dancing | Aerobic dance, Zumba, ballroom | Hip, spine, entire lower limb | Multi-directional loading; improves balance and coordination simultaneously |
| Step Aerobics | Bench stepping synchronized to music | Hip extensors, knee, spine | Modifiable step height and tempo for progression |
| Stair Climbing | Climbing 2–4 flights; stair stepper machine | Hip, femoral neck, quadriceps | Functional, accessible, high compliance |
| Tennis / Racket Sports | Recreational play, doubles preferred | Dominant-side radius, humerus, hip | Unilateral loading; significant side-to-side BMD asymmetry documented in players |
2. LOW-IMPACT WEIGHT-BEARING EXERCISES
GRF ≤ 1× body weight | Lower but still beneficial bone stimulus
Indication: Severe osteoporosis (T-score < −2.5), existing vertebral fractures, kyphosis, arthritis, poor balance
| Exercise | Technique | Bone Site Targeted | Clinical Note |
|---|
| Brisk Walking | 3–5 km/h pace, upright posture, arm swing | Hip, femoral neck, lumbar spine | Most universally recommended; minimal fracture risk; easy to dose |
| Nordic Walking | Walking with bilateral poles | Upper + lower limb, trunk | Poles improve posture alignment; reduce joint loading |
| Tai Chi | Slow, flowing martial arts sequences | Hip, lower limb | Reduces falls by up to 47%; improves proprioception and dynamic balance |
| Elliptical Trainer | Continuous low-impact machine cardio | Hip, knee | No ground impact; ideal for arthritis or joint pain |
| Low-Impact Aerobics | Non-jumping aerobic routines in class | Hip, spine | Excellent group exercise; easy to modify |
⚠️ Important: Swimming and cycling, while excellent for cardiovascular health, are NOT weight-bearing and have minimal osteogenic effect — they cannot substitute for weight-bearing exercise in osteoporosis management.
🔷 Principles for Maximising Osteogenic Effect
(Osteoporosis Management Guidelines, p. 76)
| Principle | Explanation |
|---|
| High strain magnitude | Moderate-to-vigorous intensity — gentle strolling has minimal bone effect |
| Novel/varied loading | Multidirectional movements stimulate bone in multiple planes; bone adapts to new patterns |
| Short frequent bouts | Multiple short sessions per day are MORE beneficial than one long session |
| Progressive overload | Gradually increase intensity over weeks to maintain osteogenic stimulus |
| High frequency | Most days of the week for cumulative skeletal benefit |
PART B: RESISTANCE EXERCISES
🔷 Definition and Rationale
Resistance (strength) training involves working muscles against an external force — body weight, free weights, machines, or resistance bands. Muscle contractions generate tensile and compressive forces on the bones at their attachment sites, directly stimulating osteoblast activity. Additionally, stronger muscles act as biological shock absorbers, reducing force transmitted to bone during falls.
"The most important components of the exercise prescription for the prevention of osteoporosis are moderate- to high-intensity progressive resistance training in combination with weight-bearing impact exercise and challenging balance training."
— Osteoporosis Management and Fracture Prevention Guidelines (p. 79)
🔷 Resistance Training Parameters
(Evidence-Based — Osteoporosis Management Guidelines, p. 76)
| Parameter | Recommendation |
|---|
| Frequency | 2–3 times/week on non-consecutive days |
| Intensity | Begin 40–60% 1RM → progress to 70–85% 1RM |
| Sets | 2–3 sets per exercise |
| Repetitions | 8–10 repetitions per set |
| Exercises per session | ~8 exercises targeting major muscle groups |
| Rest between sets | 60–90 seconds |
| Progression | Increase load 5–10% when all reps completed with correct form — "Progressive Overload" |
🔷 Detailed Resistance Exercises by Region
1. 🟥 SPINAL EXTENSORS (Highest Priority)
Purpose: Strengthen the muscles that hold the spine upright; counteract kyphosis; reduce vertebral compression fracture risk
| Exercise | Start Position | Technique |
|---|
| Prone Back Extension | Lie face down, arms by sides | Lift chest off mat using back muscles; hold 3–5 sec; lower slowly |
| Prone Cobra | Face down, palms near shoulders | Retract shoulder blades, lift chest and arms off ground; excellent for thoracic extensors |
| Superman | Prone, arms extended overhead | Simultaneously lift both arms and both legs; hold 2–3 sec |
| Bird-Dog | 4-point kneeling on hands and knees | Extend opposite arm and leg simultaneously; maintain perfectly neutral spine |
| Seated Row (band/machine) | Seated upright, neutral spine | Pull handle to lower ribs; squeeze shoulder blades together; controls thoracic extensors |
2. 🟧 HIP AND GLUTEAL MUSCLES
Purpose: Prevent hip fractures; strengthen hip abductors, extensors, and external rotators
| Exercise | Technique | Key Point |
|---|
| Hip Bridge / Glute Bridge | Supine, knees bent 90°; press feet into floor; drive hips upward; hold 2–3 sec at top | Squeeze glutes at top; do not hyperextend lumbar spine |
| Side-Lying Hip Abduction | Lie on side; lift top leg 30–40°, toes pointing forward | Lower slowly (eccentric phase is key for strength) |
| Clamshell | Side-lying, hips/knees bent 45°; open top knee like a clam shell | Targets gluteus medius — critical for hip stability |
| Standing Hip Abduction (band) | Resistance band around ankles; lift leg sideways | Use wall for balance support |
| Step-Ups | Step onto a sturdy 15–20 cm platform with full hip extension at top | Control descent; increase step height as strength improves |
| Sit-to-Stand | Rise from chair without using hands; pause standing; lower slowly | Most functional exercise for lower limb strength |
3. 🟨 QUADRICEPS AND KNEE EXTENSORS
Purpose: Knee stability, fall prevention, stair climbing ability
| Exercise | Notes |
|---|
| Leg Press (machine) | Safest quad exercise — no axial spinal loading |
| Mini/Wall Squat | Depth 45–60°; back flat against wall; feet shoulder-width apart |
| Terminal Knee Extension (band) | Short arc quad activation; excellent for knee stability |
| Seated Leg Extension | Machine-based; isolated quad loading |
4. 🟩 UPPER BACK / POSTURAL MUSCLES
Purpose: Counteract kyphosis and forward-rounded shoulders; strengthen rhomboids and trapezius
| Exercise | Technique |
|---|
| Resistance Band Rows | Seated or standing; pull band to lower chest; retract shoulder blades fully |
| Lat Pulldown (machine) | Pull bar to upper chest — NOT behind the neck; controlled movement |
| Wall Angels | Stand against wall; slide arms from waist to overhead; activates lower trapezius |
| Scapular Retractions | Simply squeeze shoulder blades together; hold 5 sec; can be done anywhere, anytime |
5. 🟦 CORE STABILIZERS
Purpose: Protect the spine during all daily activities; reduce vertebral fracture risk during functional movement
| Exercise | Notes |
|---|
| Modified Forearm Plank | Maintain neutral spine — no sagging or arching; progress hold duration from 10 sec to 60 sec |
| Bird-Dog | Also listed above — functions as both back extensor AND core stabilizer |
| Dead Bug | Supine; alternate arm/leg extension; ensure lumbar spine stays flat on floor |
| Abdominal Bracing | Co-contract transversus abdominis and multifidus; key for functional spinal protection |
❌ STRICTLY AVOID: Crunches, sit-ups, Russian twists, V-sits — all involve repeated spinal flexion and dramatically increase vertebral fracture risk in osteoporotic women.
6. 🟪 CALF AND ANKLE
Purpose: Calcaneal bone loading; ankle stability for fall prevention
| Exercise | Notes |
|---|
| Bilateral Standing Heel Raises | Rise onto tiptoes fully; lower slowly; use wall for balance |
| Unilateral Heel Raises | Progress to single-leg once bilateral is comfortable |
| Seated Calf Raise | With weights across thighs; soleus targeting |
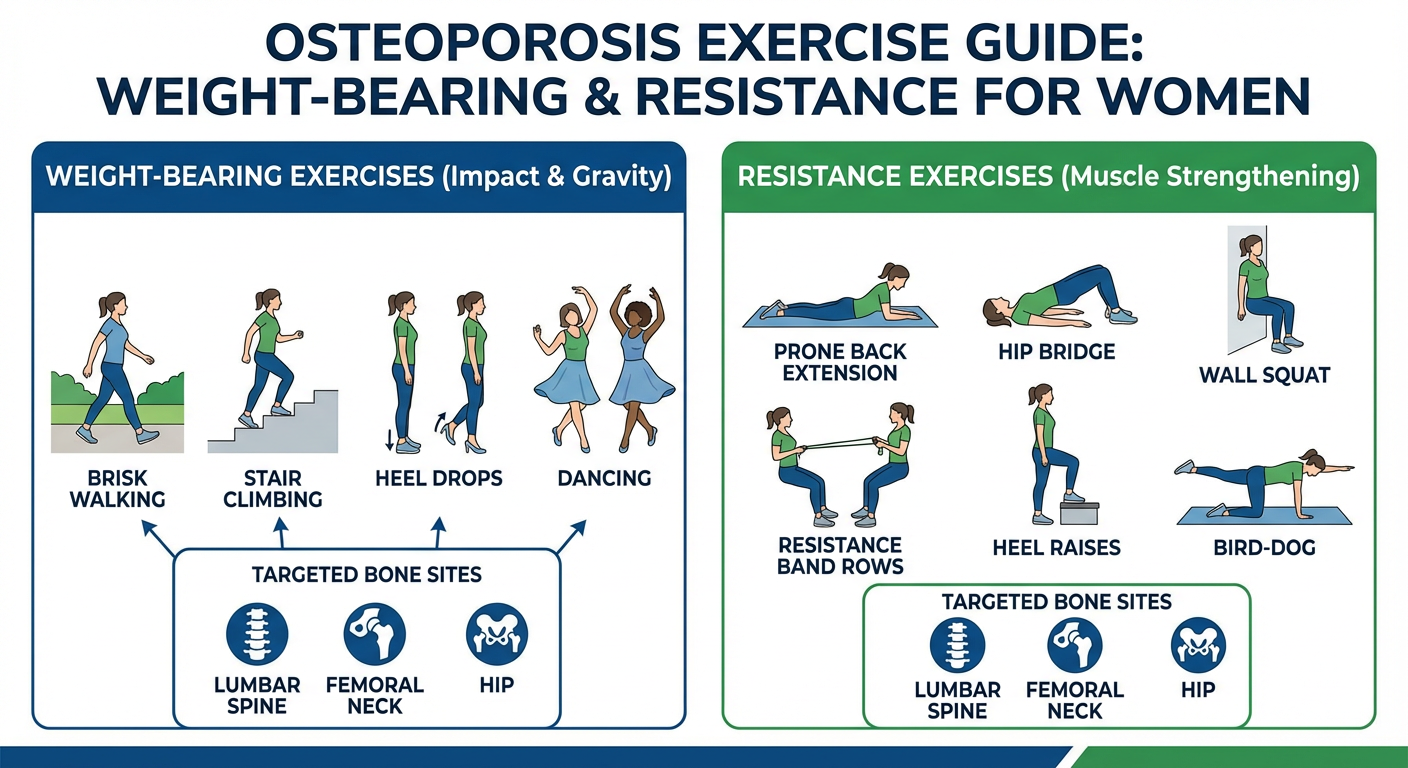
🔷 Exercise Diagram — Weight-Bearing & Resistance Exercises
Comprehensive exercise diagram for women with osteoporosis: weight-bearing exercises (brisk walking, stair climbing, heel drops, dancing) and resistance exercises (back extension, hip bridge, wall squat, bird-dog, resistance band rows, heel raises) with targeted bone sites labeled.
PART C: PRECAUTIONS — DETAILED AND COMPREHENSIVE
🚨 ABSOLUTE PRECAUTIONS (Must Avoid in ALL Women with Osteoporosis)
| ❌ Movement to Avoid | Biomechanical Reason | Example Activities to Avoid |
|---|
| Loaded spinal flexion | Compressive + anterior shear force on vertebral bodies → wedge fracture | Sit-ups, crunches, bent-over rows with rounded spine, picking up objects with bent back |
| Spinal rotation under load | Torsional forces exceed vertebral bone strength → burst fracture | Weighted trunk twists, golf swings with heavy loads |
| End-range forward bending | Even body weight creates dangerous vertebral loading | Toe-touch stretch, yoga child's pose, seated forward fold |
| Rapid uncontrolled movements | Cannot decelerate force if bone strength is reduced | Explosive jumps, jerky weight lifting, rapid directional changes |
| High-impact in severe osteoporosis / vertebral fracture | GRF exceeds fragile bone capacity → fracture | Jogging, jumping, aerobics jumping jacks |
| Hip flexion >90° + internal rotation (post-THR) | Hip dislocation risk | Deep squats, low chairs, crossing legs (Guidelines, p. 79) |
⚠️ CONDITIONAL / RELATIVE PRECAUTIONS
| Clinical Situation | Recommended Modification |
|---|
| Arthritis comorbidity | Prefer seated resistance over high-impact aerobics; reduce range of motion; modify load (Guidelines, p. 79) |
| Kyphosis | All exercises in extension-neutral or extension-biased position; back extension priority |
| Poor balance / gait impairment | RESOLVE balance and gait FIRST; balance training before progressing to ambulation (Guidelines, p. 79) |
| Frailty / severe deconditioning | Begin with chair-based exercises; progress slowly; very short session durations |
| Medications causing sedation | Exercise at times of peak cognitive alertness; avoid post-medication sedation windows (Guidelines, p. 79) |
| Visual/hearing impairment | Optimize aids; well-lit exercise space; supervision |
| Cardiovascular comorbidity | Medical clearance before vigorous exercise; monitor heart rate and symptoms |
| Osteoporotic fracture healing | Consult surgeon/physiotherapist before resuming exercise; protect healing site |
✅ SAFETY ENVIRONMENT CHECKLIST
(Osteoporosis Management Guidelines, p. 79)
- ✅ Adequate, non-glare lighting in exercise area
- ✅ Non-slip, supportive footwear with good ankle support
- ✅ Clear exercise space — remove rugs, cables, furniture corners
- ✅ Handrails or wall support during all balance exercises
- ✅ Supervision for initial program sessions
- ✅ Exercise at time of day when energy, cognition, and mood are optimal
- ✅ Avoid exercise when cognitively impaired, heavily sedated, or fatigued
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
QUESTION 2 (10-MARKER)
Detailed Exercise Prescription for Post-Menopausal Women with Osteoporosis
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
📌 INTRODUCTION
Post-menopausal osteoporosis (Type I osteoporosis) is the most prevalent form of metabolic bone disease globally, predominantly affecting women within 5–10 years after the final menstrual period. The cessation of ovarian estrogen production removes the primary suppressor of osteoclastic bone resorption. The resultant uncoupling of bone remodeling — increased resorption, inadequate formation — leads to accelerated trabecular bone loss at a rate of 2–5% per year in the early post-menopausal period.
The World Health Organization defines osteoporosis as a bone mineral density (BMD) T-score ≤ −2.5 at the femoral neck or lumbar spine on dual-energy X-ray absorptiometry (DEXA). The consequences are profound: 1 in 2 women over age 50 will sustain an osteoporotic fracture in their lifetime — hip, vertebral, and distal radius fractures being the most clinically significant.
Bone remodeling — the cyclical process of osteoclastic resorption followed by osteoblastic formation — is the mechanism through which exercise exerts its skeletal benefits. According to Harrison's Principles of Internal Medicine (21st ed., p. 11631): "Bone remodeling occurs throughout life so that most of the adult skeleton is replaced about every 10 years." Exercise, particularly mechanical loading, is the most potent physiological stimulus for maintaining this balance in favor of formation.
Exercise prescription for post-menopausal osteoporosis is therefore not simply "advise walking" — it is a structured, individualized, multi-component, progressively overloaded therapeutic program that addresses bone density, muscle strength, neuromuscular balance, postural alignment, and functional independence simultaneously.
"Programs of regular exercise for general health can be recommended, especially those that increase muscle strength and improve balance, leading to fewer falls."
— Management of Osteoporosis in Postmenopausal Women: 2021 Position Statement (p. 9)
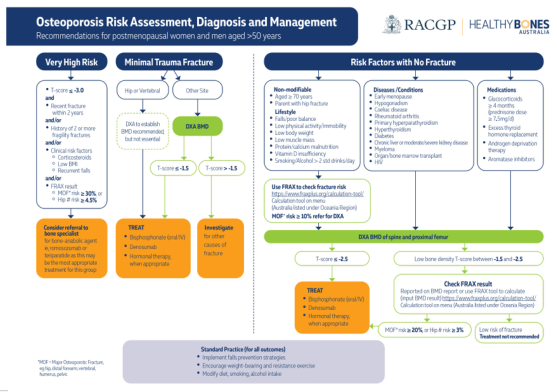
RISK STRATIFICATION BEFORE EXERCISE PRESCRIPTION
The type and intensity of exercise must be guided by the patient's risk profile. The following flowchart from clinical guidelines illustrates how osteoporosis severity determines the management pathway — including exercise intensity selection:
Clinical flowchart: Osteoporosis risk stratification in postmenopausal women — T-score thresholds, FRAX risk, fracture history, and fall risk all determine the appropriate exercise intensity and type. Standard practice (bottom) mandates weight-bearing and resistance exercise for all patients.
PRE-EXERCISE ASSESSMENT
A thorough assessment is mandatory before prescribing exercise:
| Assessment Domain | Tool / Method |
|---|
| Bone density | DEXA scan — T-score at femoral neck and lumbar spine |
| Fracture history | Vertebral, hip, wrist, rib fractures — type, site, recency |
| Fall risk screening | Timed Up and Go (TUG) test; Berg Balance Scale; 4-Stage Balance Test |
| Muscle strength | 30-second Chair Stand Test; Hand-grip dynamometry |
| Posture assessment | Kyphosis angle; forward head posture; lateral scoliosis |
| Cardiovascular fitness | 6-Minute Walk Test; resting HR and BP |
| Pain assessment | VAS/NRS score; location; aggravating/relieving factors |
| Comorbidities | Arthritis, cardiovascular disease, diabetes, neurological disorders |
| Medications | Bisphosphonates, corticosteroids, sedatives, antihypertensives (fall risk) |
| Functional limitations | ADL difficulty; fear of falling (Falls Efficacy Scale) |
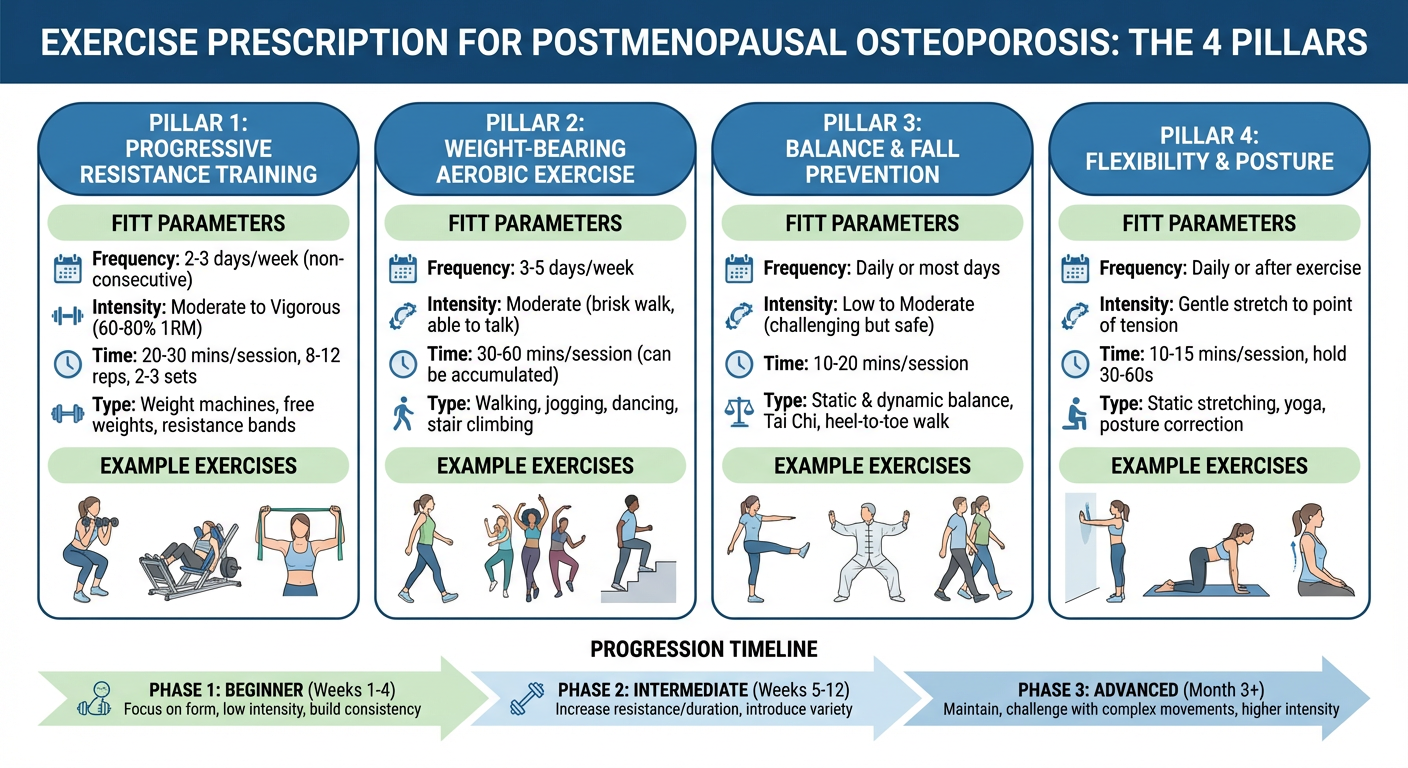
THE 4-PILLAR EXERCISE PRESCRIPTION MODEL
Exercise Prescription Diagram — 4 Pillars
The 4-pillar model of exercise prescription for postmenopausal osteoporosis: each pillar targets a specific domain of bone health, muscle function, fall prevention, and postural correction — prescribed according to FITT principles and progressed across 12 weeks.
▶ PILLAR 1: PROGRESSIVE RESISTANCE TRAINING (Primary Bone-Loading Stimulus)
Progressive resistance training (PRT) is the single most important exercise modality for postmenopausal osteoporosis. It directly loads the skeleton via muscle-tendon-bone force transmission and is the only modality proven to simultaneously increase BMD, muscle mass, and functional strength.
Principle of Progressive Overload (Guidelines, p. 76): "Resistance training may be prescribed using machines or free weights in which the loads (weights) are increased progressively over time. This is referred to as 'progressive overload', a critical training principle to elicit skeletal adaptations over time."
| Parameter | Recommendation |
|---|
| Frequency | 2–3 days/week on non-consecutive days (e.g., Mon/Wed/Fri) |
| Intensity | Begin 40–60% 1RM → progress to 70–85% 1RM over 8–12 weeks |
| Sets | 2–3 sets per exercise |
| Repetitions | 8–10 reps per set |
| Exercises/session | ~8 exercises targeting all major muscle groups |
| Rest intervals | 60–90 seconds between sets |
| Progression rule | Increase load 5–10% when patient completes all prescribed reps with perfect form |
Priority Muscle Groups and Exercises:
| Priority | Muscle Group | Exercise |
|---|
| ⭐⭐⭐ First Priority | Spinal extensors | Prone back extension, Superman, Bird-Dog, Seated row |
| ⭐⭐⭐ First Priority | Hip extensors/abductors | Hip bridge, Step-up, Clamshell, Side leg raise |
| ⭐⭐⭐ First Priority | Quadriceps | Sit-to-stand, Wall squat, Leg press |
| ⭐⭐ Second Priority | Upper back / Rhomboids | Band rows, Scapular retractions, Lat pulldown |
| ⭐⭐ Second Priority | Core stabilizers | Modified plank, Dead bug, Abdominal brace |
| ⭐ Third Priority | Shoulder / Chest | Chest press, Shoulder press, Wall push-up |
| ⭐ Third Priority | Calves / Ankle | Standing heel raises bilateral → unilateral |
▶ PILLAR 2: WEIGHT-BEARING AEROBIC EXERCISE (Skeletal Loading and Cardiovascular Health)
| Parameter | Recommendation |
|---|
| Frequency | Most days of week (5–7 days) (Guidelines, p. 76) |
| Intensity | Moderate-to-vigorous — RPE 5–7/10; 50–75% HRR |
| Duration | 30–60 min/day (accumulate in ≥10 min bouts) |
| Type | Brisk walking, stair climbing, dancing, low-impact aerobics, heel stomps |
Key evidence-based principle (Guidelines, p. 76): "Several short, more intense or higher-impact sessions are more beneficial to increase or maintain BMD than one longer, less-intense or low-impact session." Movements should be multidirectional to stimulate bone adaptation across multiple planes.
Impact-Based Activity Selection:
| Osteoporosis Severity | Appropriate Activity |
|---|
| T-score −1.0 to −2.5, no fracture | Jogging, jumping, step aerobics, dancing, stair climbing |
| T-score < −2.5, no fracture | Brisk walking, low-impact aerobics, Tai Chi, elliptical |
| Vertebral fracture present | Walking only; Tai Chi; NO jogging or jumping |
| Hip fracture, post-surgical | Aquatic walking initially; progress to land walking with clearance |
▶ PILLAR 3: BALANCE AND FALL PREVENTION TRAINING (Fracture Prevention via Fall Reduction)
Falls are the proximate cause of 90% of hip fractures in elderly osteoporotic women. Balance training directly addresses neuromuscular deficits — slower reaction time, reduced proprioception, impaired vestibular function — that accumulate after menopause.
| Parameter | Recommendation |
|---|
| Frequency | 2–3 days/week (integrated within or alongside resistance sessions) |
| Duration | 15–30 min per session |
| Type | Static balance, dynamic balance, Tai Chi, vestibular training, functional tasks |
Progressive Balance Training Protocol:
| Level | Exercise | Challenge Factor |
|---|
| Level 1 — Beginner | Two-leg standing near wall | Eyes open, firm surface, 30 sec |
| Level 2 | Tandem stance (heel-to-toe) | Eyes open → eyes closed |
| Level 3 | Semi-tandem stance / Single-leg stance | 10–30 sec holds; near wall |
| Level 4 | Single-leg stance with arm movements | Dual-task challenge |
| Level 5 — Advanced | Step-over obstacles; direction changes; balance board | Real-world fall trigger simulation |
Tai Chi deserves special emphasis: systematic reviews demonstrate Tai Chi reduces fall incidence by 47% in older adults. It combines slow controlled weight shifting, multi-directional movement, and mindful coordination — perfectly targeting the neuromotor deficits of postmenopausal women with osteoporosis.
▶ PILLAR 4: FLEXIBILITY AND POSTURE CORRECTION (Vertebral Protection and Kyphosis Management)
Thoracic kyphosis — the "dowager's hump" — results from multiple anterior vertebral compression fractures and progressively shifts the center of gravity forward, creating a vicious cycle of further falls and fractures. Posture correction exercises are therefore essential.
| Parameter | Recommendation |
|---|
| Frequency | Daily (5–7 days/week) |
| Duration | 10–15 min per session |
| Hold time | 20–30 sec per stretch, 2–3 reps |
Key Flexibility and Posture Exercises:
| Exercise | Technique | Benefit |
|---|
| Thoracic extension over foam roller | Horizontal foam roller under mid-back; gently extend over roller | Opens thoracic spine; directly counteracts kyphosis |
| Chest/Pectoral stretch | Arms extended at shoulder height in doorframe; gently lean forward | Stretches shortened anterior chest wall; opens posture |
| Hip flexor lunge stretch | Kneeling lunge position; gently push hips forward | Reduces anterior pelvic tilt; improves upright posture |
| Calf and Achilles stretch | Facing wall, heel flat; gentle lean forward | Ankle dorsiflexion; reduces fall risk |
| Upper trapezius stretch | Ear to shoulder gently; no force | Addresses forward head posture and neck tension |
| Thoracic rotation (seated) | Seated upright; rotate thorax ONLY — NOT lumbar spine | Maintains upper spinal mobility; control range carefully |
❌ STRICTLY AVOID all forward flexion stretches: seated toe-touch, yoga child's pose, Pilates roll-down, seated hamstring stretch with rounded back — these generate dangerous anterior compressive forces on osteoporotic vertebrae. (Secondary Fracture Prevention Guidelines, p. 8)
12-WEEK PROGRESSIVE EXERCISE PROGRAM
PHASE 1 — Weeks 1–4: Foundation (Learn Technique, Low Intensity)
| Component | Activity | Frequency | Duration |
|---|
| Resistance | Body weight + light resistance bands; 2 sets × 12 reps @ 40–50% 1RM | 2×/week | 30 min |
| Weight-bearing | Brisk walking on flat ground | 5×/week | 20–30 min |
| Balance | Two-leg standing; seated weight shifts; Tai Chi basics | 3×/week | 15 min |
| Flexibility | Thoracic extension, chest stretch, hip flexor stretch | Daily | 10 min |
Goal: Master correct technique; build baseline endurance; establish routine and confidence.
PHASE 2 — Weeks 5–8: Development (Moderate Intensity, Increase Load)
| Component | Activity | Frequency | Duration |
|---|
| Resistance | Light dumbbells + bands; 2–3 sets × 10 reps @ 60% 1RM | 3×/week | 40 min |
| Weight-bearing | Brisk walking + stair climbing + heel drops | 5–6×/week | 30–40 min |
| Balance | Tandem stance; single-leg stance near wall; step-overs | 3×/week | 20 min |
| Flexibility | Daily; add balance component; advance stretches | Daily | 10–15 min |
Goal: Increase load across all exercises; introduce stair climbing; challenge balance further.
PHASE 3 — Weeks 9–12: Consolidation (Moderate-High Intensity, Functional Progression)
| Component | Activity | Frequency | Duration |
|---|
| Resistance | Free weights + machines; 3 sets × 8–10 reps @ 70–80% 1RM | 3×/week | 45–50 min |
| Weight-bearing | Low-impact aerobics / dancing + walking | 5–7×/week | 40–60 min |
| Balance | Single-leg stance (no wall); balance board; full Tai Chi form | 3×/week | 25–30 min |
| Flexibility | Advanced thoracic mobility; foam roller daily | Daily | 15 min |
Goal: Achieve target training intensity; sustain across all four pillars; prepare for long-term independent maintenance.
SAMPLE MAINTENANCE WEEKLY SCHEDULE
| Day | Activity | Duration |
|---|
| Monday | Resistance Training — Lower Body (squats, hip bridge, leg press, heel raises) + Balance | 50 min |
| Tuesday | Brisk walking + Tai Chi | 45 min |
| Wednesday | Resistance Training — Upper Body + Back Extension (rows, chest press, shoulder press, prone cobra) | 45 min |
| Thursday | Low-impact aerobics / Dancing + Daily flexibility | 40 min |
| Friday | Resistance Training — Full Body Compound (sit-to-stand, step-ups, bird-dog, plank) + Balance | 50 min |
| Saturday | Stair climbing / Nordic walking + Posture stretches | 35 min |
| Sunday | Rest + Gentle thoracic extension + Deep breathing | 15 min |
MODIFICATIONS FOR SPECIAL CLINICAL SITUATIONS
| Clinical Situation | Modified Exercise Approach |
|---|
| Vertebral fracture present | No loaded spinal flexion; back extension exercises priority; seated resistance preferred; walking over jogging |
| Hip fracture (post-surgical) | Hip precautions (no flexion >90°); begin aquatic; progress to standing with surgical clearance |
| Severe kyphosis (>40°) | All exercise in extension-neutral or extension-biased position; thoracic extensor strengthening priority |
| T-score < −3.5 (very severe) | Low-impact only; supervised physiotherapy essential; chair-based resistance; NO impact loading |
| Osteoarthritis comorbidity | Seated resistance preferred; aquatic therapy for painful flares; reduce weight-bearing aerobics intensity |
| Frailty | Chair-based exercises; 10–15 min sessions; 3×/week; gradual progression only |
| Cognitive impairment | Simplified routines; supervised group program; visual demonstrations; consistent structure |
| Post-THR | Strict hip precautions: no flexion >90°, no internal rotation, no adduction past midline (Guidelines, p. 79) |
EXERCISE AND PHARMACOTHERAPY — COMPLEMENTARY ROLES
Exercise does not replace pharmacotherapy in confirmed osteoporosis. It is prescribed alongside:
| Drug Class | Example | Mechanism |
|---|
| Bisphosphonates | Alendronate, Zoledronate | Suppress osteoclast activity; reduce bone resorption |
| Denosumab | Prolia | Anti-RANKL antibody; potent resorption inhibitor |
| Anabolic agents | Teriparatide, Romosozumab | Stimulate osteoblastic new bone formation |
| HRT | Estradiol ± progestogen | Restores estrogen; reduces remodeling imbalance |
Nutrition prerequisites: Without adequate Calcium (1000–1200 mg/day) and Vitamin D (800–1000 IU/day), the osteogenic stimulus from exercise cannot be mineralized into functional new bone — nutritional optimization is mandatory alongside the exercise program.
EXPECTED OUTCOMES WITH CONSISTENT ADHERENCE
| Timeframe | Expected Benefits |
|---|
| 4–8 weeks | Improved muscle strength; reduced back pain; better postural awareness |
| 3–6 months | Measurable improvement in balance; reduced fall frequency; improved functional scores |
| 6–12 months | Stabilization or modest 1–3% increase in BMD at spine/hip on repeat DEXA |
| 1–2 years | Significant reduction in fall-related fractures; maintained mobility and independence |
| Long-term | Preserved BMD; sustained quality of life; reduced healthcare burden |
SUMMARY TABLE — Complete Exercise Prescription at a Glance
| Pillar | Type | Frequency | Intensity | Duration |
|---|
| 1. Progressive Resistance | Weights, bands, machines | 2–3×/week | 70–85% 1RM | 40–50 min |
| 2. Weight-Bearing Aerobic | Walking, dancing, aerobics | 5–7×/week | Moderate–vigorous (RPE 5–7) | 30–60 min |
| 3. Balance Training | Tai Chi, static/dynamic drills | 2–3×/week | Progressively challenging | 15–30 min |
| 4. Flexibility/Posture | Thoracic extension, stretching | Daily | Gentle (no pain) | 10–15 min |
CONCLUSION
The exercise prescription for postmenopausal women with osteoporosis is a multi-component, individualized, and progressively overloaded therapeutic intervention built on four pillars. Progressive resistance training provides the primary osteogenic mechanical stimulus; weight-bearing aerobic exercise delivers sustained skeletal loading and cardiovascular benefit; balance training directly prevents the falls that cause fractures; and flexibility and posture work protect the vertebral column from progressive kyphotic collapse. When combined with pharmacotherapy, adequate nutrition, fall-hazard reduction, and professional supervision, this exercise prescription substantially reduces fracture risk, preserves functional independence, and improves quality of life in postmenopausal women with osteoporosis.
"Exercise programs should be individualised to a person's needs, abilities and interests. People with osteoporosis should be encouraged to 'do more' and not 'less' in terms of exercise."
— Osteoporosis Management and Fracture Prevention Guidelines (p. 79)
References:
- Osteoporosis Management and Fracture Prevention in Postmenopausal Women and Men Over 50 Years of Age, pp. 76, 79
- Management of Osteoporosis in Postmenopausal Women: 2021 Position Statement, p. 9
- Secondary Fracture Prevention Guidelines, p. 8
- Harrison's Principles of Internal Medicine, 21st Edition, p. 11631