Cavernous anatomy detailed explanation and in simple way with all images
Reading File
Asking for Preferences
Finding Sources
Searching the Web
cavernous sinus anatomy detailed explanation structures relations
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I have excellent images and comprehensive content. Now I have everything I need to write a thorough, well-illustrated explanation of cavernous sinus anatomy. Let me compose the full answer.
Cavernous Sinus Anatomy - Detailed & Simple Explanation
What Is the Cavernous Sinus?
Think of the cavernous sinus as a spongy blood-filled cave on each side of the skull base. It is a dural venous sinus - meaning it is a large channel formed between two layers of the dura mater (the tough outer covering of the brain). It sits on either side of the sella turcica (the "Turkish saddle" bone housing the pituitary gland) and the body of the sphenoid bone.
Simple analogy: Imagine a sponge soaked in blood, tucked just beside the pituitary gland, with several important nerves and arteries running through or along its walls.
Location & Shape
- Position: Lateral to the sella turcica and pituitary gland, one on each side
- Extent: From the apex of the orbit anteriorly to the apex of the petrous temporal bone posteriorly
- Size: Roughly 2 cm long and 1 cm wide
- Formed by: A fold of the inner layer of dura mater, whose medial wall is continuous with the diaphragma sellae (the dural roof over the pituitary)
Coronal Section - The Most Important View
This diagram shows both cavernous sinuses in coronal section - this is the single most important view for understanding anatomy:
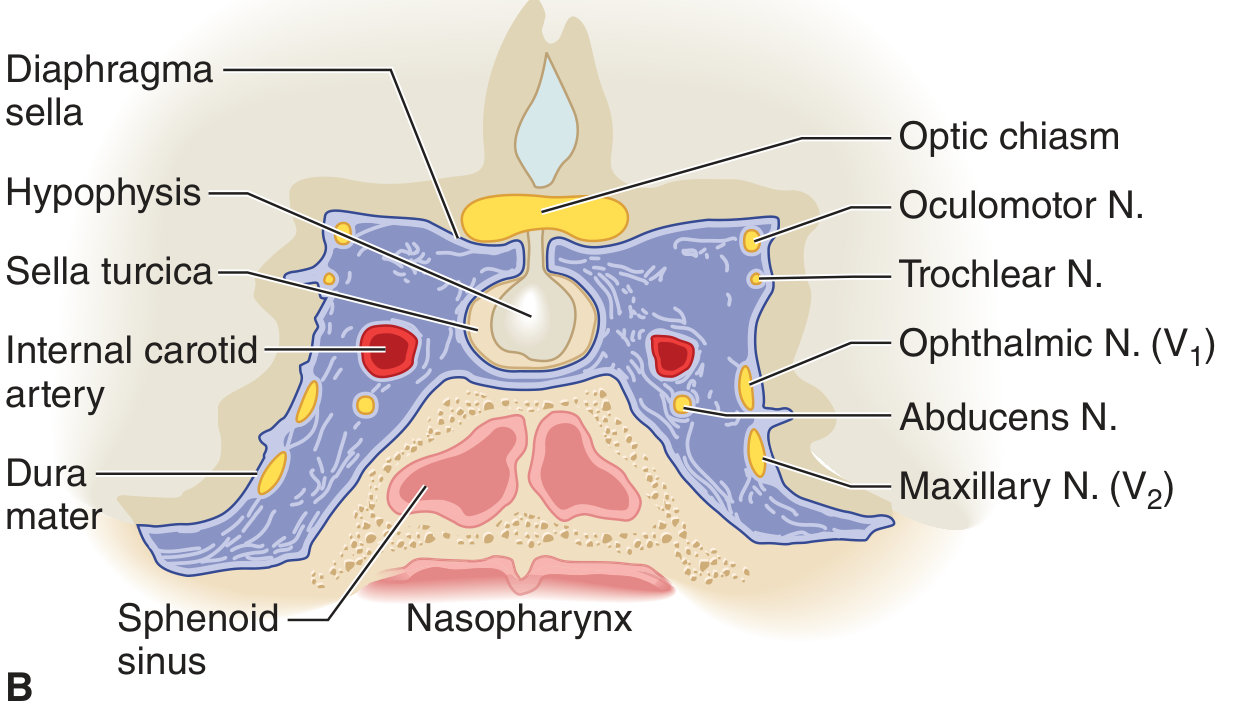
Coronal view: Both cavernous sinuses (blue) flanking the pituitary. CN III (red), CN IV (blue dot), CN V1 (green), CN V2 (orange), CN VI (light blue) are color-coded. ICA sits inside the sinus (large red circle). Sphenoid sinuses (SS) lie below.
What Is Inside the Cavernous Sinus?
The sinus contains two main structures running through its substance:
| Structure | Position | Notes |
|---|---|---|
| Internal Carotid Artery (ICA) | Passes through the sinus | The only artery in a venous sinus - unique! |
| Abducent Nerve (CN VI) | Travels freely inside the sinus | Most vulnerable nerve - no dural protection |
What Is in the Lateral Wall?
Four nerves are embedded within the lateral wall of the cavernous sinus (from top to bottom):
| Order | Nerve | Function |
|---|---|---|
| 1st (most superior) | CN III - Oculomotor | Moves eye up/down/in, pupil constriction |
| 2nd | CN IV - Trochlear | Moves eye down and inward |
| 3rd | CN V1 - Ophthalmic (branch of trigeminal) | Sensation from eye, forehead |
| 4th (most inferior) | CN V2 - Maxillary (branch of trigeminal) | Sensation from cheek, upper teeth |
Key memory trick: "O TOM CAT" or simply top to bottom: III, IV, V1, V2 in the wall; VI and ICA inside.
Lateral View - Contents Exposed
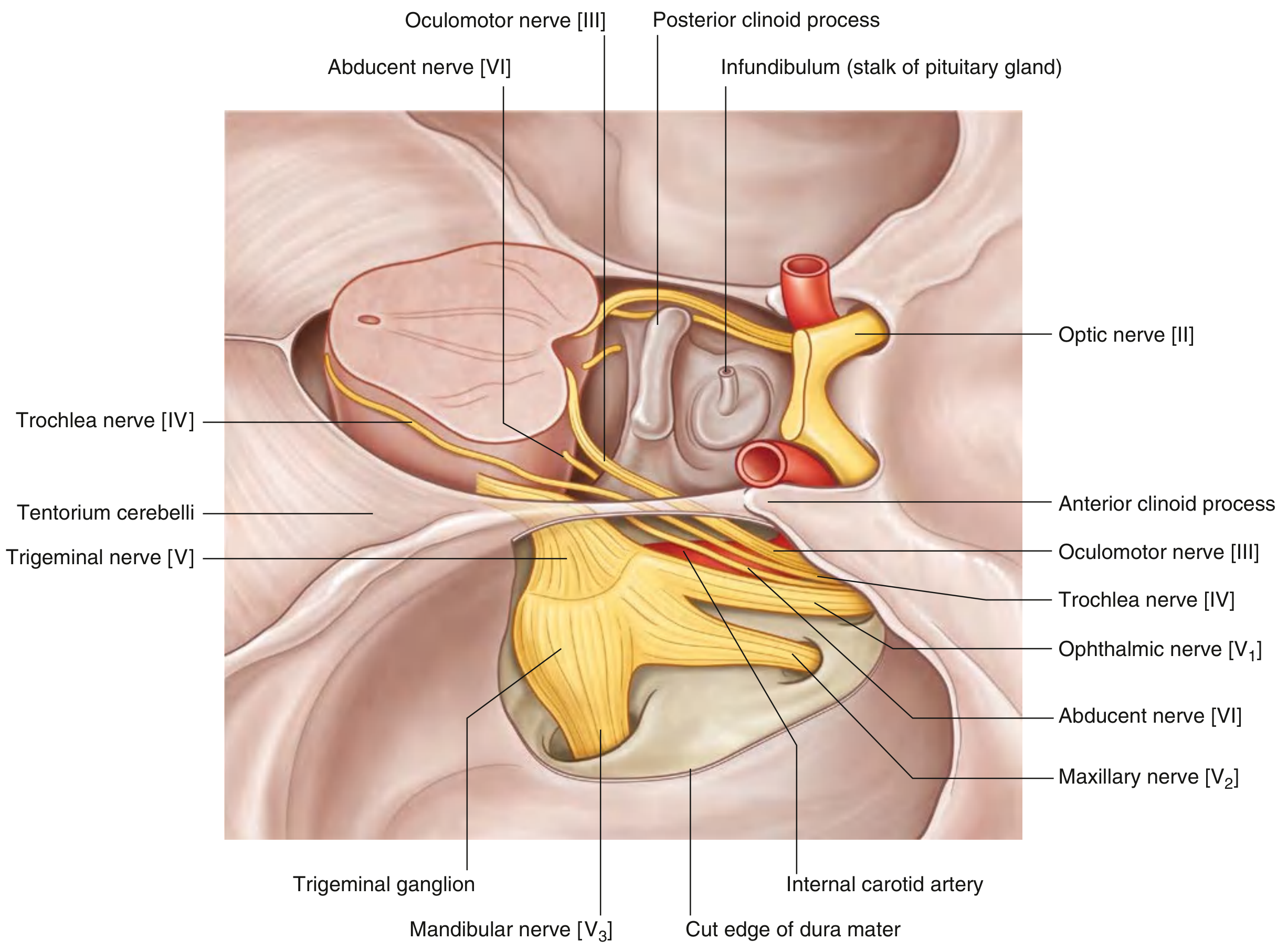
Lateral view with meningeal dura removed: The trigeminal ganglion (Gasserian ganglion) sits posterolateral to the sinus in Meckel's cave. All three cranial nerve divisions (V1, V2, V3) are visible. CN III, IV, V1, V2 run in the lateral wall; CN VI and ICA pass through the sinus itself.
Relations - What Borders the Cavernous Sinus?
| Wall | What is it adjacent to? |
|---|---|
| Medial wall | Pituitary gland (hypophysis) and sella turcica |
| Superior wall | Optic chiasm, diaphragma sellae |
| Inferior wall | Body and greater wing of sphenoid bone; sphenoid sinus below |
| Anterior end | Superior orbital fissure and apex of orbit |
| Posterior end | Petrous apex; near Meckel's cave (trigeminal ganglion) |
| Lateral wall | Contains CN III, IV, V1, V2 (embedded in dura) |
Color-Coded Diagram
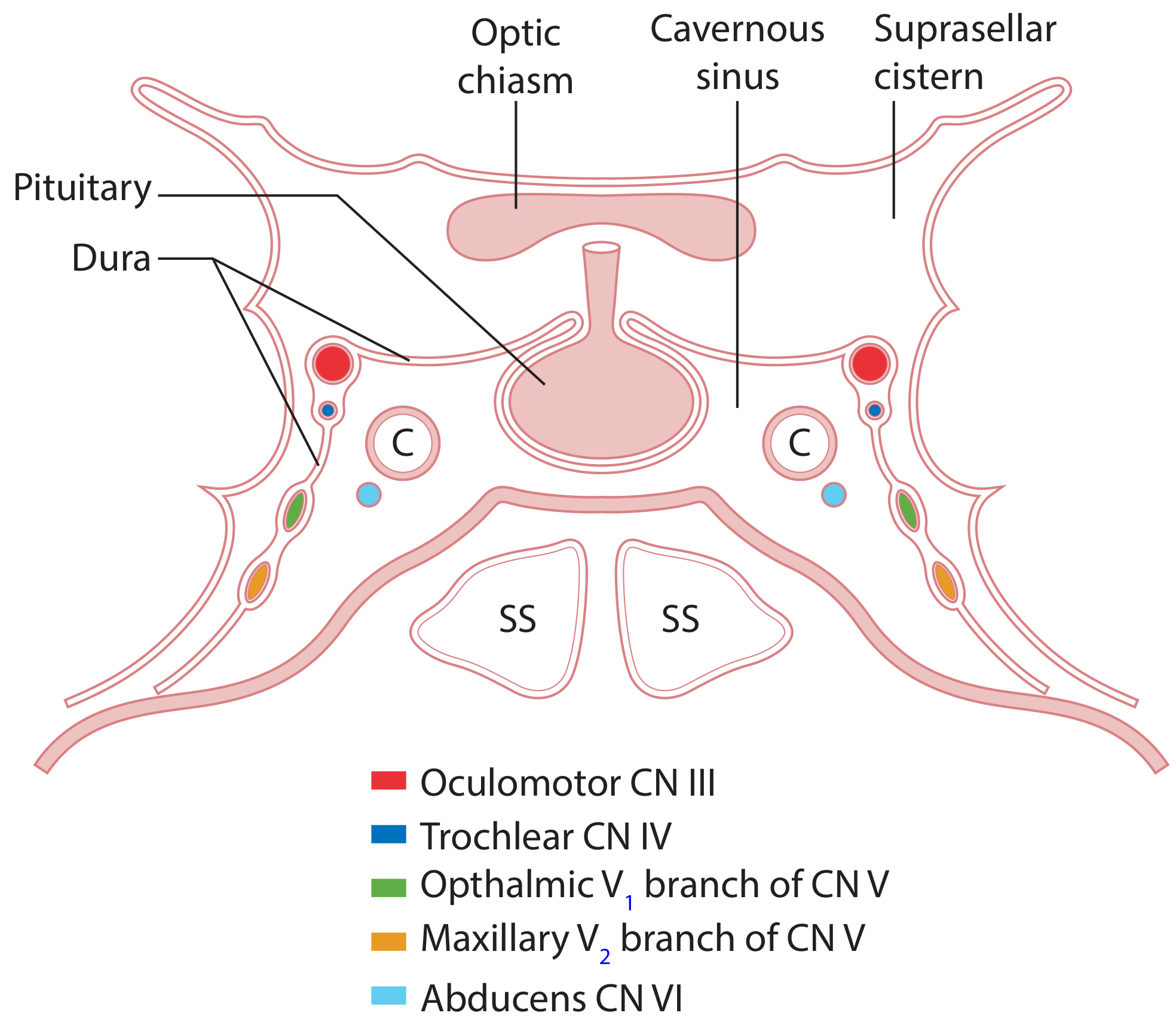
Color legend: Red = CN III; Blue = CN IV; Green = CN V1; Orange = CN V2; Light blue = CN VI. "C" labels = ICA cross-section. "SS" = Sphenoid sinuses.
Blood Supply and Drainage
What flows INTO the cavernous sinus?
The sinus collects blood from multiple sources - this is why infections can spread here so easily:
- Superior and inferior ophthalmic veins from the orbit (direct connections to the face)
- Sphenoparietal sinus (from the meningeal and diploic veins)
- Cerebral veins (from the brain surface)
- Pterygoid plexus via a communicating vein through the foramen ovale - this allows facial infections to spread intracranially!
- Angular vein / facial vein via the superior ophthalmic vein
What flows OUT of the cavernous sinus?
| Drainage Pathway | Destination |
|---|---|
| Superior petrosal sinus | → Transverse sinus |
| Inferior petrosal sinus | → Internal jugular vein |
| Intercavernous sinuses | → Connects left and right cavernous sinuses (anterior and posterior to pituitary stalk) |
| Basilar plexus | → Vertebral venous plexus |
Arteries of the Skull Base Near the Cavernous Sinus
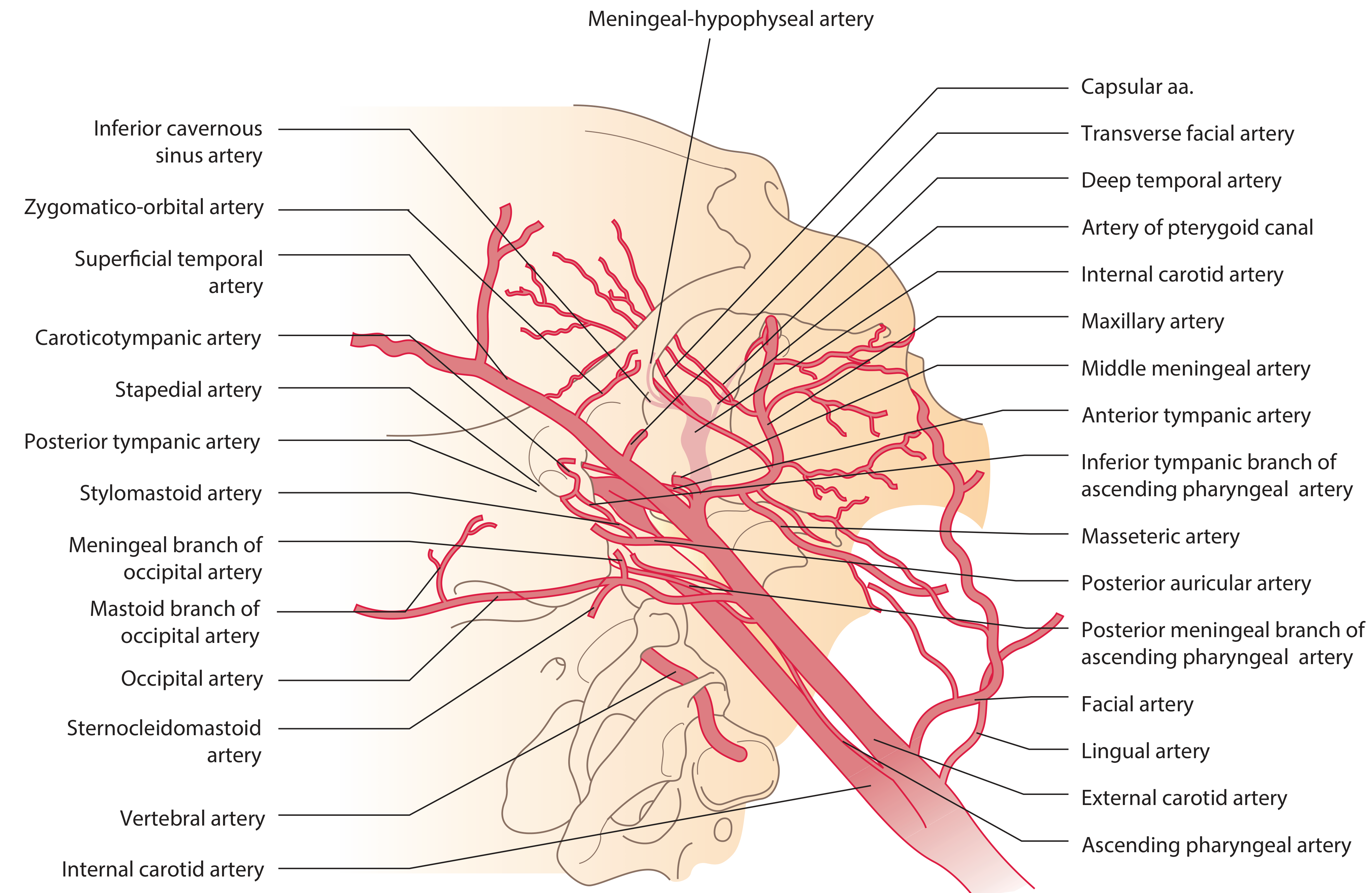
The ICA gives off the meningeal-hypophyseal artery (supplies dura, pituitary stalk, brainstem) and the inferior cavernous sinus artery while passing through the cavernous sinus.
The ICA's Course Through the Sinus - "Cavernous Siphon"
The internal carotid artery takes a characteristic S-shaped bend inside the cavernous sinus:
- Enters from below through the foramen lacerum (petrous apex)
- Turns upward, then forward, then medially
- Exits superiorly just posterior to the optic canals, piercing the dura to enter the middle cranial fossa
- Immediately divides into its terminal branches (anterior and middle cerebral arteries)
This looping segment is called the cavernous siphon and is visible on angiography. Aneurysms here are called cavernous ICA aneurysms.
Embryology (Simple)
The cavernous sinus is derived from the primary head vein during fetal development. It is not a true endothelium-lined vessel but a trabeculated venous channel enclosed within dural folds. - Scott-Brown's Otorhinolaryngology, Vol. 1
Why Is This Anatomy Clinically Important?
The cavernous sinus is one of the most clinically significant anatomical regions because:
1. Cavernous Sinus Thrombosis
Infection (e.g., from a facial boil, sinusitis) can travel via the facial vein → ophthalmic veins → cavernous sinus. This produces:
- Proptosis (eye bulging)
- Chemosis (conjunctival swelling)
- Painful ophthalmoplegia (multiple cranial nerve palsies III, IV, VI)
- Periorbital edema
2. Carotid-Cavernous Fistula (CCF)
Abnormal connection between the ICA and the cavernous sinus (trauma or aneurysm rupture). Presents with pulsatile exophthalmos and bruit over the eye.
3. Pituitary Tumor Invasion
A pituitary adenoma expanding laterally invades the cavernous sinus - the oculomotor nerve (CN III) is most frequently compressed first. Patients develop ptosis and ophthalmoplegia.
4. Cavernous Sinus Syndrome
Any lesion here (tumor, aneurysm, granuloma) causes ipsilateral involvement of CN III + IV + V1 + V2 + VI. CN VI palsy (abducens) is especially sensitive because it has NO dural protection.
5. Tolosa-Hunt Syndrome
Idiopathic granulomatous inflammation of the cavernous sinus causing painful ophthalmoplegia, treated with corticosteroids.
Quick Summary Table
| Feature | Detail |
|---|---|
| Type | Paired dural venous sinus |
| Location | Lateral to sella turcica, on sphenoid bone |
| Contents (inside) | ICA + CN VI |
| Lateral wall (top to bottom) | CN III → CN IV → CN V1 → CN V2 |
| Posterolateral | Trigeminal ganglion in Meckel's cave |
| Drains to | Superior and inferior petrosal sinuses |
| Receives from | Ophthalmic veins, sphenoparietal sinus, pterygoid plexus |
| Connects both sides via | Intercavernous sinuses |
| ICA branch inside | Meningeal-hypophyseal artery |
Sources:
- Gray's Anatomy for Students, Figs. 8.47 and 8.48
- Adams and Victor's Principles of Neurology, 12th Ed., Fig. 13-5
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1 & 2
- Color Atlas of Human Anatomy, Vol. 2 - Internal Organs
This is a shared conversation. Sign in to Orris to start your own chat.