is microfillare of wucheria bancroftei a larve
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Great - here is a thorough answer based on authoritative medical microbiology textbooks.
Are Microfilariae of Wuchereria bancrofti Larvae?
Short answer: Microfilariae are NOT true larvae. They are pre-larval embryos (sometimes called "pre-larvae" or the first embryonic stage).
Here is the breakdown:
What Are Microfilariae?
Microfilariae are the embryonated offspring produced by adult female W. bancrofti worms. The process works like this:
- The gravid female produces large numbers of embryonated eggs
- At oviposition (egg laying), the embryo uncoils to its full length (200-300 µm) inside the egg shell
- The egg shell elongates and is retained as a thin, flexible sheath
- This sheathed embryo is what we call a microfilaria ("small thread")
So a microfilaria is essentially an embryo inside a stretched egg shell (sheath) - not a true larva.
(Sherris & Ryan's Medical Microbiology, 8th Edition)
The Distinction: Embryo vs. Larva
| Feature | Microfilaria | True Larva |
|---|---|---|
| Stage | Pre-larval embryo | Post-embryonic developmental stage |
| Location | Peripheral blood (human host) | Mosquito (intermediate host) |
| Development | Not yet undergone larval molts | Has undergone ≥1 molt |
| Infective? | No - cannot directly infect humans | L3 stage is infective |
Life Cycle Context
The microfilariae circulate in the human bloodstream. To become true larvae, they must be taken up by a mosquito (the intermediate host/vector). Inside the mosquito:
- L1 larva - microfilaria develops after being ingested by mosquito
- L2 larva - first molt inside mosquito flight muscles
- L3 larva (infective stage) - migrates to mosquito's proboscis; this is the true infective larva that enters a new human host during a blood meal
So the progression is:
Embryo (egg) → Microfilaria (pre-larva in blood) → L1 → L2 → L3 (infective larva in mosquito)
Characteristics of W. bancrofti Microfilariae
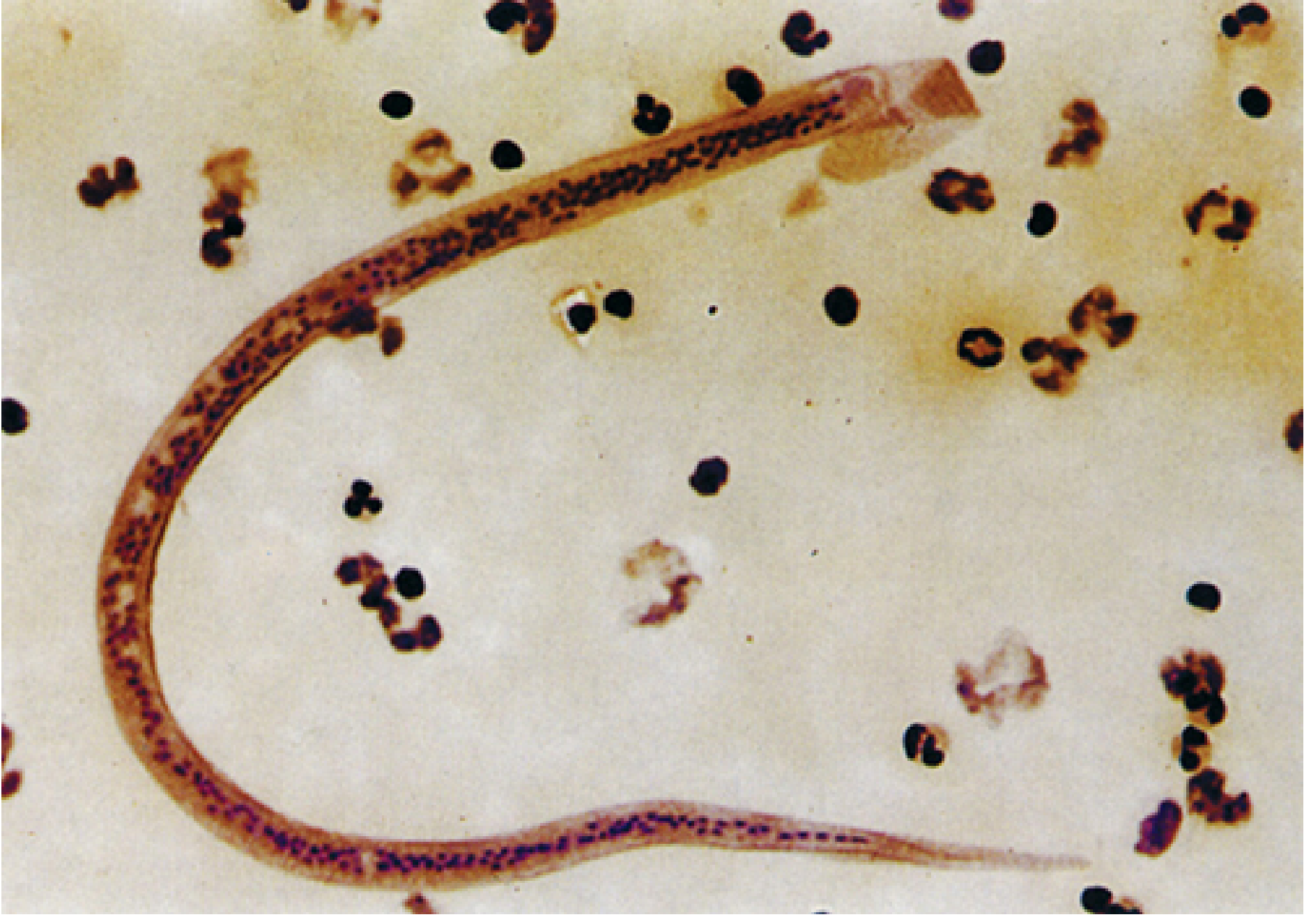
Microfilaria of W. bancrofti in blood film - Sherris & Ryan's Medical Microbiology, 8th Ed.
| Feature | Detail |
|---|---|
| Size | 245-295 µm long × 7-10 µm wide (in blood smear) |
| Sheath | Present (key distinguishing feature) |
| Tail nuclei | Absent - nuclei do NOT reach the tail tip |
| Periodicity | Nocturnal (peak in peripheral blood: 9 PM - 2 AM) |
| Location in human | Peripheral blood (and pulmonary vessels during daytime) |
(Medical Microbiology 9e; Sherris & Ryan's Medical Microbiology 8e)
Why the Confusion?
Some older texts loosely call microfilariae "larvae" or "first-stage larvae (L1)" because they are the first mobile offspring. However, strictly speaking:
- Microfilariae are pre-larval - they have not yet undergone any larval molt
- The true L1 stage only begins inside the mosquito after the microfilaria is ingested
- The term "larva" is more correctly reserved for post-embryonic, post-molt stages in the mosquito
Summary: Microfilariae of W. bancrofti are embryos (pre-larvae) circulating in human blood inside a sheath (stretched egg shell). They become true larvae only after being ingested by a mosquito, going through L1 → L2 → L3 stages. The L3 is the infective larval stage transmitted back to humans.
wucheria bancrofti complete microbiology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Here is the complete microbiology of Wuchereria bancrofti, compiled from multiple authoritative medical textbooks.
Wuchereria bancrofti - Complete Microbiology
1. Classification
| Feature | Detail |
|---|---|
| Kingdom | Animalia |
| Phylum | Nematoda (roundworms) |
| Superfamily | Filarioidea ("thread-like") |
| Class | Tissue nematode |
| Disease caused | Lymphatic filariasis (Bancroftian filariasis) |
2. Morphology
Adult Worms
- Long, slender, thread-like white worms coiled in lymphatic vessels
- Female: ~100 mm (10 cm) long
- Male: ~40 mm long
- Adults live coiled together in lymphatic vessels for up to 10 years
- Both sexes harbor endosymbiotic Wolbachia bacteria in their gut, which are required for normal reproduction and metabolism
Microfilariae
The gravid female produces large numbers of embryonated eggs. At oviposition, the embryo uncoils inside the elongating egg shell (retained as a thin flexible sheath) to become a microfilaria.

| Feature | W. bancrofti | B. malayi (for comparison) |
|---|---|---|
| Location | Blood | Blood |
| Sheath | Present | Present |
| Size | 245-295 µm × 7-10 µm | 180-230 µm × 5-6 µm |
| Tail nuclei | Absent (nuclei do NOT reach tip) | Present (2 distinct nuclei at tip) |
| Sheath staining (Giemsa) | Does not stain pink | Stains bright pink |
| Periodicity | Usually nocturnal | Nocturnal/subperiodic |
3. Life Cycle
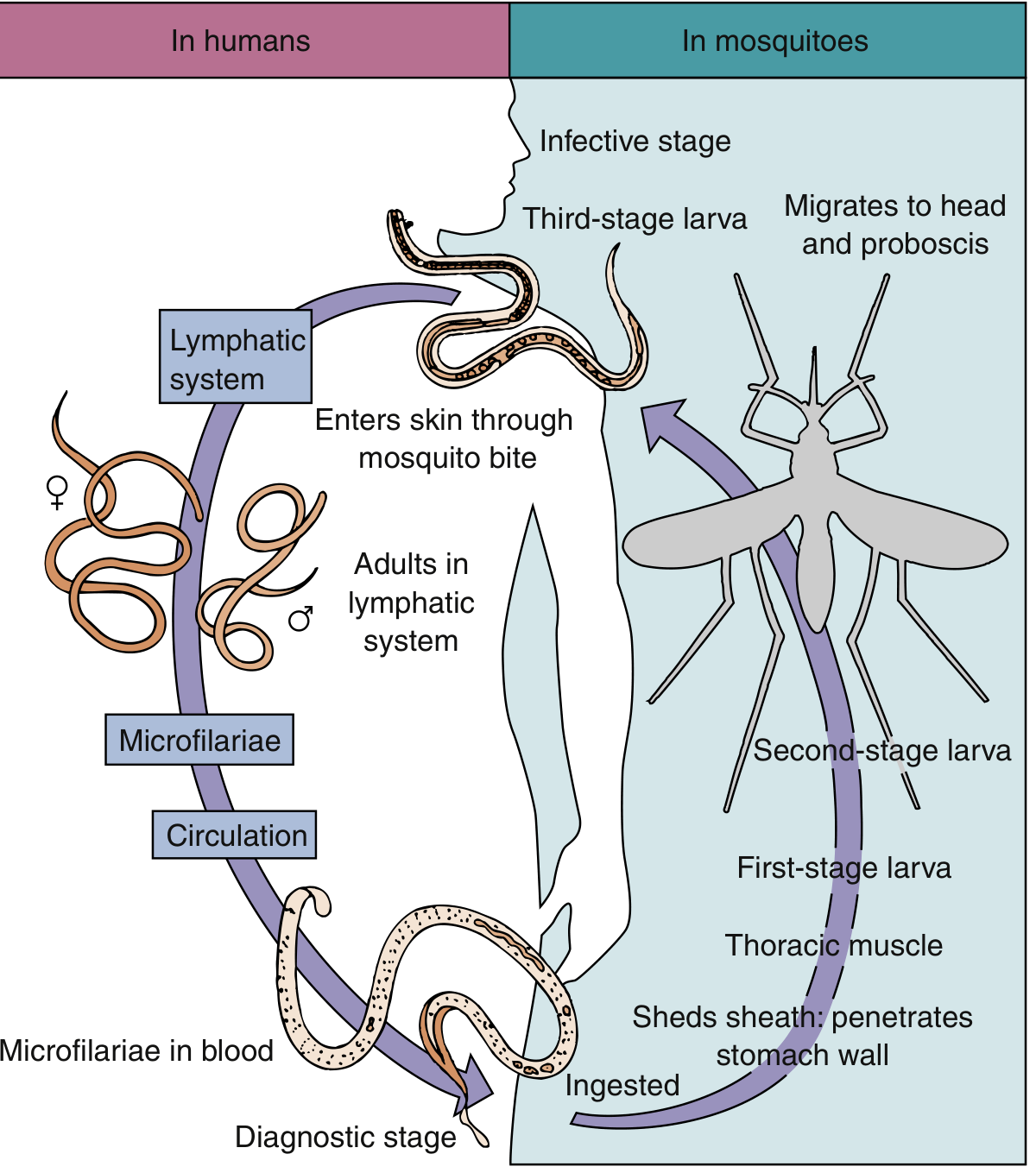
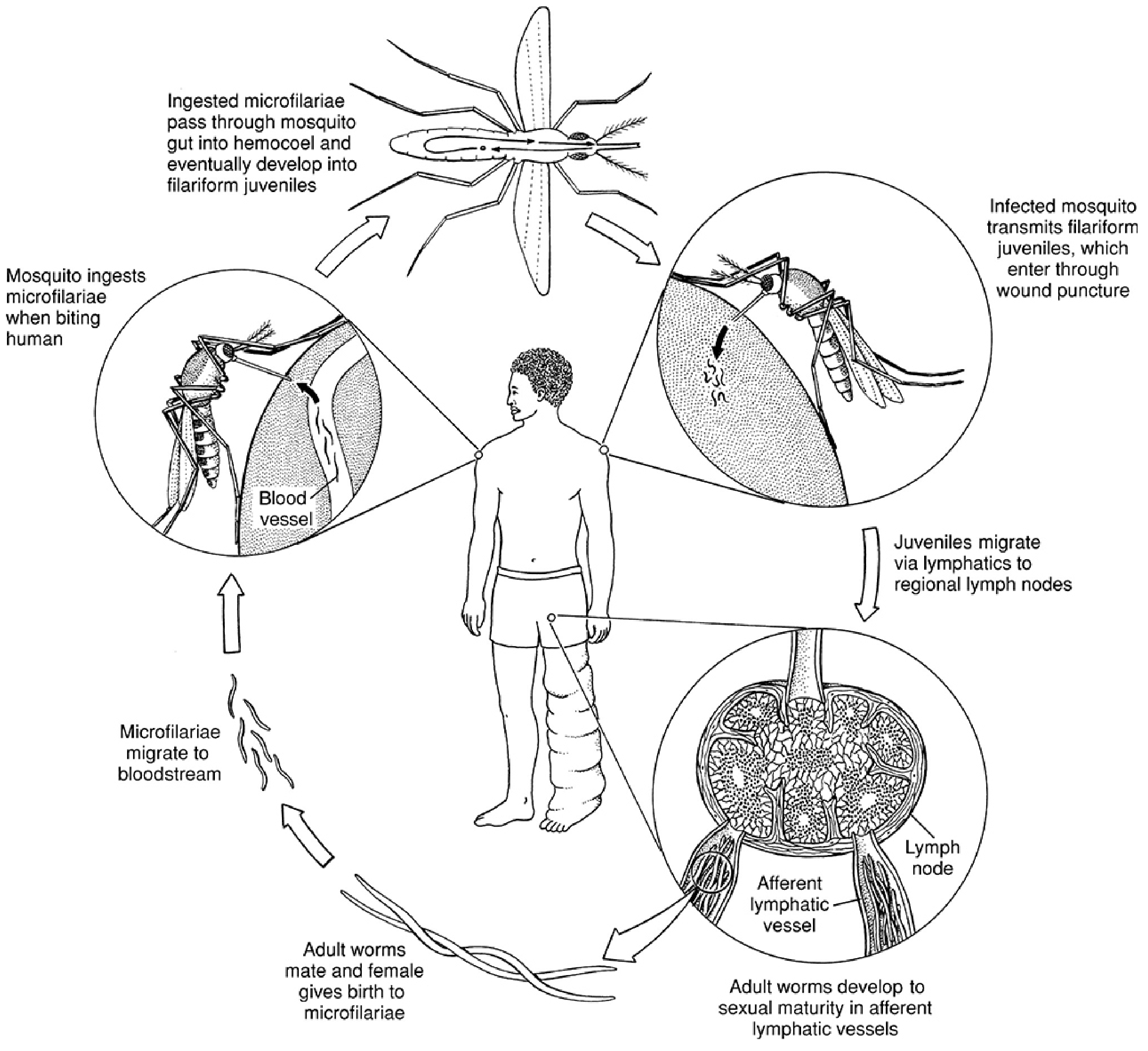
In the Human Host
- Infected mosquito bites → deposits L3 (infective) larvae into the skin wound
- L3 larvae migrate to the lymphatic vessels (arms, legs, groin)
- Larvae undergo molts and mature into adult worms over 6-12 months
- Adults mate; gravid females produce microfilariae → microfilariae enter lymph → reach peripheral blood
- Adults persist for up to 10 years
In the Mosquito (Intermediate Host/Vector)
- Mosquito ingests microfilariae during a blood meal
- Microfilariae shed their sheath and penetrate the mosquito stomach wall
- Develop in thoracic flight muscles: microfilaria → L1 (rhabditiform) → L2 → L3 (filariform/infective)
- L3 larvae migrate to the proboscis (mouthparts)
- Transmitted to a new human host during the next blood meal
Vector Mosquitoes
- W. bancrofti: transmitted by Culex, Anopheles, and Aedes mosquitoes
- No animal reservoir for W. bancrofti (humans are the only definitive host)
4. Epidemiology
- Infects approximately 120 million people in 73 countries
- Endemic in: central Africa, Mediterranean coast, Asia (India, China, Korea, Japan, Philippines, Malaysia), parts of Caribbean and South America (Haiti, Brazil, Trinidad)
- Concentrated in poorly sanitized, densely crowded urban and tropical/subtropical areas
- B. malayi (related species) has animal reservoirs (cats, monkeys); W. bancrofti does not
5. Pathology and Pathogenesis
Mechanism
Adult worms in lymphatic vessels are the primary cause of inflammatory and fibrotic reactions. Two phases:
Acute Phase
- Presence of molting adolescent worms and dying adults triggers:
- Dilatation of lymphatics
- Hyperplastic endothelial changes
- Lymphatic infiltration by lymphocytes, plasma cells, and eosinophils
- Thrombus formation (acute lymphangitis)
- Granuloma formation and fibrosis follow
- Recurring acute episodes of fever, lymphadenitis, lymphangitis, chills
Chronic Phase
- Repeated infections → permanent lymphatic obstruction
- Lymphedema, ascites, pleural effusion, hydrocele, joint effusion
- Elephantiasis: grotesque enlargement of extremities, scrotum, breasts from massive lymphatic blockade + skin thickening/fibrosis
- Dilated lymphatics may rupture → abscess, draining sinuses, chyluria (lymph in urine)
- Bacterial and fungal superinfections worsen tissue damage
Tropical Pulmonary Eosinophilia (TPE)
- Rare syndrome (< 1% of infected)
- Immune hyperresponsiveness to microfilariae trapped in the lungs
- Features: nocturnal paroxysmal cough/wheezing, weight loss, low-grade fever, marked blood eosinophilia (≥3000/µL), elevated IgE
- More common in young adult males
- Microfilariae usually absent from blood in TPE
- Responds rapidly to DEC
6. Clinical Syndromes
| Presentation | Features |
|---|---|
| Asymptomatic microfilaremia | Microfilariae present, no symptoms |
| Acute adenolymphangitis | Fever, tender lymph nodes, lymphangitis (centrifugally spreading down limbs) |
| Filarial fever | Low-grade fever, recurs over weeks/months |
| Orchitis / epididymitis | Bancroftian filariasis specifically involves testicular, spermatic cord lymphatics |
| Hydrocele | Common chronic manifestation |
| Elephantiasis | Massive limb, genital, breast enlargement (irreversible) |
| Chyluria | Lymph in urine (milky urine) from ruptured lymphatics |
| Tropical Pulmonary Eosinophilia | Nocturnal cough, wheeze, marked eosinophilia |
7. Laboratory Diagnosis
Direct Detection
| Method | Details |
|---|---|
| Peripheral blood film (Giemsa) | Gold standard - detects sheathed microfilariae; blood collected at night (10 PM - 2 AM) for nocturnal periodicity strains |
| Buffy coat examination | Concentrates microfilariae for better detection |
| Membrane filtration technique | Anticoagulated blood filtered through 5-µm membrane; washed, stained - detects small numbers |
| Thick blood film | More sensitive than thin film |
Indirect / Molecular
| Method | Details |
|---|---|
| Circulating antigen detection | ICT cards (immunochromatographic test) - sensitivity 96-100%, specificity ~98%; can be done any time of day; not FDA-approved in USA |
| Serology (antifilarial antibodies) | Available at reference labs; not species-specific |
| NAAT / PCR | Most sensitive; detects parasite DNA; no commercial platform yet |
| Eosinophilia | Usually present in acute episodes |
| Ultrasound | "Filarial dance sign" - live adult worms seen moving in dilated lymphatics |
Species Differentiation of Microfilariae
- W. bancrofti: sheathed, tail nuclei absent, sheath does not stain pink with Giemsa
- B. malayi: sheathed, 2 distinct nuclei in tail, sheath stains bright pink with Giemsa
8. Treatment
Drug of Choice
Diethylcarbamazine (DEC) - 6 mg/kg/day
- Mechanism: stimulates cholinergic receptors → muscle depolarization → worm paralysis; also enhances leukocyte adherence to microfilariae
- Kills microfilariae primarily; also has activity against adult worms
- Caution: Destruction of microfilariae releases Wolbachia antigens → inflammatory reaction (Mazzotti-like reaction); always screen for co-infection with Loa loa (risk of encephalopathy) and Onchocerca volvulus before starting DEC
Alternative/Adjunct Drugs
| Drug | Role |
|---|---|
| Ivermectin | Single dose reduces microfilariae for up to 6 months; fewer side effects than DEC |
| Albendazole | Used in combination for mass drug administration programs |
| DEC + Albendazole or DEC + Ivermectin | Used in WHO global elimination programs |
| Doxycycline | Targets Wolbachia endosymbionts → sterilizes/kills adult worms over weeks; used as adjunct |
Mass Drug Administration (MDA)
WHO Global Programme to Eliminate Lymphatic Filariasis (GPELF) uses annual MDA with DEC + albendazole (or ivermectin + albendazole in onchocerciasis co-endemic areas) to interrupt transmission.
9. Prevention and Control
- Vector control: insecticide spraying, larval source reduction (Culex breeding sites)
- Personal protection: mosquito nets, repellents, protective clothing
- Mass drug administration (MDA): annual single-dose treatment of entire at-risk populations
- No animal reservoir for W. bancrofti - human-to-mosquito-to-human transmission only
10. Key Distinguishing Facts (High-Yield Summary)
| Point | Detail |
|---|---|
| Causative agent of | Bancroftian filariasis (lymphatic filariasis) |
| Adult worm habitat | Lymphatic vessels |
| Adult worm lifespan | Up to 10 years |
| Diagnostic stage | Microfilariae in blood |
| Microfilaria features | Sheathed, no tail nuclei, 245-295 µm |
| Infective stage | L3 larva (in mosquito proboscis) |
| Vector | Culex, Anopheles, Aedes mosquitoes |
| Periodicity | Nocturnal (blood collected at night) |
| Animal reservoir | None (humans only) |
| Endosymbiont | Wolbachia bacteria |
| Drug of choice | DEC (diethylcarbamazine) |
| Classic chronic sign | Elephantiasis |
| Pulmonary complication | Tropical Pulmonary Eosinophilia |
Sources: Sherris & Ryan's Medical Microbiology 8e; Medical Microbiology 9e (Murray); Jawetz, Melnick & Adelberg's Medical Microbiology 28e; Katzung's Basic & Clinical Pharmacology 16e; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.