Bro diabetes type 2 k treatment protocol patient age 50 year
Reading File
Finding Sources
Searching PubMed
"type 2 diabetes"[MeSH Terms] AND "management"[MeSH Terms]
Finding Sources
Searching PubMed
"type 2 diabetes" AND "treatment guidelines"
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a comprehensive answer. Here is the full Type 2 Diabetes treatment protocol for a 50-year-old patient:
Type 2 Diabetes Mellitus - Treatment Protocol (Patient Age: 50 Years)
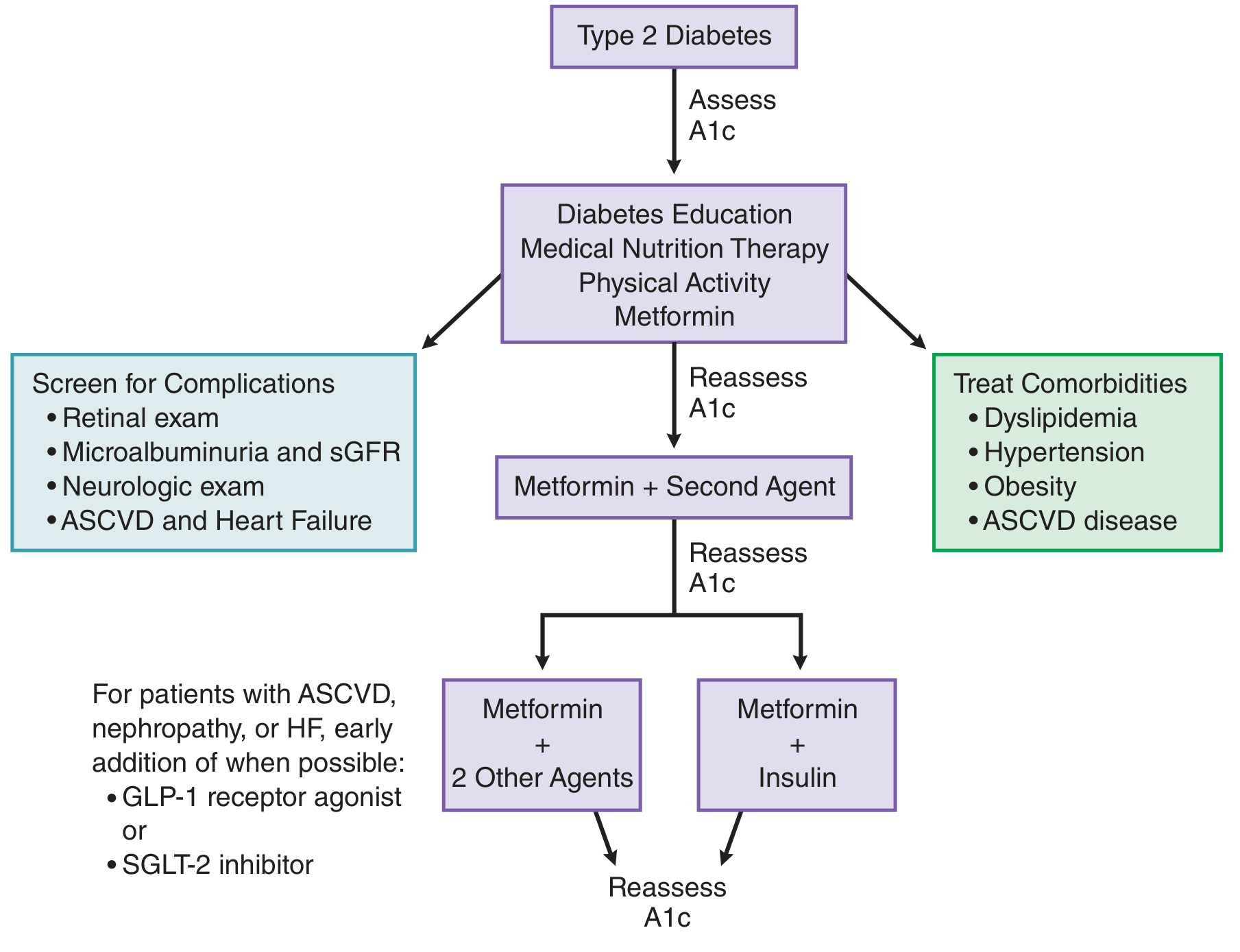
Step 0 - Initial Assessment
Before starting any medication, assess the following:
| Parameter | Target / Action |
|---|---|
| HbA1c | Measure baseline; target <7% for most patients |
| FPG / OGTT | Confirm diagnosis |
| eGFR / Creatinine | Required before Metformin (hold if eGFR <30) |
| Lipid profile | Screen for dyslipidemia |
| BP | Target <130/80 mmHg |
| BMI / Weight | Assess for obesity |
| Retinal exam | Baseline diabetic retinopathy screen |
| Microalbuminuria | Baseline nephropathy screen |
| CVD risk | ASCVD, heart failure, CKD present? |
Step 1 - Lifestyle + Metformin (Start at Diagnosis)
Lifestyle modifications (mandatory, reinforce at every visit):
- Prudent diet, caloric restriction, carbohydrate control
- Weight loss if BMI >25 (even 5-10% weight loss significantly improves glycemia)
- Aerobic exercise: 150 min/week minimum
- Diabetes education and self-monitoring of blood glucose
Pharmacotherapy - First Line:
Metformin (Drug of Choice)
| Detail | Information |
|---|---|
| Mechanism | Reduces hepatic gluconeogenesis, improves peripheral glucose uptake, decreases intestinal glucose absorption |
| Dose | Start 500 mg once or twice daily with meals; titrate slowly over 4-8 weeks |
| Max dose | 2000-2550 mg/day (benefit plateaus at 2000 mg) |
| XR formulation | 500-2000 mg once daily (fewer GI side effects) |
| Key advantages | No hypoglycemia, mild weight loss, low cost, reduces microvascular complications |
| Side effects | GI: nausea, diarrhea, bloating (minimize by slow titration + take with meals); Vitamin B12 deficiency - monitor periodically |
| Contraindications | eGFR <30 mL/min, active liver disease, alcohol excess, iodinated contrast (hold 48h) |
Reassess HbA1c at 3 months. If target not achieved, add a second agent.
Step 2 - Add Second Agent (if HbA1c still >7% after 2-3 months)
Drug choice depends on comorbidities:
A) Patient has ASCVD / High CV Risk
- Add GLP-1 Receptor Agonist (preferred): Liraglutide, Dulaglutide, Semaglutide
- Reduce CV events, promote weight loss, once weekly injection
- OR SGLT-2 Inhibitor: Empagliflozin, Canagliflozin, Dapagliflozin
- Reduce CV mortality, HF hospitalization
B) Patient has Heart Failure or Diabetic Nephropathy
- SGLT-2 Inhibitor preferred (Empagliflozin/Dapagliflozin)
- Reduces renal progression and HF hospitalization
- Caution: hold if eGFR <45 (canagliflozin) or <30 (empagliflozin)
C) Patient needs to avoid weight gain and hypoglycemia
- DPP-4 Inhibitor: Sitagliptin, Saxagliptin, Linagliptin
- Weight neutral, no hypoglycemia, safe in renal insufficiency
- Can be used with Metformin or TZD
D) Cost is a major concern
- Sulfonylurea (SU): Glipizide, Glimepiride
- Cheap and effective; risk of hypoglycemia + weight gain
- Avoid or use cautiously in elderly / those with erratic meals
Second Agent Quick Reference Table
| Drug Class | Example | HbA1c Reduction | Weight | Hypoglycemia | Special Use |
|---|---|---|---|---|---|
| GLP-1 agonist | Liraglutide, Semaglutide | 1-1.5% | Loss | No | CV protection |
| SGLT-2 inhibitor | Empagliflozin | 0.5-1% | Loss | No | HF/CKD protection |
| DPP-4 inhibitor | Sitagliptin | 0.5-0.8% | Neutral | No | Safe in CKD |
| Sulfonylurea | Glipizide | 1-1.5% | Gain | Yes | Low cost |
| TZD | Pioglitazone | 0.5-1.4% | Gain | No | NAFLD benefit |
| Meglitinide | Repaglinide | 0.5-1% | Neutral | Less | Postprandial spikes |
Reassess HbA1c at 3 months again. If still not at goal - escalate.
Step 3 - Triple Therapy / Insulin
If HbA1c remains above goal on dual therapy:
- Metformin + 2 Oral Agents (e.g., Metformin + SGLT-2 + DPP-4), OR
- Metformin + Basal Insulin (Glargine or Detemir, once nightly)
- 15-20% of T2DM patients will eventually need insulin
- Start basal insulin at 10 units at bedtime, titrate by 2 units every 3 days until fasting glucose 80-130 mg/dL
Monitoring Schedule
| Test | Frequency |
|---|---|
| HbA1c | Every 3 months until stable, then every 6 months |
| Fasting glucose / SMBG | Daily (patient self-monitors) |
| eGFR + Creatinine | Annually |
| Urine microalbumin | Annually |
| Lipid panel | Annually |
| Blood pressure | Every visit |
| Retinal exam | Annually |
| Foot examination | Annually (monofilament test, pulses) |
| Vitamin B12 | Annually (if on Metformin long-term) |
HbA1c Target for a 50-Year-Old
| Patient Profile | HbA1c Target |
|---|---|
| Otherwise healthy, long life expectancy | <7% (ADA standard) |
| Extensive comorbidities, risk of hypoglycemia | 7.5-8% |
| Short life expectancy / frail | 8-8.5% |
A 50-year-old with no major comorbidities should aim for HbA1c <7% to prevent micro- and macrovascular complications.
Comorbidity Management (Often Overlooked But Critical)
| Comorbidity | First-Line Drug |
|---|---|
| Hypertension | ACE inhibitor or ARB (also protects kidneys) |
| Dyslipidemia | Statin therapy (high-intensity if CV risk high) |
| Obesity | GLP-1 agonist or SGLT-2 inhibitor preferred |
| Microalbuminuria | ACE inhibitor/ARB + SGLT-2 inhibitor |
| ASCVD | GLP-1 agonist + Statin + Aspirin (if appropriate) |
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Table 51-6 & Figure 51-11
- Swanson's Family Medicine Review, Table 4.11
- Textbook of Family Medicine 9e, Diabetes Mellitus chapter
This is a shared conversation. Sign in to Orris to start your own chat.