Explain me 10 common heart diseases with ECG changes and ECG images of those diseases.
Reading File
Finding Sources
Searching the Web
ECG changes 10 common heart diseases with ECG images examples
Finding Sources
Finding Sources
Reading Web Page
ECG changes common heart diseases with images
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
ECG ventricular tachycardia pericarditis heart block Wolff-Parkinson-White pulmonary embolism ECG images
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Searching the Web
ECG pericarditis saddle shape ST elevation PR depression 12 lead ECG image
Loading Image
I now have an excellent collection of ECG images and clinical content from authoritative textbooks. Let me compile the comprehensive response.
10 Common Heart Diseases: ECG Changes with Images
1. ST-Elevation Myocardial Infarction (STEMI)
Mechanism: Complete occlusion of a coronary artery causes transmural ischemia, injuring the full myocardial wall thickness.
ECG Changes:
- Hyperacute T waves - earliest change (tall, broad, peaked)
- ST-segment elevation ≥1 mm in 2 contiguous leads (the key diagnostic finding)
- Reciprocal ST depression in leads facing the opposite wall
- Pathological Q waves - develop within hours to days (necrosis marker)
- T-wave inversion - evolves as injury resolves
- Location identifies the artery: V1-V4 = anterior (LAD), II/III/aVF = inferior (RCA), I/aVL/V5-V6 = lateral (LCx)
Anterior Wall STEMI (LAD occlusion) - ST elevation in V1-V4:
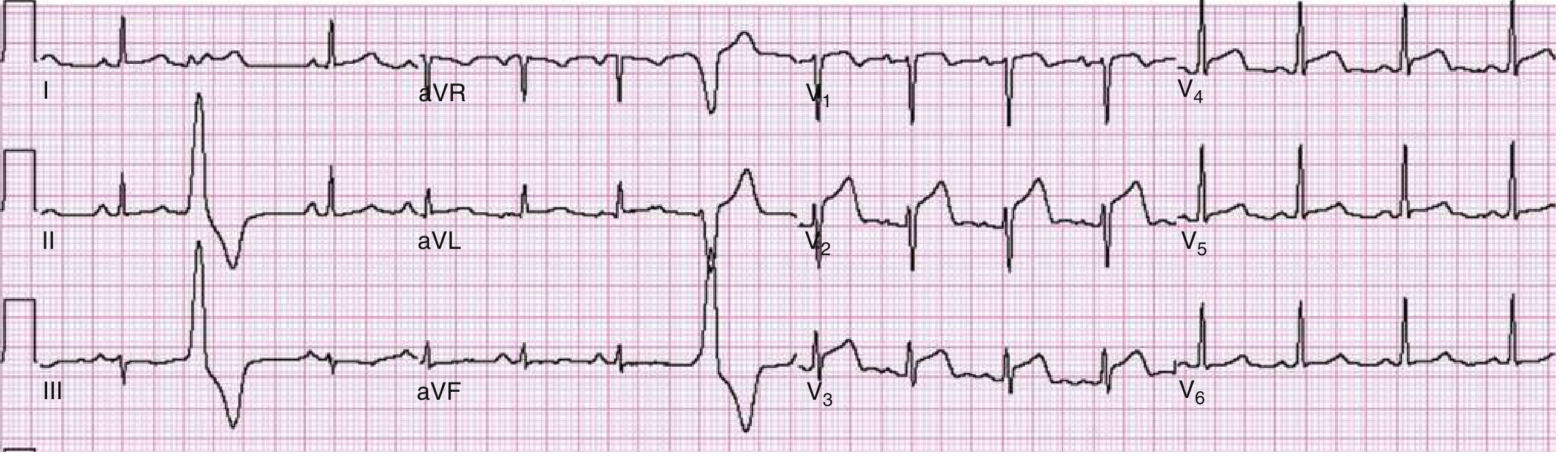 Fig: Anterior wall STEMI. ST elevation is evident in leads V1-V4. Emergency catheterization revealed 90% stenosis of the left anterior descending artery. - Rosen's Emergency Medicine
Fig: Anterior wall STEMI. ST elevation is evident in leads V1-V4. Emergency catheterization revealed 90% stenosis of the left anterior descending artery. - Rosen's Emergency Medicine
Anterolateral STEMI - ST elevation extending to V5, V6, I, aVL:
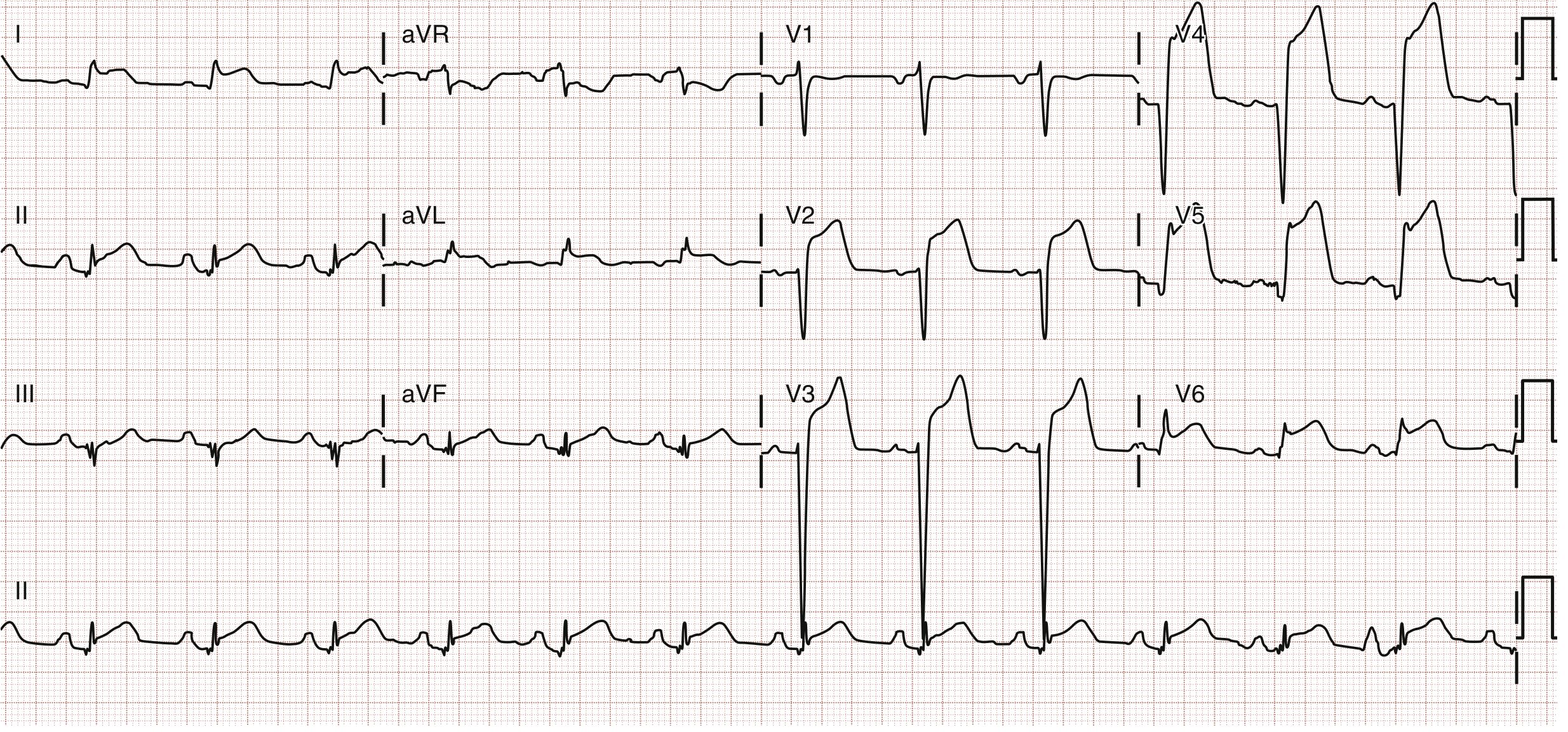 Fig: Anterolateral STEMI with ST elevation in V1-V6 and leads I and aVL. - Rosen's Emergency Medicine
Fig: Anterolateral STEMI with ST elevation in V1-V6 and leads I and aVL. - Rosen's Emergency Medicine
Inferior STEMI (RCA occlusion) - ST elevation in II, III, aVF:
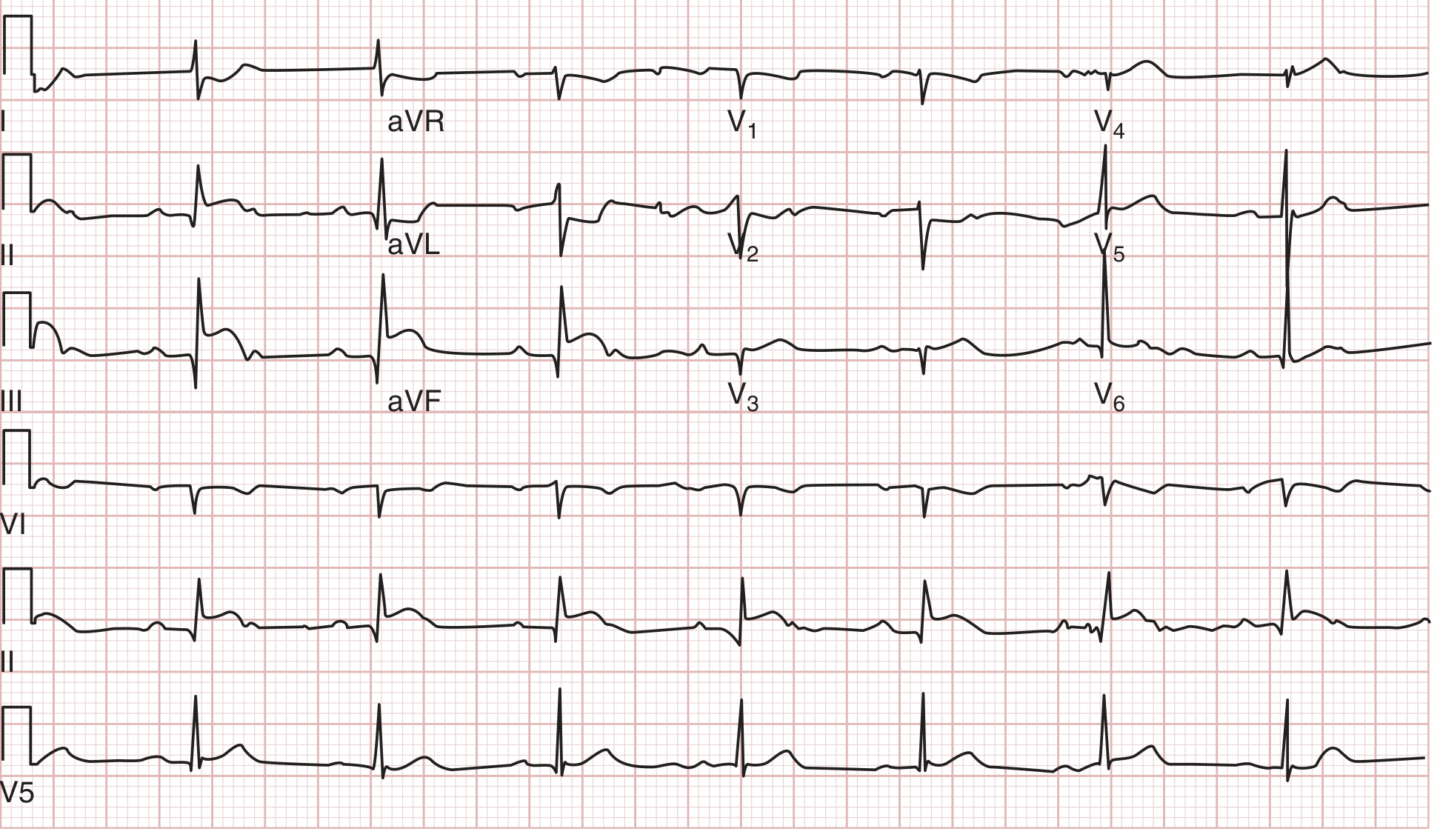 Fig: Inferior MI from RCA occlusion - ST elevation in III greater than II, with ST depression in I and aVL (reciprocal changes). - Tintinalli's Emergency Medicine
Fig: Inferior MI from RCA occlusion - ST elevation in III greater than II, with ST depression in I and aVL (reciprocal changes). - Tintinalli's Emergency Medicine
Right Ventricular Infarction (complicates inferior STEMI - requires right-sided leads):
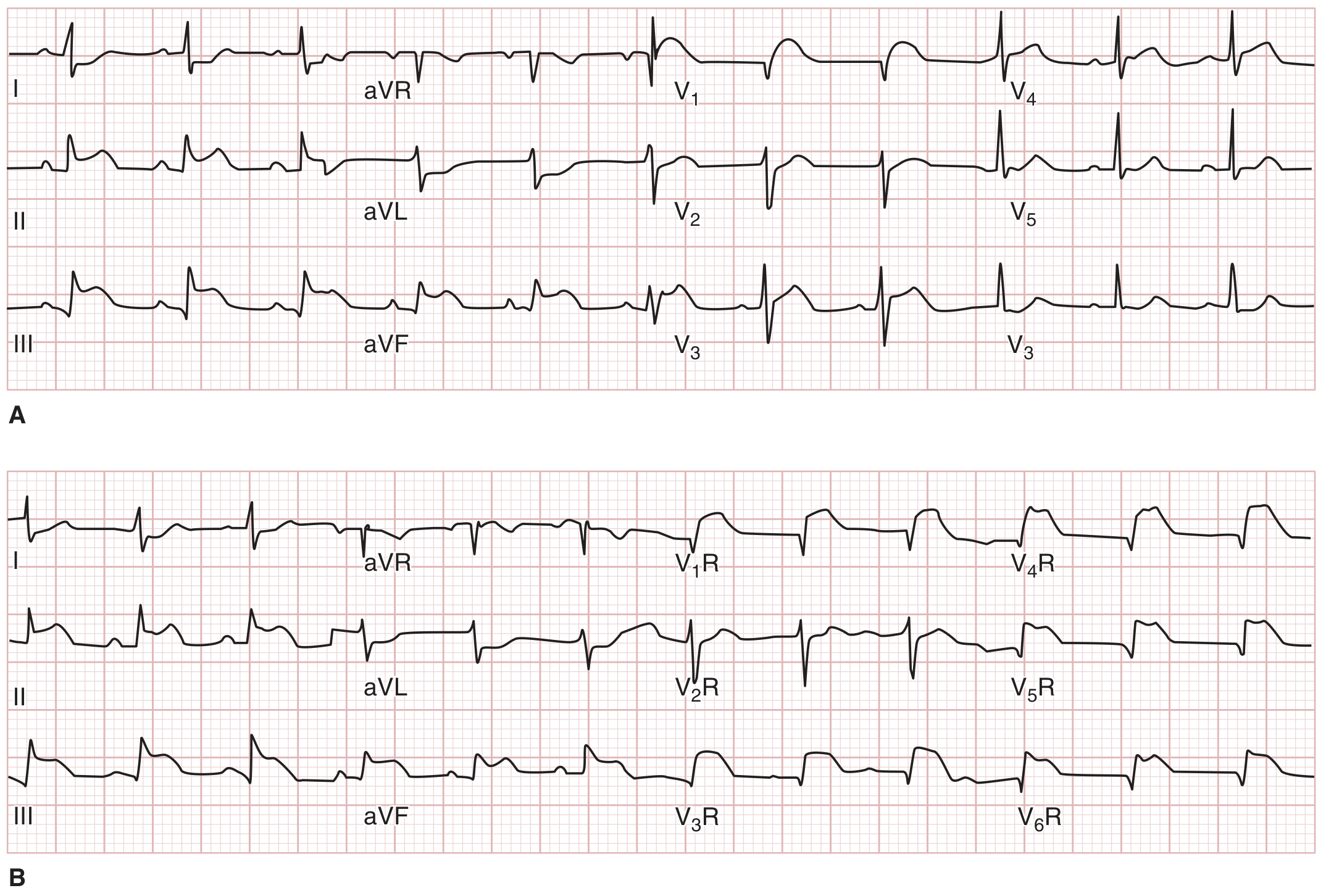 Fig: A - Inferior STEMI with ST elevation in V1 suggesting RV involvement. B - Right-sided leads confirming ST elevation in V1R-V6R. - Tintinalli's Emergency Medicine
Fig: A - Inferior STEMI with ST elevation in V1 suggesting RV involvement. B - Right-sided leads confirming ST elevation in V1R-V6R. - Tintinalli's Emergency Medicine
| Location | Elevated Leads | Reciprocal Depression |
|---|---|---|
| Anterior | V1-V4 | II, III, aVF |
| Lateral | I, aVL, V5-V6 | II, III, aVF |
| Inferior | II, III, aVF | I, aVL |
| Right Ventricle | V6R | - |
| Posterior | V8-V9 | V1-V3 (ST depression) |
2. Non-ST Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
Mechanism: Partial occlusion of a coronary artery - subendocardial ischemia without transmural injury.
ECG Changes:
- ST depression ≥0.5 mm in 2 contiguous leads (subendocardial ischemia)
- T-wave inversion - especially deep, symmetric inversions ("Wellens' sign" in V2-V3 = critical LAD stenosis)
- Transient ST elevation - may occur during pain, resolves at rest
- No pathological Q waves (no full-thickness necrosis in most cases)
- The ECG may be completely normal in up to 6% of confirmed NSTEMIs
Distinguishing feature: NSTEMI = troponin positive + ST depression/T inversion. Unstable angina = troponin negative + same ECG pattern.
3. Atrial Fibrillation (AF)
Mechanism: Multiple chaotic re-entry circuits in the atria fire at 350-600 bpm; the AV node filters this to an irregularly irregular ventricular response.
ECG Changes:
- Absence of distinct P waves - replaced by fibrillatory baseline (f waves, irregular undulations at 350-600/min)
- Irregularly irregular RR intervals - the hallmark
- Narrow QRS complexes (unless aberrant conduction or pre-excitation)
- Rate: can be bradycardic (<60), normal (60-100), or with rapid ventricular response (>100)
ECG showing a PAC initiating atrial fibrillation:
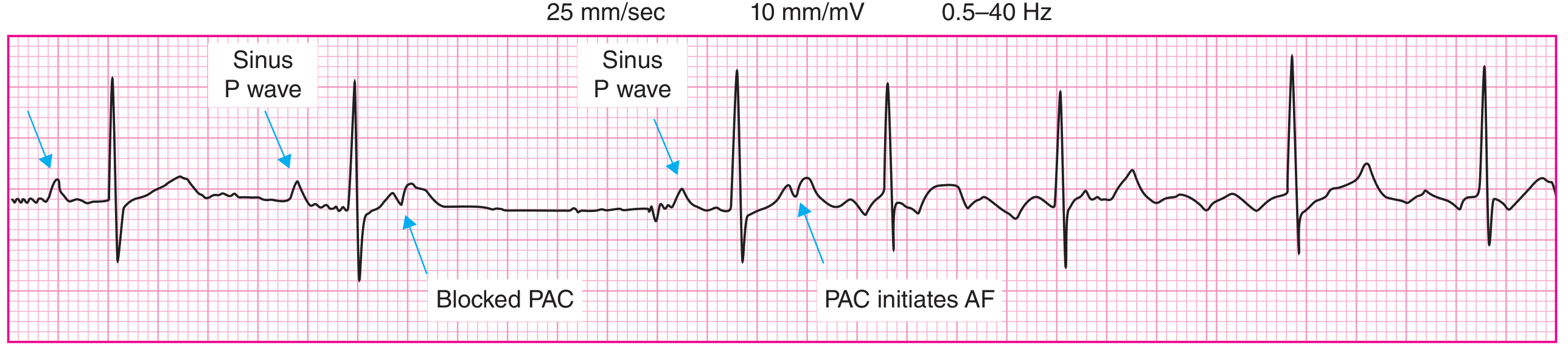 Fig: ECG showing sinus P waves, a blocked PAC, then a PAC initiating atrial fibrillation. - Harrison's Principles of Internal Medicine 22E
Fig: ECG showing sinus P waves, a blocked PAC, then a PAC initiating atrial fibrillation. - Harrison's Principles of Internal Medicine 22E
Atrial fibrillation with fibrillatory p waves (f waves):
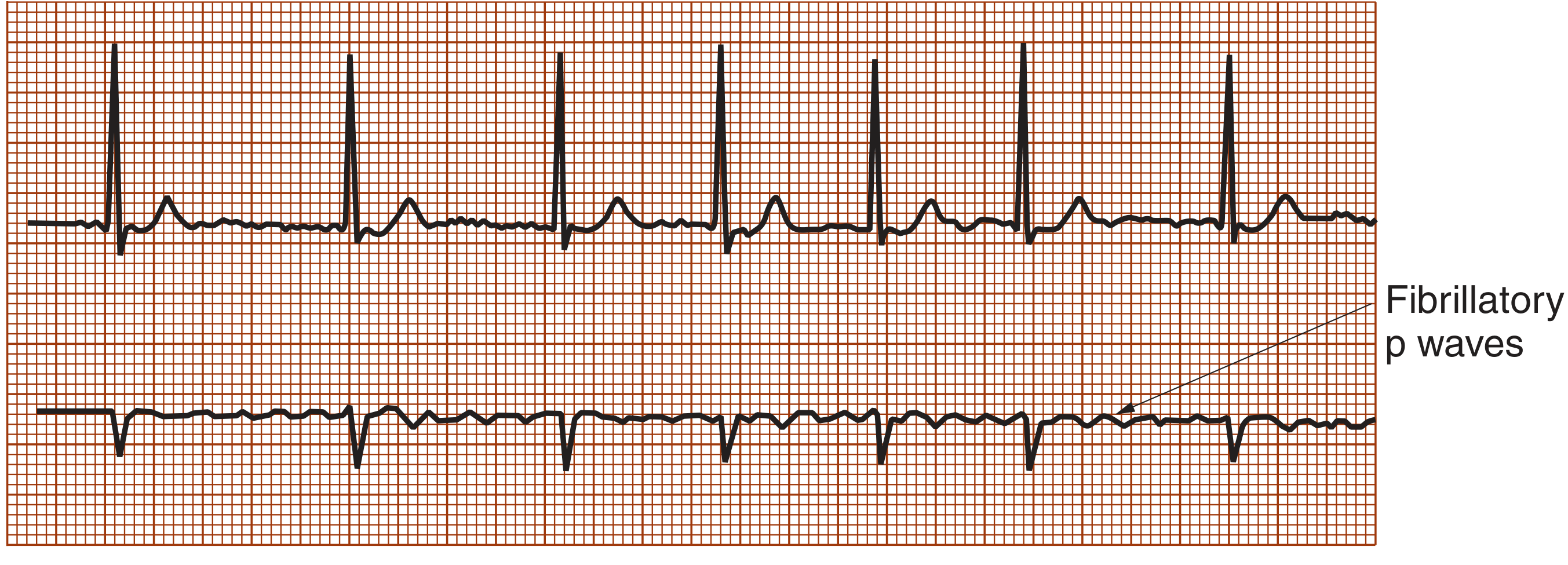 Fig: ECG of atrial fibrillation - irregularly irregular rhythm with fibrillatory (f) waves replacing normal P waves. - Symptom to Diagnosis, 4th Ed.
Fig: ECG of atrial fibrillation - irregularly irregular rhythm with fibrillatory (f) waves replacing normal P waves. - Symptom to Diagnosis, 4th Ed.
4. Complete Heart Block (Third-Degree AV Block)
Mechanism: Complete dissociation of atrial and ventricular conduction - no sinus impulses conduct through the AV node. The ventricles are driven by a slower escape rhythm (junctional or ventricular).
ECG Changes:
- P waves and QRS complexes are completely independent (AV dissociation)
- Regular P-P intervals (atrial rate normal, 60-100/min)
- Regular but slower RR intervals (ventricular escape rate 20-40/min if ventricular, 40-60/min if junctional)
- Wide QRS complexes if ventricular escape; narrow QRS if junctional escape
- PR interval is completely variable (not constant) - this distinguishes it from 2:1 block
Complete Heart Block ECG with His-bundle recording:
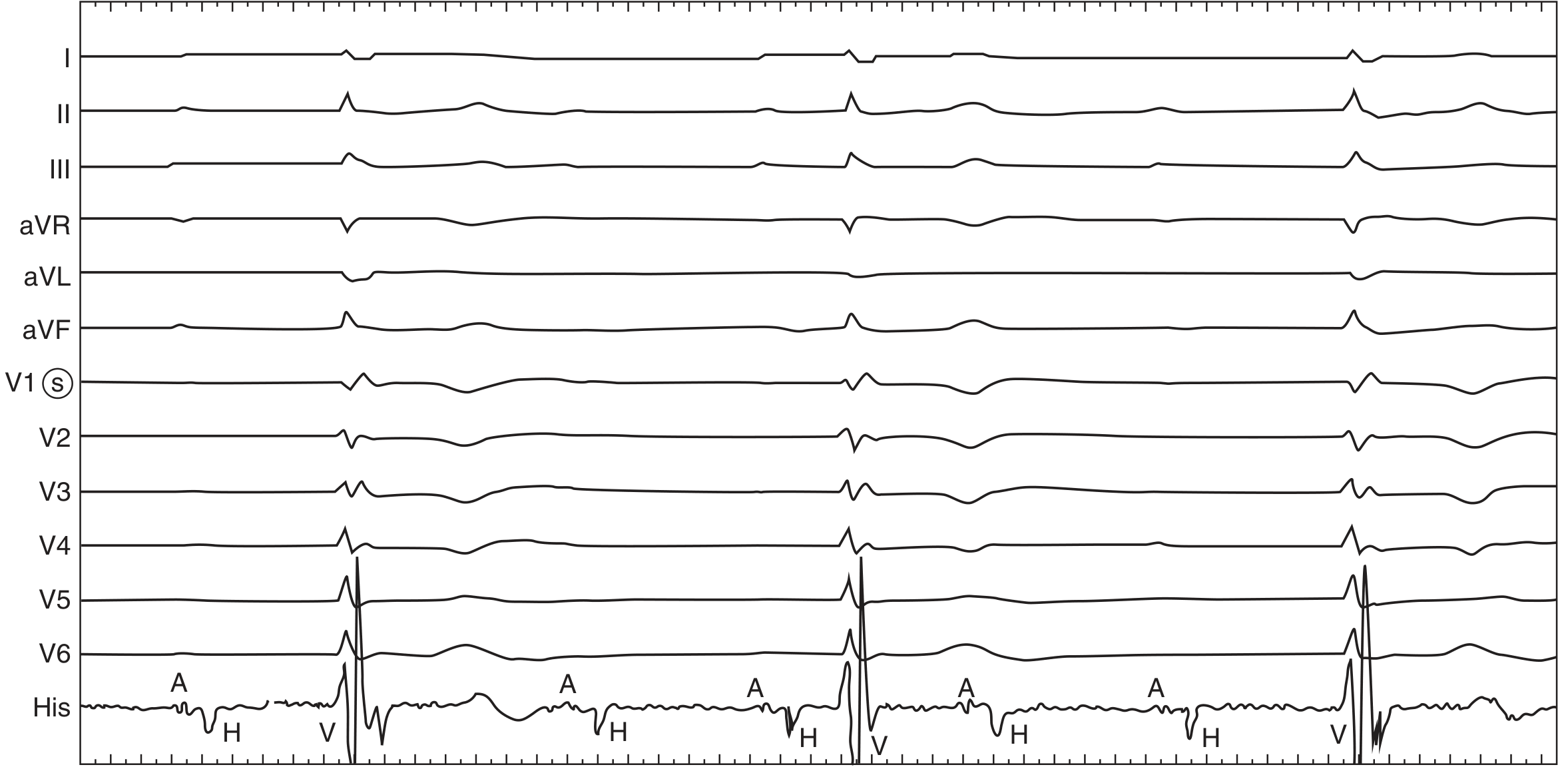 Fig: Complete heart block. Surface leads show AV dissociation - atrial (A) and His (H) potentials occur without relationship to ventricular (V) activity. Most beats are conducted through an escape rhythm. - Fuster and Hurst's The Heart, 15th Ed.
Fig: Complete heart block. Surface leads show AV dissociation - atrial (A) and His (H) potentials occur without relationship to ventricular (V) activity. Most beats are conducted through an escape rhythm. - Fuster and Hurst's The Heart, 15th Ed.
5. Ventricular Tachycardia (VT)
Mechanism: Rapid ventricular ectopic focus or re-entrant circuit fires faster than the sinus node (usually due to ischemia, cardiomyopathy, or electrolyte disturbance).
ECG Changes:
- Wide QRS complexes (≥120 ms) - the defining feature of VT
- Rate: 100-250 bpm (usually 140-200)
- Regular rhythm (monomorphic VT) or irregular (polymorphic VT / Torsades)
- AV dissociation - P waves independent of QRS (present in ~50%; confirms VT)
- Fusion beats - partial capture of ventricle by sinus impulse (pathognomonic for VT)
- Capture beats - narrow QRS amid wide complexes (brief AV conduction; diagnostic)
- Morphology criteria: Brugada, Josephson's notching, concordance in chest leads
Key point: Any wide-complex tachycardia should be presumed VT until proven otherwise.
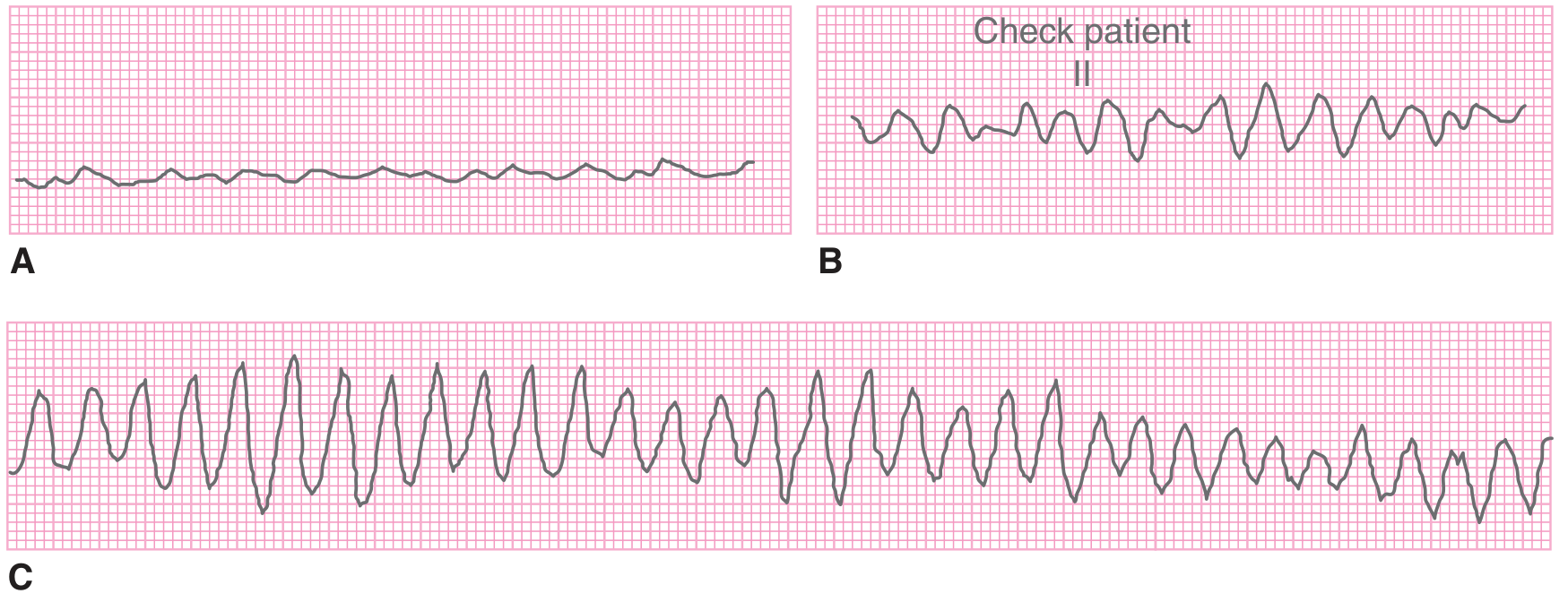
6. Ventricular Fibrillation (VF)
Mechanism: Completely disorganized ventricular depolarization - no coordinated contraction, no cardiac output. A cardiac arrest rhythm requiring immediate defibrillation.
ECG Changes:
- No identifiable P waves, QRS complexes, or T waves
- Chaotic, irregular deflections varying in amplitude and morphology
- Can be fine (low amplitude, <3 mm - worse prognosis, harder to defibrillate) or coarse (high amplitude - more recently onset)
- Coarse VF can mimic VT morphologically
Common causes: Acute MI (most common), hypokalemia, long QT syndrome, cardiomyopathy, hypothermia, electrocution, commotio cordis.
7. Acute Pericarditis
Mechanism: Inflammation of the pericardial sac irritates the epicardial surface of the heart, causing diffuse myocardial current-of-injury pattern (unlike focal MI changes).
ECG Changes (4 stages):
- Stage 1 (acute, hours-days): Diffuse concave-upward ST elevation in most leads (I, II, aVF, V2-V6) PLUS PR segment depression (atrial injury) - most specific finding. Reciprocal ST elevation in aVR with PR elevation in aVR.
- Stage 2 (days-weeks): ST normalizes, T waves flatten
- Stage 3: Diffuse T-wave inversion throughout
- Stage 4: ECG normalization (or permanent T inversion)
Key differences from STEMI: Pericarditis ST elevation is (1) diffuse (not regional), (2) concave upward ("saddle-shaped"), (3) accompanied by PR depression, and (4) without reciprocal ST depression (except aVR).
8. Left Ventricular Hypertrophy (LVH)
Mechanism: Pressure or volume overload (hypertension, aortic stenosis, hypertrophic cardiomyopathy) causes left ventricular myocyte hypertrophy, increasing the electrical mass and shifting the QRS vector leftward and posteriorly.
ECG Changes:
- Voltage criteria (several, pick one):
- SV1 + RV5 or RV6 >35 mm (Sokolow-Lyon)
- RaVL >20 mm (women) or >28 mm (men)
- R wave in lead I + S wave in lead III >25 mm (Cornell)
- Left atrial enlargement - broad, notched P wave (P mitrale) in lead II, or biphasic P in V1
- Left axis deviation (QRS axis -30° to -90°)
- "LVH strain pattern": ST depression + T-wave inversion in I, aVL, V5-V6 (the leads with dominant R waves)
- QRS widening as LVH progresses toward LBBB
Note: Voltage criteria alone have low sensitivity (~50%) but high specificity. Repolarization (strain) changes increase diagnostic certainty.
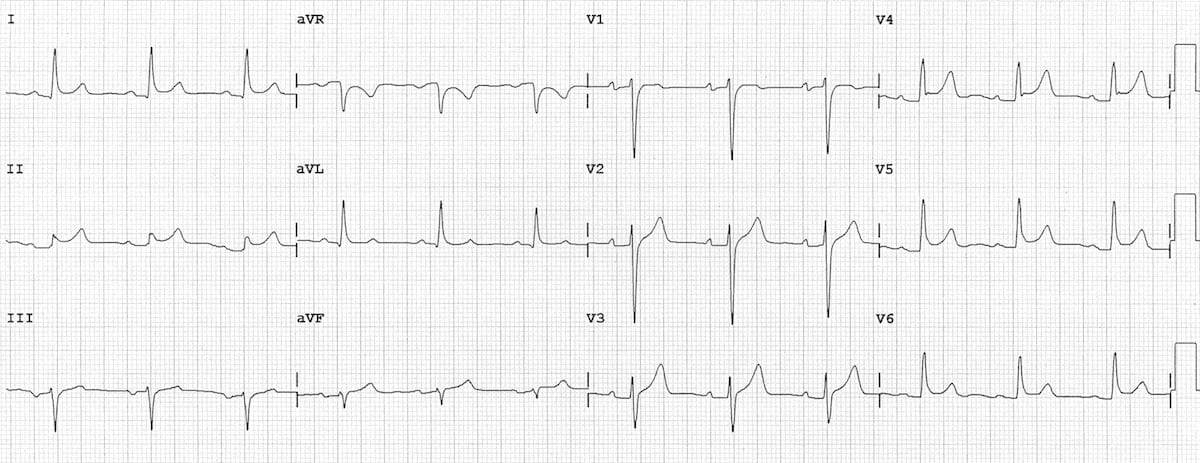
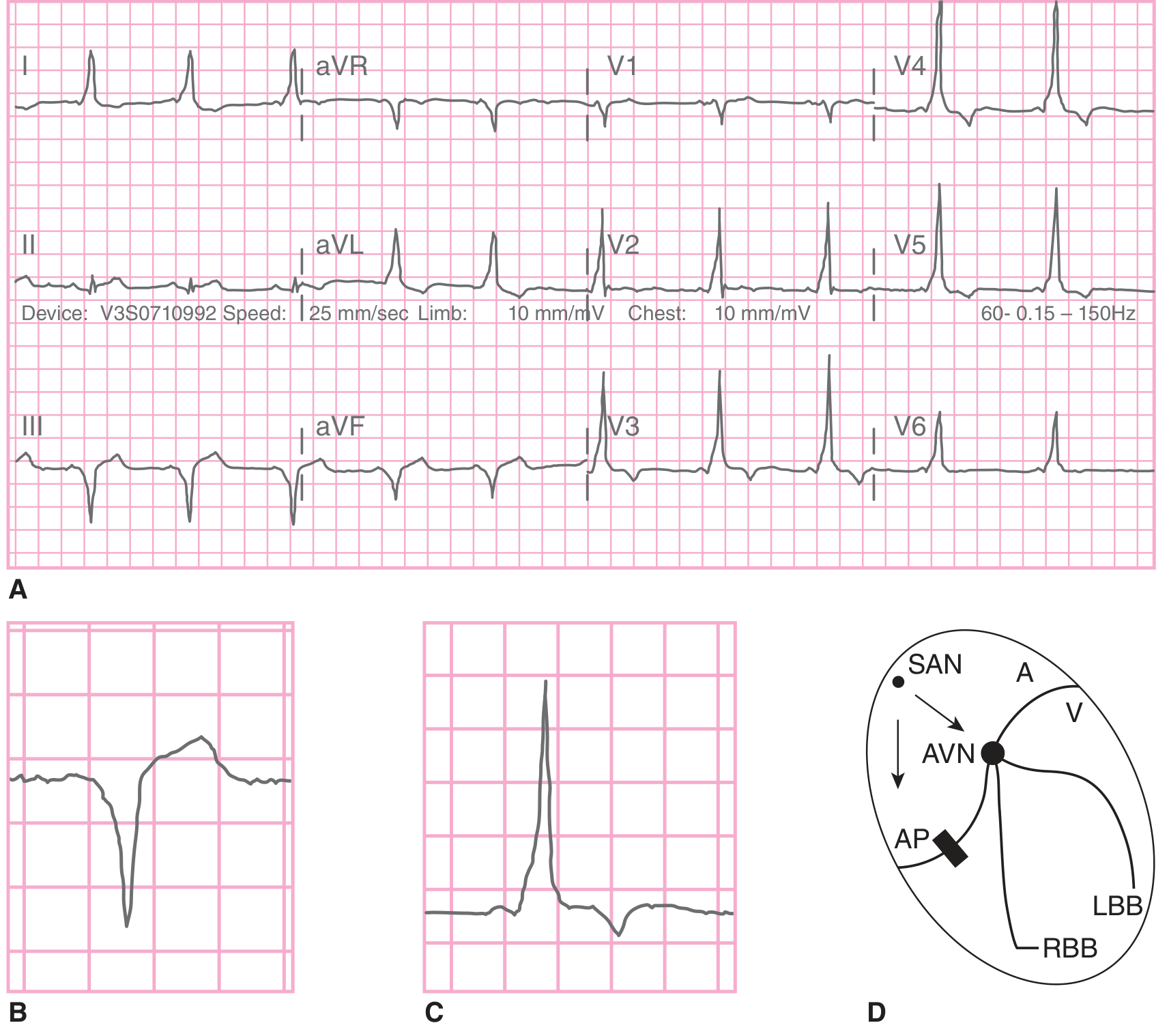
9. Wolff-Parkinson-White (WPW) Syndrome
Mechanism: An accessory pathway (Bundle of Kent) bypasses the AV node, creating a direct atrial-ventricular electrical connection. This allows:
- Ventricular pre-excitation during sinus rhythm (causing delta waves)
- Re-entrant tachycardias (AV reciprocating tachycardia at 160-220 bpm)
- Rapid ventricular response in AF (potentially causing VF)
ECG Changes (during sinus rhythm - the classic triad):
- Short PR interval (<120 ms) - impulse bypasses AV node delay
- Delta wave - slurred initial upstroke of the QRS (earliest ventricular activation via accessory pathway)
- Wide QRS (>120 ms) - fusion of delta wave + normal His-Purkinje activation
- Discordant ST-T changes - ST/T waves directed opposite to the delta wave and QRS
- Pseudo-Q waves - negative delta waves can mimic infarction
During tachycardia:
- Orthodromic AVRT: narrow QRS, regular, 160-220 bpm (no delta wave)
- Antidromic AVRT: wide QRS, mimics VT
- AF with accessory pathway: irregular wide bizarre QRS, rate can reach 300 bpm
10. Pulmonary Embolism (PE)
Mechanism: Acute pulmonary artery obstruction causes acute right heart pressure overload - the right ventricle dilates and shifts the cardiac axis rightward, affecting the ECG pattern.
ECG Changes:
- Sinus tachycardia - most common finding (occurs in ~44% of PE)
- S1Q3T3 pattern - deep S wave in lead I + Q wave in III + T-wave inversion in III (occurs in ~20%)
- Right bundle branch block (RBBB) - new incomplete or complete RBBB (right ventricular strain)
- Right axis deviation
- T-wave inversions in V1-V4 - right ventricular strain pattern (anterior leads)
- P pulmonale - tall peaked P waves in lead II (right atrial enlargement)
- Atrial fibrillation or flutter - may be triggered by right atrial stretch
- Low-voltage QRS in massive PE with cardiac tamponade physiology
- Important: ECG is normal in ~25% of PE cases; a normal ECG does not exclude PE
Key clinical point: The S1Q3T3 pattern is specific but insensitive. The combination of sinus tachycardia + new RBBB + anterior T-wave inversions should raise strong suspicion for PE.
Quick Reference Summary Table
| Disease | Key ECG Findings |
|---|---|
| STEMI | Regional ST elevation, reciprocal depression, Q waves |
| NSTEMI/UA | ST depression, T-wave inversion, normal in some |
| Atrial Fibrillation | No P waves, irregularly irregular rhythm |
| Complete Heart Block | AV dissociation, slow escape rhythm |
| Ventricular Tachycardia | Wide QRS >120ms, rate 100-250, AV dissociation |
| Ventricular Fibrillation | Chaotic baseline, no QRS/P/T complexes |
| Acute Pericarditis | Diffuse concave ST elevation, PR depression |
| LVH | High voltage (SV1+RV5 >35mm), strain pattern |
| WPW Syndrome | Short PR, delta wave, wide QRS |
| Pulmonary Embolism | Tachycardia, S1Q3T3, RBBB, anterior T inversions |
Sources: Rosen's Emergency Medicine 9e, Tintinalli's Emergency Medicine, Harrison's Principles of Internal Medicine 22E (2025), Fuster and Hurst's The Heart 15e, Symptom to Diagnosis 4e, LITFL ECG Library
This is a shared conversation. Sign in to Orris to start your own chat.