teach me stroke consultant level internal medicine get most content from harrison and teach me all types / variants of stroke with real time imaging and also at the end of discussion also arrange mcqs atleast 15 for better understanding and evaluation
Reading File
Finding Sources
Searching the Web
stroke types classification ischemic hemorrhagic imaging radiology 2024 2025
Searching PubMed
"ischemic stroke" AND classification AND management
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have extensive Harrison's content, key imaging, and pathophysiology diagrams. Now I have enough to compile the full consultant-level teaching session. Let me compose the comprehensive answer.
STROKE - Consultant-Level Internal Medicine Teaching
Based primarily on Harrison's Principles of Internal Medicine, 22nd Edition (2025)
OVERVIEW & EPIDEMIOLOGY
Stroke is defined as an acute neurologic deficit of vascular origin lasting >24 hours (or any duration if imaging confirms infarction or hemorrhage). Transient Ischemic Attack (TIA) is identical in mechanism but resolves within 24 hours with no infarct on imaging - it is now understood as a neurologic emergency, not a benign event, as ~10-15% of TIA patients stroke within 90 days, with the highest risk in the first 48 hours.
Global burden: ~795,000 strokes/year in the US. Stroke is the 5th leading cause of death and a leading cause of disability. About 87% are ischemic, 13% hemorrhagic.
MASTER CLASSIFICATION OF STROKE
STROKE
├── ISCHEMIC (87%)
│ ├── Large-vessel atherothrombotic
│ ├── Cardioembolic
│ ├── Small-vessel (lacunar)
│ ├── Cryptogenic / ESUS
│ └── Other determined etiology
│ (dissection, vasculitis, hypercoagulable)
│
└── HEMORRHAGIC (13%)
├── Intracerebral Hemorrhage (ICH)
│ ├── Hypertensive (deep / basal ganglia / pons)
│ ├── Cerebral Amyloid Angiopathy (lobar)
│ ├── AVM / cavernoma
│ └── Secondary (coagulopathy, tumor)
└── Subarachnoid Hemorrhage (SAH)
├── Aneurysmal (ruptured berry aneurysm)
└── Non-aneurysmal (perimesencephalic, AVM)
PART I: ISCHEMIC STROKE
PATHOPHYSIOLOGY OF ISCHEMIC STROKE
(Harrison's Ch. 438)
Acute arterial occlusion reduces cerebral blood flow (CBF) to the region supplied. The degree of ischemia depends on collateral flow, site of occlusion, and systemic blood pressure.
CBF thresholds:
| CBF (mL/100g/min) | Effect |
|---|---|
| 0 | Brain death in 4-10 minutes |
| <16-18 | Infarction within 1 hour |
| <20 | Ischemia without infarction if brief |
| Normal: 50-60 | Normal function |
The ischemic core is irreversibly infarcted tissue. The surrounding ischemic penumbra is dysfunctional but viable tissue - saving it is the entire goal of reperfusion therapy.
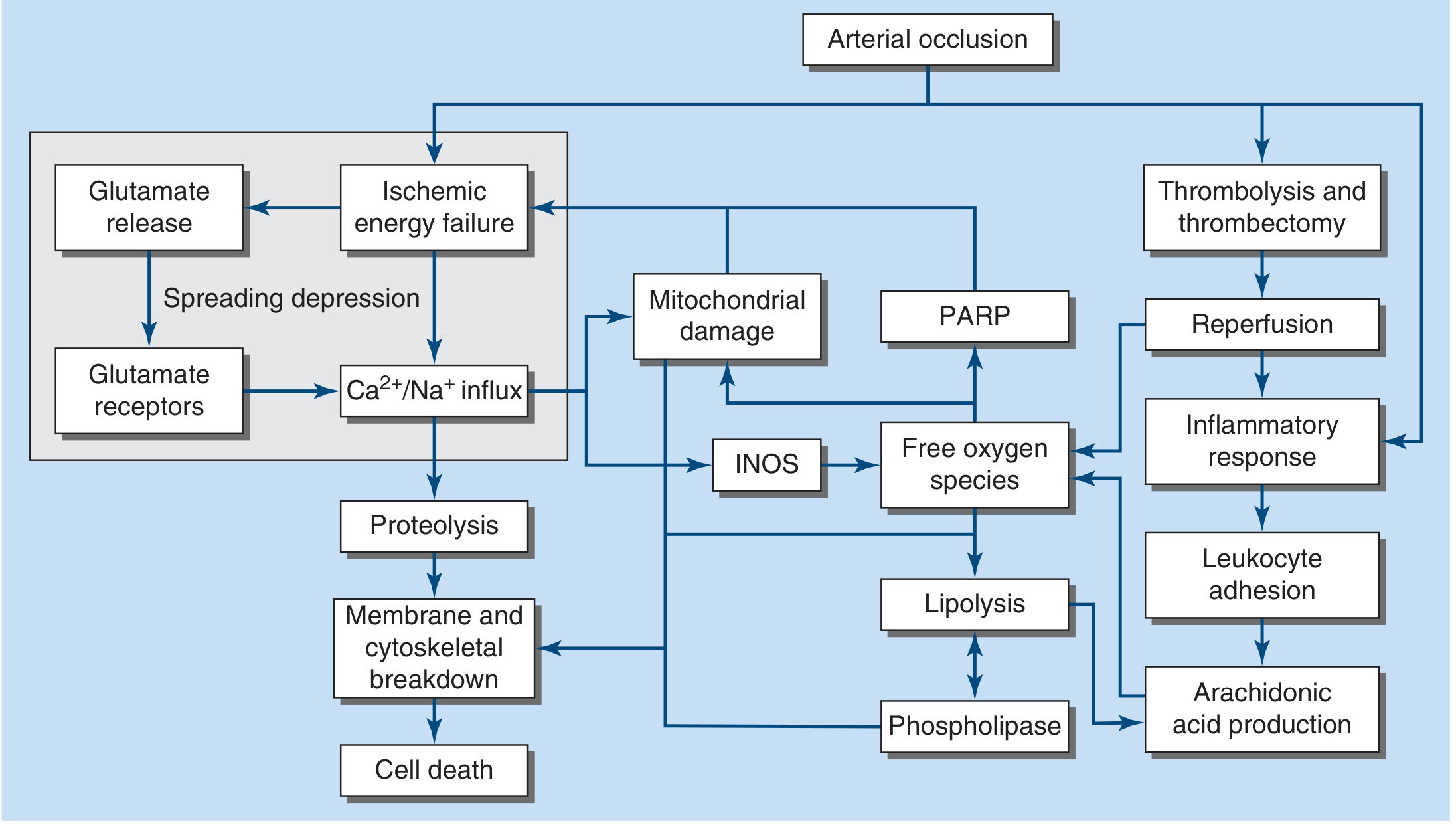
FIGURE 438-1 (Harrison's): The cascade from arterial occlusion → ischemic energy failure → glutamate release → Ca²⁺/Na⁺ influx → proteolysis → membrane breakdown → cell death. Simultaneously: mitochondrial damage, free oxygen species, INOS activation, lipolysis → phospholipase activation. The right arm shows thrombolysis/thrombectomy → reperfusion → inflammatory response → leukocyte adhesion → arachidonic acid production.
Molecular mechanism in detail (Harrison's):
- ATP depletion → membrane ion pumps fail → Na⁺/Ca²⁺ enter cells → cell swelling and depolarization
- Depolarization → glutamate release from synapses; glial cells fail to reuptake glutamate
- Sustained extracellular glutamate → NMDA/AMPA receptor activation → Ca²⁺ influx → reactive oxygen species (ROS)
- ROS damage DNA, lipid membranes, cytoskeleton
- Innate immune activation within hours: microglial activation + peripheral immune cell infiltration → protease + ROS release → secondary injury
- Fever worsens ischemia; hyperglycemia (>11.1 mmol/L / 200 mg/dL) dramatically worsens outcomes - both should be actively treated
ETIOLOGY OF ISCHEMIC STROKE
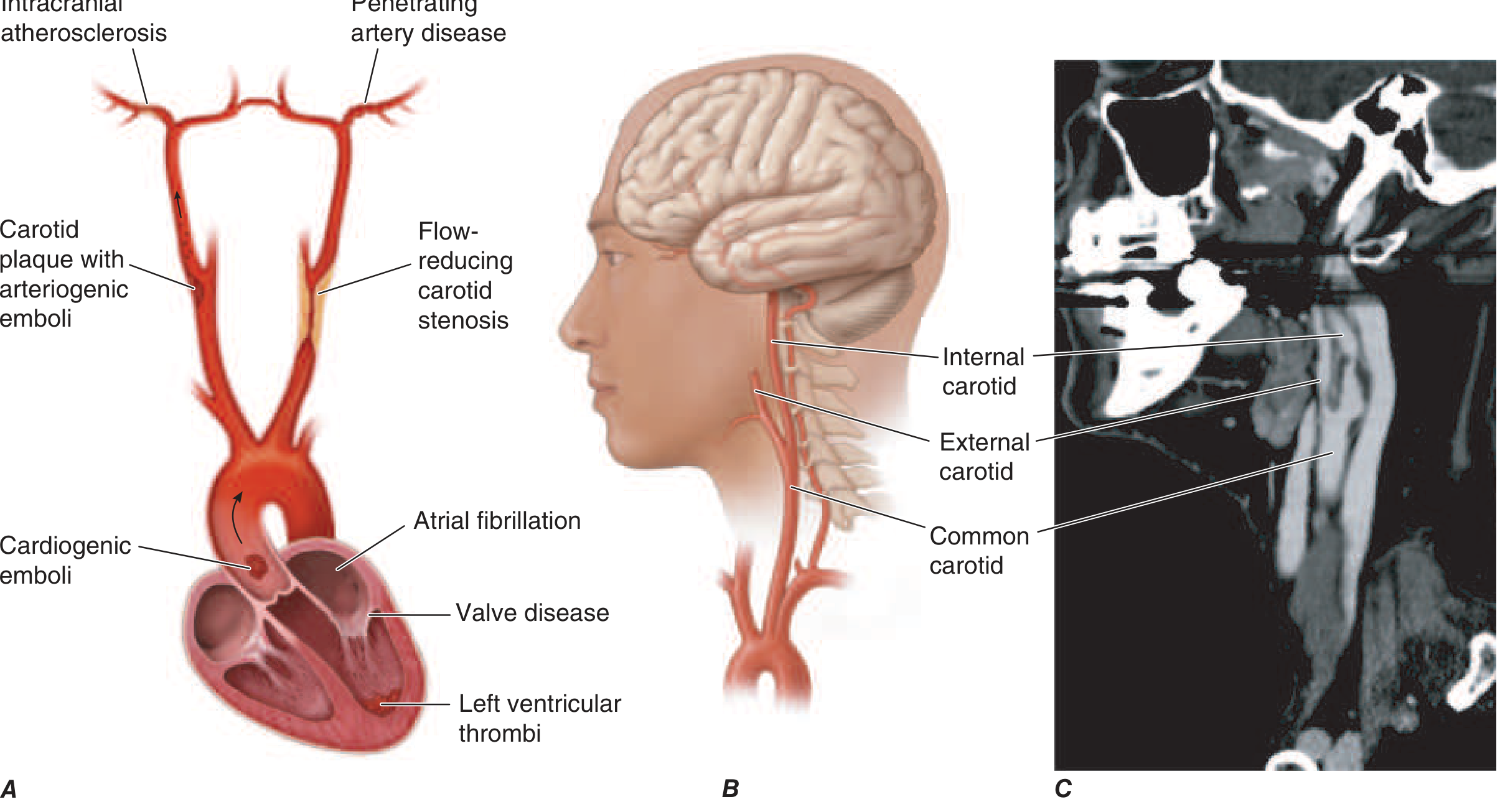
FIGURE 438-4 (Harrison's): Three major mechanisms - (1) Cardioembolic (AF, valve disease, LV thrombus); (2) Artery-to-artery emboli from carotid atherosclerotic plaque; (3) In-situ thrombosis of small penetrating arteries (lacunar). Right panel: CTA showing high-grade ICA stenosis.
Harrison's Table 438-2 - Causes of Ischemic Stroke:
| COMMON CAUSES | UNCOMMON CAUSES |
|---|---|
| Lacunar stroke (small vessel) | Hypercoagulable disorders |
| Large-vessel thrombosis | Protein C/S deficiency |
| Dehydration | Antiphospholipid syndrome |
| Artery-to-artery emboli (carotid bifurcation, aortic arch) | Factor V Leiden, Prothrombin G20210A |
| Atrial fibrillation | Sickle cell anemia |
| Mural thrombus (post-MI, dilated CMP) | Polycythemia vera |
| Valvular lesions (mitral stenosis, mechanical valve) | SLE, Homocysteinemia |
| Bacterial endocarditis | TTP, DIC |
| Carotid/vertebral dissection | CADASIL |
TYPE 1: LARGE-VESSEL ATHEROTHROMBOTIC STROKE
Mechanism: Atherosclerosis of major intracranial/extracranial arteries (ICA, MCA, basilar) → in-situ thrombus or artery-to-artery embolism.
Risk factors: Hypertension, diabetes, smoking, hyperlipidemia, age.
Typical features:
- Gradual or stuttering onset (vs. embolic = maximal-at-onset)
- Preceded by TIAs in the same territory
- Symptoms often worse with standing (hemodynamic mechanism)
- Carotid bruit may be audible
Key syndromes by vessel:
Middle Cerebral Artery (MCA) Stroke
(The most common clinically significant ischemic stroke)
The MCA supplies the lateral hemisphere, internal capsule (via lenticulostriate perforators), basal ganglia.
Complete MCA occlusion (M1):
- Contralateral hemiplegia + hemianesthesia
- Contralateral homonymous hemianopia
- Conjugate gaze deviation toward the lesion side (ipsilateral)
- Dysarthria
- Dominant hemisphere: Global aphasia (Broca + Wernicke)
- Non-dominant hemisphere: Anosognosia, hemispatial neglect, constructional apraxia
Partial/branch MCA occlusion:
- Superior division (frontal/parietal): Broca's aphasia (dominant) + arm/face weakness > leg
- Inferior division (temporal): Wernicke's aphasia (dominant) + hemianopia without hemiparesis
Anterior Cerebral Artery (ACA) Stroke
- Leg weakness and sensory loss >> arm (the medial hemisphere leg area is supplied by ACA)
- Urinary incontinence (parasagittal motor cortex)
- Contralateral grasp reflex, abulia (frontal lobe)
- Bilateral ACA infarction → akinetic mutism
Internal Carotid Artery (ICA) Occlusion
- Can be asymptomatic if circle of Willis collaterals are adequate
- Symptomatic: ipsilateral monocular blindness (retinal TIA = amaurosis fugax) + contralateral hemiplegia
- "Middle cerebral + anterior cerebral" combined territory infarct
Posterior Cerebral Artery (PCA) - Two Syndromes
P1 Syndrome (proximal - thalamic/midbrain):
- Thalamic syndrome: contralateral sensory loss (all modalities), spontaneous pain, choreoathetosis
- Weber's syndrome: ipsilateral CN III palsy + contralateral hemiplegia (peduncular)
- Claude's syndrome: CN III palsy + contralateral ataxia
P2 Syndrome (distal - cortical):
- Contralateral homonymous hemianopia (macular sparing common)
- Bilateral PCA: cortical blindness (Anton's syndrome - patient denies blindness)
- Memory defect (hippocampal infarction)
- Prosopagnosia (non-dominant)
- Alexia without agraphia (dominant - posterior corpus callosum + left calcarine)
TYPE 2: CARDIOEMBOLIC STROKE
(Harrison's Ch. 438 - Cardioembolic Stroke)
Mechanism: Embolus from cardiac source → typically large vessel occlusion → abrupt maximal-at-onset deficit.
Sources:
- Atrial fibrillation (most common): left atrial appendage thrombus
- Left ventricular thrombus (post-MI, dilated cardiomyopathy)
- Valvular disease (mitral stenosis, mechanical valve, endocarditis)
- Patent foramen ovale (PFO) + paradoxical embolism
- Atrial myxoma, nonbacterial thrombotic endocarditis
Clinical clues:
- Sudden onset, maximal at onset
- Multiple territory infarcts or hemorrhagic transformation on imaging
- Systemic emboli (renal, splenic, limb)
- Known cardiac disease / AF on ECG
- Younger patient with no vascular risk factors
Harrison's key point on AF: Patients with non-valvular AF have a 5x increased stroke risk. CHA₂DS₂-VASc score guides anticoagulation. DOACs (apixaban, rivaroxaban) are preferred over warfarin.
Workup: ECG, 24-72h cardiac monitoring (long-term if cryptogenic), echocardiogram (TTE + TEE), bubble study for PFO.
TYPE 3: SMALL-VESSEL (LACUNAR) STROKE
(Harrison's - Small-Vessel Stroke section)
Mechanism: Lipohyalinosis and microatheroma of small penetrating arteries (lenticulostriate, thalamoperforators, pontine perforators) in chronically hypertensive patients → small deep infarcts ("lacunes," typically 3-15 mm).
Locations: Putamen, internal capsule, thalamus, caudate, pons, corona radiata.
Classic lacunar syndromes (Harrison's "pure" syndromes):
| Syndrome | Location | Features |
|---|---|---|
| Pure motor hemiplegia | Posterior limb internal capsule or pons | Face + arm + leg weakness, no sensory, no cortical signs |
| Pure sensory stroke | VPL thalamus | Contralateral hemisensory loss, no motor |
| Sensorimotor stroke | Thalamocapsular | Combined motor + sensory |
| Ataxic hemiparesis | Pons or internal capsule | Ipsilateral arm ataxia + leg weakness |
| Clumsy hand-dysarthria | Pons | Dysarthria + hand clumsiness |
Key teaching point: Lacunar strokes are NOT associated with cortical signs (no aphasia, no neglect, no hemianopia, preserved consciousness). This is because the cortex itself is not infarcted.
Imaging: MRI DWI (most sensitive acutely). CT often misses small lacunes, especially in posterior fossa.
TYPE 4: CRYPTOGENIC STROKE / EMBOLIC STROKE OF UNKNOWN SOURCE (ESUS)
Defined as infarction not attributable to a defined source after full workup. ~25-30% of ischemic strokes. The concept of ESUS (Hart 2014) requires: non-lacunar infarct on CT/MRI, no proximal arterial stenosis, no high-risk cardiac source, no other specific cause.
Ongoing trials address anticoagulation vs antiplatelet therapy in ESUS. Recent meta-analyses (PMID 40555310, 2025) examine the role of left atrial septal pouch and TEE findings in cryptogenic stroke workup.
TYPE 5: LESS COMMON/SPECIFIC CAUSES
Carotid/vertebral artery dissection:
- Young patients, often after neck trauma, chiropractic manipulation, or spontaneous
- Ipsilateral neck pain + Horner's syndrome + stroke
- Imaging: CTA/MRA showing "flame sign" or intramural hematoma
- Treatment: Anticoagulation or antiplatelet (CADISS trial showed equivalence)
CADASIL (Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy):
- Mutation in NOTCH3 gene
- Recurrent lacunar strokes + migraine with aura + dementia + psychiatric symptoms
- White matter lesions on MRI (especially anterior temporal poles - pathognomonic)
Cerebral venous sinus thrombosis (CVST):
- Headache ± seizure ± focal deficit
- Associated with oral contraceptives, pregnancy, thrombophilia, infection
- CT: "empty delta sign" (after contrast); MRI/MRV confirms
- Treatment: Anticoagulation (even with hemorrhagic infarction)
Vasculitis: Primary CNS vasculitis or secondary (SLE, PAN, giant cell)
STROKE SYNDROMES BY VASCULAR TERRITORY - POSTERIOR CIRCULATION
Vertebrobasilar System
The posterior circulation (vertebral arteries → basilar artery → PCA) supplies the brainstem, cerebellum, thalami, and occipital lobes.
Characteristic features: Often crossed deficits (ipsilateral cranial nerve + contralateral body), ataxia, vertigo, dysarthria, dysphagia - distinguishing from anterior circulation.
Wallenberg Syndrome (Lateral Medullary / PICA Infarct) - "Must Know"
Artery: Posterior inferior cerebellar artery (PICA) or vertebral artery
Signs:
- Ipsilateral: Face pain/numbness (CN V), Horner's syndrome (ptosis, miosis, anhidrosis), limb ataxia, dysphonia/dysphagia (CN IX/X), loss of taste
- Contralateral: Pain + temperature loss (body) - spinothalamic
- Preserved: Motor strength, vibration/proprioception, consciousness
This is a pure sensory-ataxic syndrome with NO hemiplegia - a classic board question.
Basilar Artery Occlusion - A Neurological Emergency
Complete basilar occlusion → "locked-in syndrome" or death. Partial occlusion produces a range of brainstem syndromes.
Features of basilar territory ischemia:
- Bilateral motor signs (quadriplegia)
- Bilateral cranial nerve palsies
- Altered consciousness (reticular formation)
- "Top of the basilar" syndrome: thalamic infarcts, peduncular hallucinations, memory loss, oculomotor palsies, cortical blindness
Locked-in syndrome: Complete pontine infarct → quadriplegia + anarthria, but preserved consciousness and vertical eye movements (superior colliculus spared). Communication via vertical eye movements / blinking.
Anterior Inferior Cerebellar Artery (AICA)
- Ipsilateral hearing loss + facial numbness + Horner's + ataxia
- Peripheral facial palsy (CN VII nucleus involvement)
- Contralateral body pain/temperature loss
IMAGING IN STROKE - RADIOLOGICAL APPROACH
Non-Contrast CT (NCCT) - First Line in All Acute Stroke
Why CT first?
- Widely available, fast, excellent for ruling out hemorrhage
- Cannot miss ICH before giving tPA
What to look for on NCCT in ischemic stroke:
| Finding | Significance | Timeframe |
|---|---|---|
| Hyperdense MCA sign | Thrombus in MCA | Within hours |
| Loss of gray-white differentiation | Early ischemia | 3-6 hours |
| Insular ribbon sign | MCA territory ischemia | 3-6 hours |
| Sulcal effacement | Cytotoxic edema | 6-24 hours |
| Established hypodensity | Completed infarct | 24+ hours |
ASPECTS Score (Alberta Stroke Program Early CT Score): 0-10 point scale scoring early ischemic changes in MCA territory. Score ≤6 predicts poor outcome with thrombolysis.
CT Angiography (CTA) and CT Perfusion (CTP)
- CTA: Identifies LVO (large vessel occlusion) - essential for thrombectomy candidacy
- CTP: Distinguishes ischemic core (CBF <30%, irreversible) from penumbra (CBV preserved, CBF reduced) - the "mismatch" justifies late-window thrombectomy (DAWN/DEFUSE-3 trials)
MRI - Gold Standard for Stroke Characterization
| Sequence | Purpose |
|---|---|
| DWI (Diffusion-Weighted Imaging) | Detects acute ischemia within minutes; bright signal = restricted diffusion |
| ADC map | Dark in acute ischemia (confirms restricted diffusion, not T2 shine-through) |
| FLAIR | Dark in hyperacute (<4.5h), bright when chronic; FLAIR-DWI mismatch = still in time window |
| GRE/SWI | Detects microbleeds, hemosiderin, old hemorrhage |
| MRA | Vessel imaging without contrast |
| PWI (Perfusion) | Identifies penumbra; PWI-DWI mismatch = salvageable tissue |
DWI-FLAIR Mismatch: If DWI positive (acute infarct) but FLAIR still dark → stroke likely <4.5 hours even without a known onset time → patient may be eligible for IV tPA ("wake-up stroke").
PART II: HEMORRHAGIC STROKE
INTRACEREBRAL HEMORRHAGE (ICH)
(Harrison's Ch. 439)
Definition: Spontaneous bleeding directly into brain parenchyma (not traumatic, not subarachnoid).
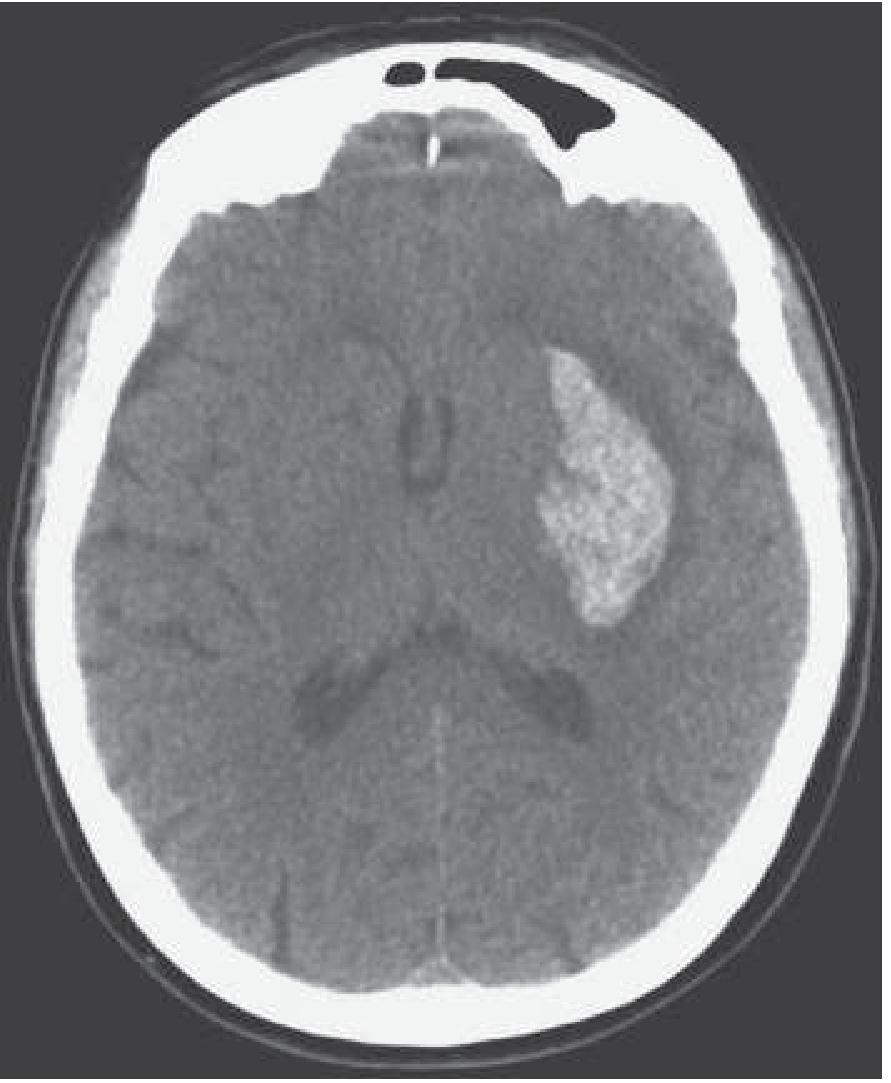
FIGURE 439-1 (Harrison's): Transaxial noncontrast CT scan showing a hyperintense (white) hematoma in the left putamen in a patient with right hemiparesis - classic hypertensive basal ganglia ICH.
Incidence: ~10% of all strokes. Higher mortality than ischemic stroke (30-day mortality ~40%).
LOCATION TELLS YOU THE CAUSE:
| Location | Most Likely Cause | Clinical Clue |
|---|---|---|
| Putamen / basal ganglia | Hypertension | Hemiplegia, gaze deviation |
| Thalamus | Hypertension | Sensory > motor, medial gaze palsy |
| Pons | Hypertension | Pinpoint pupils, quadriparesis, hyperthermia |
| Cerebellum | Hypertension | Ataxia, vomiting, no hemiparesis - SURGICAL EMERGENCY |
| Lobar (cortical/subcortical) | CAA (elderly) or AVM (young) | Depends on lobe; amyloid→ recurrent, multiple |
| Multiple simultaneous lobar | Cerebral amyloid angiopathy | Elderly, dementia, prior lobar bleeds |
Cerebral Amyloid Angiopathy (CAA):
- Amyloid-β deposition in cortical/leptomeningeal vessels
- Recurrent lobar hemorrhages in elderly
- MRI SWI/GRE: multiple cortical microbleeds ("blooming artifacts") - pathognomonic
- Associated with Alzheimer's disease pathology
- CAA-related inflammation: seizures, cognitive decline - responds to steroids
Pathophysiology of hematoma expansion:
- 30-40% of hematomas expand in the first 24 hours
- Expansion → worse outcomes
- "Spot sign" on CTA: extravasation of contrast within the hematoma = predictor of expansion
- INTERACT2 / ATACH2 trials: aggressive SBP lowering to <140 mmHg is safe and may improve functional outcome (though ATACH2 showed no mortality benefit and increased renal adverse events)
Clinical Presentation:
- Sudden onset headache + focal deficit + altered consciousness
- No "maximal at onset" rule: ICH often progresses over minutes-hours as hematoma expands
- Vomiting more common than ischemic stroke
- Significantly elevated BP (often >180/110)
Management of ICH (Harrison's):
- Airway: Aggressive airway management - deterioration is common and progressive
- Blood pressure: Target SBP <140 mmHg in patients with initial SBP 150-220 mmHg (AHA/ASA guidelines) - use IV labetalol, nicardipine
- Reverse anticoagulation:
- Warfarin: Vitamin K + 4-factor PCC (idarucizumab if dabigatran)
- DOACs: specific reversal agents (andexanet alfa for factor Xa inhibitors)
- ICP management: Elevate head of bed 30°, avoid hyperglycemia and fever, consider hypertonic saline or mannitol for herniation
- Seizure prophylaxis: Not routinely recommended unless clinical seizures
- Surgery:
- Cerebellar hematoma >3 cm or with brainstem compression → emergent surgical evacuation
- Supratentorial ICH: STICH trials showed no benefit of early surgery except possibly superficial lobar ICH
- Minimally invasive surgery (MISTIE III): reduced hematoma but no functional benefit in landmark trial
Prognosis - ICH Score:
| Factor | Points |
|---|---|
| GCS 3-4 | 2 |
| GCS 5-12 | 1 |
| Age ≥80 | 1 |
| Volume ≥30 mL | 1 |
| IVH present | 1 |
| Infratentorial origin | 1 |
Score 0 = 0% 30-day mortality; Score ≥5 = ~97% 30-day mortality.
SUBARACHNOID HEMORRHAGE (SAH)
(Harrison's Ch. 440)
Definition: Bleeding into the subarachnoid space (between arachnoid and pia mater).
Causes:
- Aneurysmal SAH (~85%): Rupture of saccular ("berry") aneurysm
- Perimesencephalic SAH (~10%): Benign, venous/capillary origin, normal angiography
- Other (5%): AVM, dural fistula, cocaine, mycotic aneurysm
Epidemiology (Harrison's):
- Prevalence of unruptured aneurysms: ~2% of adults
- Incidence of SAH: 6-11/100,000/year (25,000-30,000 cases/year in US)
- Overall mortality: ~35% (one-third die before hospitalization)
- Rebleeding: 20% in first 2 weeks, 30% in first month, ~3%/year thereafter
Aneurysm locations (common):
- Anterior communicating artery (ACoA) - most common, associated with abulia/mutism
- Posterior communicating artery (PCoA) - presents with CN III palsy
- MCA bifurcation - hematoma in sylvian fissure
- Basilar tip - oculomotor palsies, coma
- PICA origin - posterior fossa, may mimic Wallenberg
Clinical Presentation - The "Thunderclap Headache":
- "Worst headache of my life" - sudden, severe, peaks within seconds
- Nausea, vomiting, photophobia, meningismus (stiff neck)
- Loss of consciousness at onset (~50%)
- Sentinel headache: Days to weeks prior in ~50% - WARNING BLEED, often missed
- Focal signs if: hematoma (lobar, sylvian), vasospasm, or specific aneurysm location
- CN III palsy = posterior communicating artery aneurysm until proven otherwise (fixed dilated pupil)
Diagnosis:
- Non-contrast CT: Hyperdense blood in subarachnoid cisterns (basal cisterns, sylvian fissures, interhemispheric fissure). Sensitivity: 95-98% within first 12 hours, falls to ~85% by 24h
- Lumbar puncture: If CT negative + high suspicion → xanthochromia (yellow CSF from oxyhemoglobin/bilirubin breakdown) develops after 2-4h and persists 2 weeks
- CT Angiography (CTA): First line to identify aneurysm
- Digital Subtraction Angiography (DSA): Gold standard - also therapeutic
Hunt and Hess Classification (clinical grade):
| Grade | Description | Mortality |
|---|---|---|
| 1 | Asymptomatic / mild headache | ~1-5% |
| 2 | Moderate-severe headache, nuchal rigidity, no deficit | ~5-15% |
| 3 | Drowsy, minimal confusion, mild focal deficit | ~15-30% |
| 4 | Stupor, moderate-severe hemiparesis | ~50-80% |
| 5 | Deep coma, decerebrate rigidity | ~~90% |
WFNS Grade (World Federation of Neurological Surgeons) uses GCS + motor deficit.
Fisher Scale (CT-based - predicts vasospasm):
| Grade | CT Findings | Vasospasm Risk |
|---|---|---|
| 1 | No blood | Low |
| 2 | Diffuse thin SAH | Low-moderate |
| 3 | Thick cisternal clot >1mm | HIGH |
| 4 | Intracerebral or intraventricular hemorrhage | Moderate-high |
Complications of SAH:
- Rebleeding - highest risk in first 24-48h; prevention = early aneurysm securing (clipping or coiling)
- Cerebral vasospasm - peaks day 4-14, causes delayed cerebral ischemia (DCI)
- Diagnosis: TCD (VMCA >120 cm/s = vasospasm; >200 = severe), CTA, DSA
- Treatment: Nimodipine (60mg q4h for 21 days) - reduces DCI and improves outcomes (oral only; IV nimodipine NOT approved - causes severe hypotension)
- "Triple H therapy" (hypertension, hypervolemia, hemodilution) is used for symptomatic vasospasm
- Intra-arterial verapamil/nicardipine + balloon angioplasty for refractory vasospasm
- Hydrocephalus - communicating (impaired CSF resorption) or obstructive → EVD placement
- Hyponatremia - cerebral salt wasting (SIADH-like but with volume depletion → treat with fluid + salt, NOT fluid restriction)
- Cardiac complications: "Neurogenic stunned myocardium" - ECG changes (QTc prolongation, T-wave inversion, ST changes), troponin elevation, wall motion abnormalities → distinguish from ACS
Management of SAH:
- Emergency stabilization: ICU, BP control (avoid SBP >160 before aneurysm secured, avoid hypotension)
- Secure the aneurysm:
- Endovascular coiling (preferred in ISAT trial - better outcomes, same rebleed risk)
- Surgical clipping (preferred for: MCA aneurysms with hematoma, young patients, complex aneurysm anatomy)
- Nimodipine 60mg q4h × 21 days
- Seizure management: Treat clinical seizures; prophylactic AED controversial
- ICP management: EVD for hydrocephalus
- Prevent DCI: Maintain euvolemia (avoid hypovolemia), induced hypertension if vasospasm develops
PART III: TIA - TRANSIENT ISCHEMIC ATTACK
Definition (modern): Transient neurologic dysfunction from focal brain/spinal/retinal ischemia WITHOUT acute infarction on imaging.
Key concept: TIA is a medical emergency. Risk of stroke after TIA is highest in the first 48 hours.
ABCD² Score (risk stratification):
| Factor | Points |
|---|---|
| Age ≥60 years | 1 |
| BP ≥140/90 mmHg | 1 |
| Clinical features: unilateral weakness | 2 |
| Clinical features: speech disturbance without weakness | 1 |
| Duration ≥60 min | 2 |
| Duration 10-59 min | 1 |
| Diabetes | 1 |
Score 6-7: High risk (~8% 2-day stroke risk) → urgent inpatient workup.
Tissue-based definition implications:
- Amaurosis fugax (monocular blindness): TIA of retinal artery
- If DWI shows infarct despite resolution of symptoms = minor ischemic stroke, NOT TIA
Dual antiplatelet therapy after TIA/minor stroke (Harrison's):
The CHANCE and POINT trials showed that dual antiplatelet therapy (aspirin + clopidogrel) for 21 days after TIA/minor stroke significantly reduces early recurrent stroke without increasing major bleeding.
PART IV: ACUTE MANAGEMENT OF ISCHEMIC STROKE
(Harrison's Ch. 438)
The Time-Critical Algorithm
"Time is Brain" - 1.9 million neurons lost per minute in a major stroke
Onset → ED Arrival → CT → tPA decision → CTA → Thrombectomy
<10 min <25 min <60 min <25 min <90 min from arrival
(door-to-needle)
IV Thrombolysis - Alteplase (tPA)
- Dose: 0.9 mg/kg IV (max 90mg), 10% as bolus, 90% over 60 min
- Time window: ≤4.5 hours from symptom onset (extended from 3h in ECASS-3)
- Tenecteplase (0.25 mg/kg IV single bolus) is now an alternative with similar efficacy and simpler administration
Absolute contraindications to IV tPA:
- CT showing hemorrhage or large established infarct
- Prior ICH ever
- Active internal bleeding (not menstruation)
- Ischemic stroke or serious head trauma in past 3 months
- BP >185/110 (must be controlled first)
- Platelets <100,000; INR >1.7; aPTT >40 (if on anticoagulants)
- Blood glucose <50 or >400 mg/dL
- Endocarditis
Blood pressure management before/after tPA:
- Must be ≤185/110 before tPA
- Maintain ≤180/105 for 24h after tPA
Endovascular Thrombectomy (EVT)
The landmark achievement of modern stroke neurology. Multiple RCTs (MR CLEAN, ESCAPE, SWIFT PRIME, DAWN, DEFUSE-3) established EVT as standard of care for LVO.
Indications (AHA/ASA guidelines):
- LVO confirmed on CTA (ICA, M1, or proximal M2 MCA; basilar; vertebral)
- NIHSS ≥6 (significant deficit)
- ASPECTS ≥6 (limited early ischemia)
- Early window (0-6h): Based on clinical/imaging criteria above
- Late window (6-24h): DAWN/DEFUSE-3 criteria - requires perfusion imaging showing core/penumbra mismatch
Technique: Mechanical thrombectomy via stent-retriever or aspiration catheter via femoral/radial access.
Antithrombotic Therapy (non-tPA)
- Aspirin 162-325mg within 24-48h (not within 24h if tPA given) - reduces early recurrence
- Early anticoagulation with heparin: NOT recommended routinely (increases bleeding without reducing recurrence)
- Dual antiplatelet (aspirin + clopidogrel) for 21 days in high-risk TIA/minor stroke (CHANCE, POINT trials)
Medical Support (Harrison's)
- Treat fever (antipyretics, cooling blanket)
- Treat hyperglycemia (target 140-180 mg/dL with insulin)
- Avoid hypotension (permissive hypertension up to 220/120 in non-tPA patients)
- DVT prophylaxis: pneumatic compression stockings (proven benefit), low-dose heparin (also safe)
- Swallowing assessment before oral intake
- Early physiotherapy, speech therapy, occupational therapy
PART V: SECONDARY STROKE PREVENTION
Antiplatelet Therapy (non-cardioembolic stroke)
- Aspirin 75-325mg/day
- Clopidogrel 75mg/day (slightly superior to aspirin in CAPRIE trial)
- Aspirin + dipyridamole ER (Aggrenox) - ESPS-2 trial
- Short-course aspirin + clopidogrel (21 days) for TIA/minor stroke
Anticoagulation (cardioembolic / AF)
- AF: DOACs preferred (apixaban, rivaroxaban, dabigatran, edoxaban) over warfarin
- Mechanical heart valves: Warfarin only (DOACs contraindicated - RE-ALIGN trial)
- Timing after stroke: For large cardioembolic infarcts, delay anticoagulation 1-2 weeks (risk of hemorrhagic transformation)
Carotid Revascularization
- Symptomatic ICA stenosis 50-99%: CEA (carotid endarterectomy) within 2 weeks - absolute benefit greatest within 2 weeks
- NASCET trial: CEA reduces 2-year stroke risk from 26% to 9% in 70-99% stenosis
- CAS (carotid artery stenting): Alternative in high surgical risk patients
Risk Factor Modification
- Hypertension: Target <130/80 (ACEi + thiazide diuretic combination - PROGRESS trial)
- Statins: High-intensity statin for all ischemic stroke/TIA regardless of LDL (SPARCL trial - atorvastatin 80mg reduced stroke recurrence)
- Diabetes: Tight glycemic control
- Smoking cessation, weight loss, physical activity
- AF management: Rate/rhythm control + anticoagulation
IMAGING SUMMARY TABLE
| Stroke Type | CT Findings | MRI DWI | Key Imaging Feature |
|---|---|---|---|
| Acute ischemic (0-6h) | May be normal / hyperdense MCA sign | Bright (restricted diffusion) | DWI bright, ADC dark |
| Ischemic (>24h) | Hypodense area | FLAIR bright | Gyral swelling |
| Lacunar | Usually normal or small hypodensity | Small bright focus in deep structures | Dots in internal capsule/pons |
| ICH | Hyperdense (white) hematoma | Variable - complex signal | Homogeneous hyperattenuation on CT |
| SAH | Hyperdense blood in cisterns/fissures | FLAIR very sensitive | Basal cistern blood |
| Chronic ICH | Hypodense (old blood) | Hemosiderin on SWI/GRE (blooming) | "Blooming" on susceptibility MRI |
🧠 MCQ EVALUATION - 15 QUESTIONS
Q1.
A 68-year-old hypertensive man develops sudden-onset right hemiplegia, global aphasia, and left gaze deviation. NCCT shows no hemorrhage. What is the most likely diagnosis?
A. Right MCA territory infarction
B. Left MCA territory infarction ✅
C. Left ACA territory infarction
D. Basilar artery occlusion
Explanation: Global aphasia (dominant hemisphere = left) + right hemiplegia + gaze deviation TOWARD the lesion (left) = left MCA syndrome. Gaze deviation is ipsilateral to the hemispheric lesion.
Q2.
A 45-year-old woman presents with sudden onset of "the worst headache of my life" followed by vomiting and neck stiffness. CT is negative. Next best step?
A. MRI brain with DWI
B. IV tPA immediately
C. Lumbar puncture ✅
D. Start nimodipine empirically
Explanation: CT has ~95-98% sensitivity for SAH in first 12h. A negative CT does not exclude SAH - LP is mandatory to check for xanthochromia. Nimodipine should be started once SAH is confirmed.
Q3.
A 72-year-old diabetic woman presents with pure hemisensory loss on the right side without motor deficits, aphasia, or visual field defect. MRI shows a 6mm DWI-positive lesion in the left thalamus. Most likely diagnosis?
A. Cardioembolic stroke
B. Large vessel atherothrombotic stroke
C. Lacunar (small vessel) stroke ✅
D. Cortical branch MCA infarction
Explanation: Pure sensory stroke is one of the classic lacunar syndromes. The VPL nucleus of the thalamus is supplied by small penetrating arteries. No cortical signs = lacunar.
Q4.
On CTP imaging for acute stroke, the "ischemic penumbra" is best defined as:
A. Area of CBF = 0 with cell death
B. Area of CBF reduction with CBV preserved - reversibly dysfunctional tissue ✅
C. Region with FLAIR positivity
D. Zone of luxury perfusion post-reperfusion
Explanation: Harrison's defines the penumbra as ischemic but reversibly dysfunctional tissue. It has reduced CBF but preserved CBV (compensatory vasodilation). This is the tissue target of reperfusion therapy.
Q5.
A 55-year-old man presents with acute stroke 4 hours after onset. BP is 200/110 mmHg. You plan IV alteplase. What is the correct BP management?
A. Do not lower BP; proceed with tPA immediately
B. Lower BP to <185/110 before tPA, then maintain <180/105 for 24h ✅
C. Lower BP to <140/90 aggressively before proceeding
D. BP >180 is an absolute contraindication to tPA regardless
Explanation: Harrison's: BP must be ≤185/110 before tPA administration. After tPA, maintain ≤180/105 for 24h. Aggressive BP lowering in ischemic stroke can worsen penumbral ischemia.
Q6.
Which of the following is the MOST IMPORTANT early complication to prevent in aneurysmal SAH?
A. Cerebral vasospasm
B. Hyponatremia
C. Rebleeding ✅
D. Hydrocephalus
Explanation: Rebleeding is the most catastrophic early complication (20% in 2 weeks, highest in first 24-48h) and is prevented by urgently securing the aneurysm. Vasospasm is the main cause of delayed morbidity (days 4-14).
Q7.
A 78-year-old with recurrent lobar intracerebral hemorrhages is most likely to have which underlying condition?
A. Hypertension
B. Arteriovenous malformation
C. Cerebral amyloid angiopathy ✅
D. Warfarin toxicity
Explanation: CAA causes recurrent LOBAR hemorrhages in elderly patients. Hypertension causes deep (basal ganglia, pons, thalamus) hemorrhages. MRI SWI shows multiple cortical microbleeds in CAA.
Q8.
Nimodipine is used in SAH for which specific purpose?
A. To reduce intracranial pressure
B. To prevent rebleeding
C. To reduce the risk of delayed cerebral ischemia from vasospasm ✅
D. As a neuroprotective agent to reduce initial hemorrhage
Explanation: Nimodipine 60mg orally q4h × 21 days reduces DCI (not necessarily angiographic vasospasm) and improves neurologic outcomes. It does NOT prevent vasospasm itself but protects against ischemic injury. IV nimodipine causes dangerous hypotension and is not used.
Q9.
A patient with right-sided Horner's syndrome, right facial pain/numbness, right limb ataxia, and left body pain/temperature loss most likely has an infarct in:
A. Right MCA territory
B. Right pontine territory
C. Right lateral medulla (Wallenberg syndrome) ✅
D. Right thalamus
Explanation: Lateral medullary (Wallenberg) syndrome: ipsilateral face (CN V), Horner's, ataxia, IX/X palsies + contralateral body spinothalamic loss. The crossing of spinothalamic fibers in the cord explains the dissociated sensory loss. Motor strength is preserved.
Q10.
Which trial established dual antiplatelet therapy (aspirin + clopidogrel) for 21 days as beneficial after TIA or minor ischemic stroke?
A. CAPRIE trial
B. CHANCE trial ✅
C. NASCET trial
D. SPARCL trial
Explanation: CHANCE (China) and POINT (US/Canada) trials both showed dual antiplatelet for 21-90 days (high-risk TIA or minor stroke) significantly reduces early stroke recurrence without increasing major bleeding. CAPRIE = clopidogrel vs aspirin. NASCET = CEA for carotid stenosis. SPARCL = atorvastatin 80mg for stroke prevention.
Q11.
A patient's ICH Score is calculated as: GCS 7, age 75, hematoma volume 45 mL, no IVH, supratentorial location. What is the score and estimated 30-day mortality?
A. Score 2, ~26% mortality
B. Score 3, ~72% mortality ✅
C. Score 4, ~97% mortality
D. Score 1, ~13% mortality
Explanation: GCS 5-12 = 1 point; age ≥80 = 0; volume ≥30 mL = 1 point; no IVH = 0; supratentorial = 0. Total = 2 points → ~26% mortality. Wait - let me recalculate: GCS 7 (5-12 range) = 1pt; age 75 (<80) = 0pt; volume 45mL (≥30) = 1pt; no IVH = 0; supratentorial = 0. Total = 2 points, ~26% mortality. Answer A is correct. This question tests careful point calculation.
Q12.
On MRI, the DWI-FLAIR mismatch concept is used to:
A. Identify hemorrhagic transformation
B. Distinguish acute vs subacute infarction for late-window thrombolysis ✅
C. Diagnose cerebral venous thrombosis
D. Quantify the ischemic penumbra on MR perfusion
Explanation: DWI positivity = acute infarct. FLAIR negativity = stroke <4.5 hours. If DWI bright + FLAIR still dark = patient is likely within the treatment window, even in wake-up strokes where onset time is unknown.
Q13.
Which artery, when occluded, classically produces a crossed deficit with ipsilateral CN III palsy and contralateral hemiplegia?
A. Posterior inferior cerebellar artery
B. Anterior inferior cerebellar artery
C. Posterior cerebral artery (P1 segment, Weber's syndrome) ✅
D. Basilar artery perforators - AICA
Explanation: Weber's syndrome = ipsilateral CN III palsy (oculomotor nerve at cerebral peduncle level) + contralateral hemiplegia (corticospinal tract in peduncle). This is a P1 PCA / posterior penetrating artery syndrome affecting the cerebral peduncle.
Q14.
In a patient with AF who has a large cardioembolic ischemic stroke, when is it generally safe to initiate anticoagulation?
A. Immediately (within 24 hours) to prevent early recurrence
B. After 1-2 weeks, once the risk of hemorrhagic transformation has decreased ✅
C. Never - anticoagulation is contraindicated after large cardioembolic stroke
D. After 6 weeks regardless of infarct size
Explanation: Large cardioembolic infarcts carry high risk of hemorrhagic transformation, especially in the first 1-2 weeks. Guidelines recommend delaying anticoagulation 1-2 weeks for large infarcts (the "1-3-6-12 day rule" is sometimes used: TIA=day 1, small=day 3, medium=day 6, large=day 12).
Q15.
A patient with acute cerebellar ICH (4.5 cm hematoma with brainstem compression on CT) is obtunded. What is the priority intervention?
A. IV mannitol and observation
B. Emergent surgical evacuation ✅
C. Nimodipine and blood pressure control only
D. Start IV tPA to dissolve the hematoma
Explanation: Harrison's: Cerebellar hematoma >3 cm or causing brainstem compression is a surgical emergency. The posterior fossa has no room for expansion - brainstem herniation can occur rapidly. Emergent suboccipital craniectomy with hematoma evacuation is lifesaving. Supratentorial ICH generally does not benefit from surgery (STICH trials).
SUMMARY CARD FOR RAPID REVIEW
| Feature | Ischemic | ICH | SAH |
|---|---|---|---|
| Onset | Maximal at onset (embolic) / stuttering (thrombotic) | Progressive over minutes-hours | Thunderclap, instantaneous |
| Headache | Rare | Moderate | Severe "worst of life" |
| LOC | Less common | Progressive | Common at onset |
| CT | Normal early / hypodensity late | Hyperdense hematoma | Hyperdense cisterns/fissures |
| LP | Not needed | Not needed | Xanthochromia if CT negative |
| Key treatment | tPA / thrombectomy | BP control, reverse coag, surgery if cerebellar | Secure aneurysm, nimodipine |
| BP target acute | Permissive ≤220/120 (no tPA) | <140 mmHg SBP | Avoid hypotension; control hypertension after securing |
RECENT EVIDENCE UPDATE (2025-2026)
- PMID 40788598 (JAMA Neurol, 2025): Meta-analysis on intracranial hemorrhage after endovascular treatment with/without alteplase - IV alteplase before EVT does not significantly increase sICH risk in LVO patients
- PMID 40555310 (2025): Systematic review showing left atrial septal pouch detected on TEE is associated with cryptogenic stroke / ESUS - supports aggressive cardiac workup including TEE
- PMID 41614311 (JAHA, 2026): Small-vessel disease and stroke linked to occupational factors - emerging risk factor data
Primary sources: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapters 437, 438, 439, 440. Supplemented by Bradley & Daroff's Neurology in Clinical Practice and current PubMed literature (2025-2026).
This is a shared conversation. Sign in to Orris to start your own chat.