Ibd full explained acc to robbins text of pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have all the material needed for a complete, detailed, image-rich IBD explanation from Robbins. Let me compile the full answer.
Inflammatory Bowel Disease (IBD) - Robbins Pathology
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10e) and Robbins & Kumar Basic Pathology
Definition and Overview
Inflammatory bowel disease (IBD) is a chronic inflammatory condition triggered by the host immune response to intestinal microbes in genetically predisposed individuals. IBD encompasses two distinct entities:
- Crohn Disease (CD)
- Ulcerative Colitis (UC)
The distinction between them is based on the distribution of affected sites and the morphologic expression of disease at those sites.
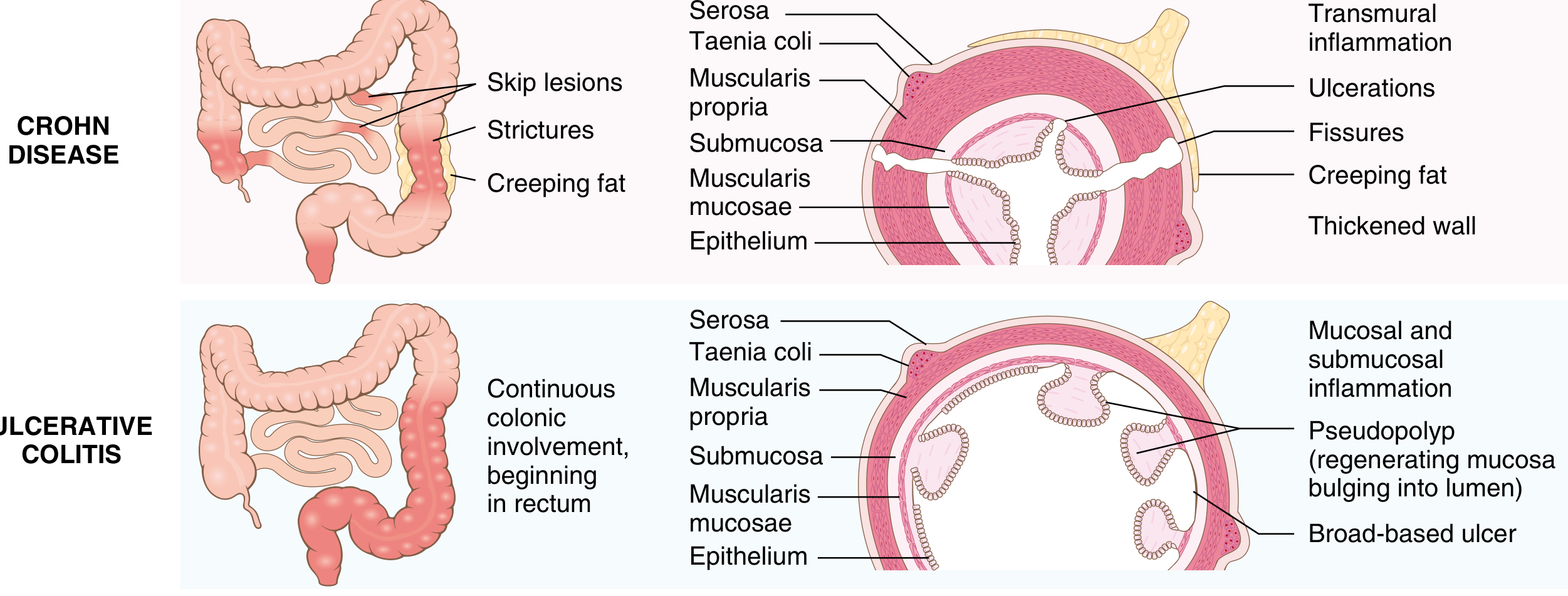
Comparison Table: Crohn Disease vs. Ulcerative Colitis
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Bowel region | Ileum ± colon (any GI segment) | Colon only |
| Rectal involvement | Sometimes | Always |
| Distribution | Skip lesions | Diffuse, continuous |
| Stricture | Yes (common) | Rare |
| Bowel wall | Thick (transmural fibrosis) | Thin/normal |
| Inflammation depth | Transmural | Mucosa and submucosa only |
| Ulcers | Deep, knife-like, serpentine | Superficial, broad-based |
| Pseudopolyps | Moderate | Marked |
| Lymphoid reaction | Marked | Moderate |
| Fibrosis | Marked | Mild to none |
| Serositis | Marked | Mild to none |
| Granulomas | Yes (~35%) | No |
| Fistulas/sinuses | Yes | No |
| Perianal fistula | Yes (in colonic disease) | No |
| Fat/vitamin malabsorption | Yes | No |
| Malignant potential | Yes (colonic involvement) | Yes |
| Recurrence after surgery | Common | No (colectomy is curative) |
| Toxic megacolon | No | Yes |
| p-ANCA | ~10% | ~75% |
Epidemiology
- Both diseases most often present in adolescents and young adults (teens to early 20s), but can occur at any age.
- IBD is more prevalent in North America, northern Europe, and Australia; incidence is rising in Africa, South America, and Asia.
- In the United States, it is 3-5x more common among Ashkenazi Jewish people than the general population.
- Hygiene hypothesis: reduced enteric infections in early childhood (due to improved hygiene) leads to inadequate development of regulatory mucosal immune responses, allowing luminal microbes to trigger persistent inflammation in susceptible hosts. Other proposed factors include preservatives and processed food additives causing low-grade mucosal damage.
- Monozygotic twin concordance: ~50% in Crohn disease vs ~20% in ulcerative colitis - indicating genetic factors are more dominant in Crohn disease.
Pathogenesis
IBD results from a combination of genetic susceptibility + abnormal host-microbe interactions + epithelial dysfunction + aberrant mucosal immunity.
1. Genetic Factors
- Over 200 IBD-associated risk alleles identified by GWAS, but these account for less than 20% of disease risk in Crohn disease, and even less in UC.
- NOD2 (nucleotide oligomerization binding domain 2) is the most strongly Crohn-associated gene in European populations. NOD2 encodes an intracellular sensor of muramyl dipeptide (a bacterial cell wall peptidoglycan component) and activates NF-κB. Disease-associated NOD2 variants are ineffective at defending against intestinal bacteria, allowing them to penetrate the epithelium and trigger chronic inflammation. However:
- The three major NOD2 risk alleles are present in only ~30% of Crohn patients
- They are uncommon in patients of African and Asian descent
- Disease develops in <10% of carriers
- Multiple variants in autophagy-related genes (autophagosome pathway) are also associated - like NOD2, these involve host responses to intracellular bacteria. These associations are NOT seen in UC.
2. Abnormal Mucosal Immune Responses
- Microbial antigens are presented to CD4+ helper T cells, which differentiate into Th1 and Th17 cells (driven by IL-12 and IL-23).
- These cells activate macrophages, recruit neutrophils, and release pro-inflammatory cytokines (TNF, IFN-γ, IL-17).
- In Crohn disease: predominantly a Th1/Th17-mediated response.
- In ulcerative colitis: mucosal production of the Th2-derived cytokine IL-13 is increased.
- Defects in regulatory T cells (especially IL-10-producing subsets) that normally dampen inflammation may contribute. Rare mutations in IL-10 or IL-10 receptor genes cause severe early-onset colitis.
- Anti-TNF antibodies (infliximab, adalimumab) are effective in both diseases, confirming a shared inflammatory mechanism.
3. Defects in Intestinal Epithelial Barrier
- Defective epithelial barrier function allows luminal microbes to gain access to the lamina propria.
- This is exacerbated by ongoing inflammation, creating a vicious cycle.
- Abnormalities in Paneth cell and goblet cell function are implicated - both involved in mucosal defense.
4. Altered Intestinal Microbiota
- The composition of gut microbiota (microbiome) is altered in IBD patients.
- Luminal microbiota play an important role in triggering and sustaining mucosal inflammation in genetically predisposed individuals.
CROHN DISEASE - Morphology
Site Distribution
- Can involve any area of the GI tract from mouth to anus.
- Most commonly: terminal ileum, ileocecal valve, and cecum.
- Small intestine only: ~40% of cases.
- Small intestine + colon: ~30%.
- Colon only: ~30% (hardest to distinguish from UC when pancolitis is present).
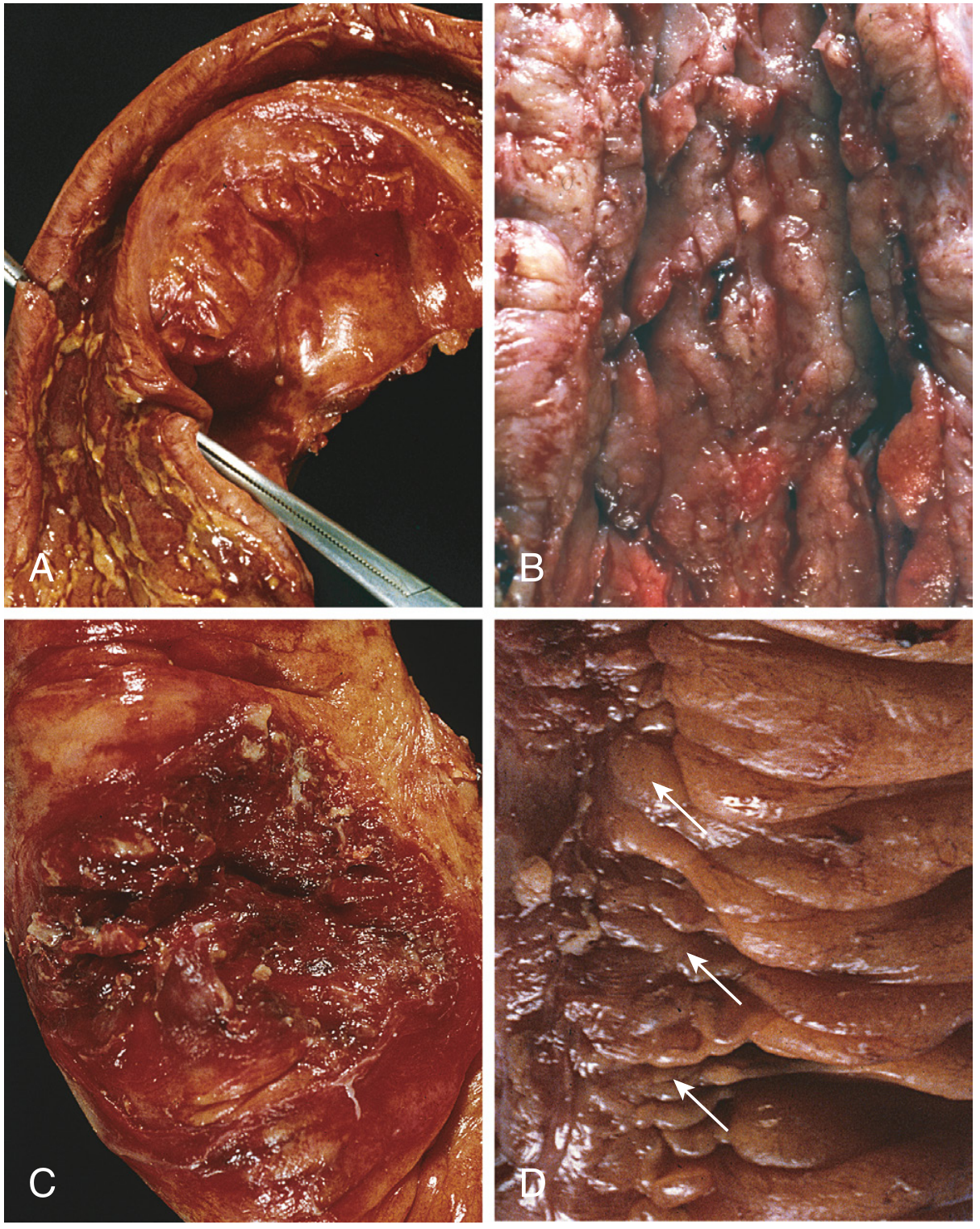
Gross (Macroscopic) Features
- Skip lesions: multiple separate, sharply delineated areas of disease with normal intervening bowel - pathognomonic feature.
- Earliest lesion: aphthous ulcer - small superficial erosion.
- Ulcers progress and coalesce into elongated, serpentine ulcers oriented along the long axis of the bowel.
- Ulceration with sparing of adjacent mucosa creates a cobblestone appearance.
- Fissures: deep clefts that may extend into mesenteric adipose tissue, creating peritoneal abscesses and perforation sites, or forming fistula tracts (enteroenteric, enterovesical, enterovaginal, perianal).
- Bowel wall thickening and rubbery consistency due to transmural edema, inflammation, submucosal fibrosis, and muscularis propria hypertrophy → stricture formation.
- Creeping fat: mesenteric adipose tissue wraps around the serosal surface due to transmural disease.
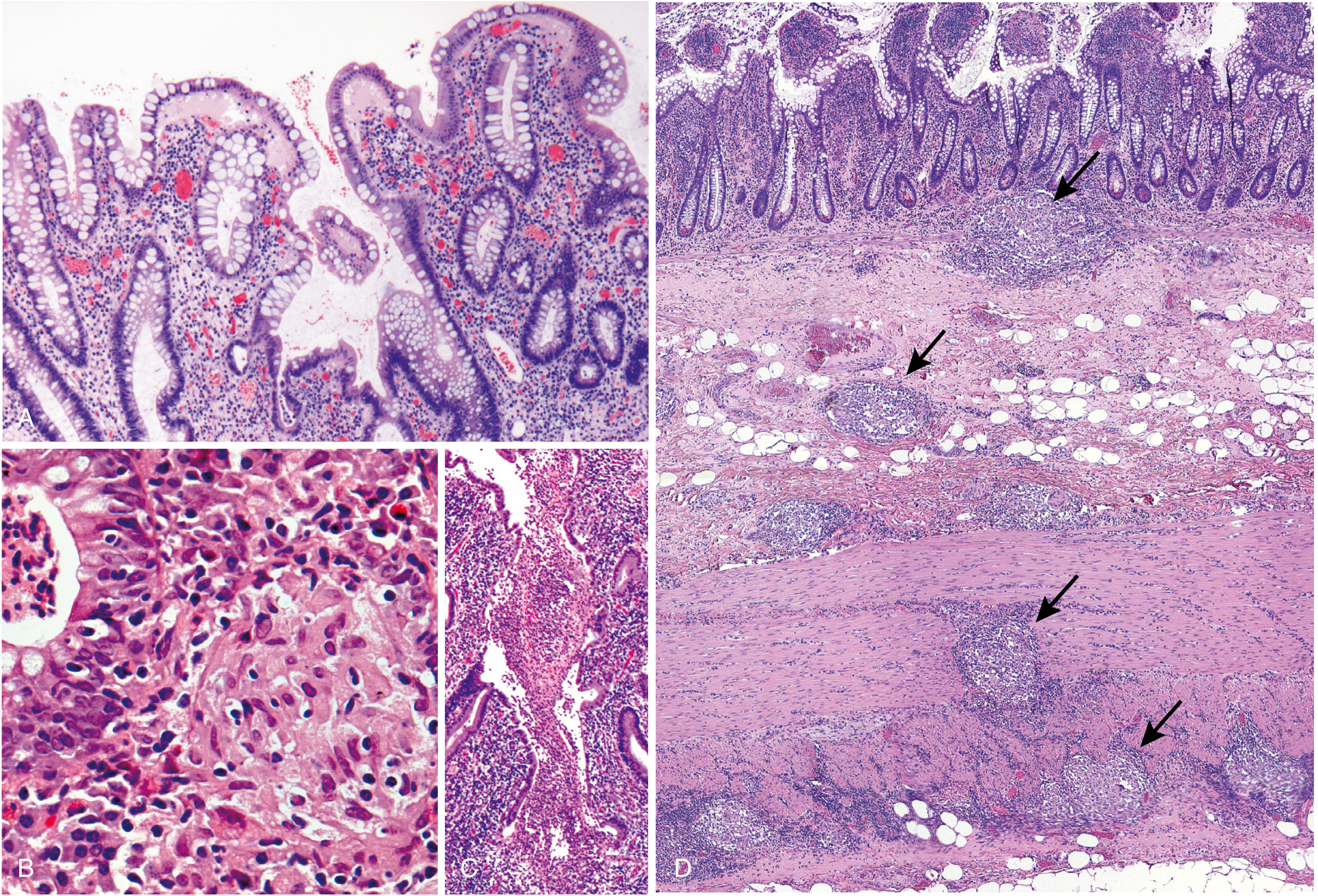
Microscopic Features
- Crypt abscesses: clusters of neutrophils within crypts, with crypt destruction.
- Transmural inflammation: lymphocytes, plasma cells, and macrophages throughout all layers - including serosa and mesentery.
- Noncaseating granulomas (present in ~35%): clusters of epithelioid macrophages with giant cells, WITHOUT caseation necrosis. They can appear in all layers - mucosa, submucosa, muscularis propria, and even regional lymph nodes.
- Crypt distortion and disorganization: from repeated cycles of crypt destruction and regeneration - crypts take on bizarre branching shapes and abnormal orientations.
- Patchy inflammation even in areas of apparent gross involvement.
- Abrupt transition between ulcerated and adjacent normal mucosa.
Clinical Features of Crohn Disease
- Intermittent attacks of crampy, non-bloody diarrhea (or bloody if colon involved), fever, and abdominal pain - in contrast to UC.
- Malabsorption: vitamin B12, fat-soluble vitamins, bile salts (due to ileal involvement) → steatorrhea, megaloblastic anemia.
- Complications: strictures causing bowel obstruction, fistulae (perianal, enterovesical, enterovaginal, enteroenteric), abscesses, perforation, nutritional deficiencies.
- Surgery does NOT cure Crohn disease - recurrence after surgery is common.
- Associated with smoking (smoking worsens Crohn disease but is protective in UC - paradox).
ULCERATIVE COLITIS - Morphology
Site Distribution
- Always involves the rectum and extends proximally in a continuous, uninterrupted fashion.
- Pancolitis: disease of the entire colon.
- Left-sided colitis / ulcerative proctitis / ulcerative proctosigmoiditis: limited distal disease.
- Small intestine is NOT affected (pure colonic disease).
- Exception: backwash ileitis - mild mucosal inflammation of the distal ileum in severe pancolitis.
- Cecal red spot: focal appendiceal or cecal inflammation in left-sided disease - does NOT represent a true skip lesion.
Gross Features
- Colonic mucosa ranges from slightly red and granular (early/mild) to extensive, broad-based ulcers (severe).
- Sharp, abrupt transition between diseased and uninvolved colon.
- Ulcers aligned along the long axis of the colon but do NOT form serpentine patterns.
- Pseudopolyps (inflammatory polyps): isolated islands of regenerating mucosa bulge into the lumen due to surrounding ulceration - a hallmark of UC.
- Mucosal bridges: tips of pseudopolyps fuse to create bridges across the lumen.
- Chronic disease → mucosal atrophy with smooth surface lacking normal folds.
- Colon wall is NOT thickened (not transmural), serosal surface is normal, strictures do NOT occur.
Microscopic Features
- Inflammation limited to the mucosa and submucosa - this is the single most important distinguishing feature from Crohn disease.
- Crypt abscesses and crypt destruction.
- Crypt distortion and disorganization (architectural changes from chronicity).
- Pseudopyloric metaplasia in the colon.
- NO granulomas in UC (their presence suggests Crohn disease).
- Active disease: abundant neutrophilic infiltrate, crypt abscesses.
- Quiescent disease: mucosal atrophy with fewer glands; histology may revert to near-normal after prolonged remission.
Clinical Features of UC
- Relapsing and remitting course.
- Bloody diarrhea with stringy mucoid material, lower abdominal crampy pain temporarily relieved by defecation.
-
50% of patients have clinically mild disease; almost all experience at least one relapse within 10 years.
- Toxic megacolon: acute colonic dilatation >6 cm with systemic toxicity - a life-threatening complication exclusive to UC (not Crohn); may lead to perforation.
- Initial onset of symptoms may be associated with smoking cessation (opposite of Crohn disease).
- Colectomy is curative for intestinal disease - unlike Crohn, disease does not recur after removal of the colon.
- Historically, up to 30% needed colectomy within 3 years; this has fallen sharply due to biologic agents.
- Extraintestinal manifestations may persist even after colectomy.
Indeterminate Colitis
- In ~10% of IBD patients, it is not possible to distinguish Crohn disease from UC.
- These cases have continuous colonic disease (like UC) but features suggesting Crohn (patchy histologic disease, family history of Crohn, perianal lesions).
- Fortunately, overlap in medical management allows treatment without a definitive diagnosis.
Extraintestinal Manifestations (Both Diseases)
- Joints: migratory polyarthritis, sacroiliitis, ankylosing spondylitis
- Eyes: uveitis, episcleritis
- Skin: erythema nodosum, pyoderma gangrenosum
- Liver/biliary: Primary sclerosing cholangitis (PSC) - markedly increased in UC (~5% of UC patients); conversely, the majority of PSC patients have UC.
- Oral: aphthous ulcers (more common in Crohn)
Colitis-Associated Neoplasia (Cancer Risk)
One of the most serious long-term complications of both diseases is the development of colorectal adenocarcinoma. Risk factors:
- Duration of disease: risk increases beginning 8-10 years after disease onset.
- Extent of involvement: pancolitis carries greater risk than partial colonic involvement.
- Degree of inflammation: greater frequency and severity of active neutrophilic inflammation increases carcinogenic risk (inflammation enables carcinogenesis).
- PSC co-existence: patients with both UC and PSC are at markedly greater risk - surveillance colonoscopy is initiated at the time of PSC diagnosis, not after 8 years.
Surveillance: Patients are enrolled in colonoscopic surveillance programs approximately 8 years after IBD diagnosis, requiring regular, extensive mucosal biopsies. In many cases, dysplasia occurs in flat mucosa that appears macroscopically normal - hence, advanced endoscopic imaging is being developed for early detection.
- In UC: cancer risk is confined to the colon.
- In Crohn disease: risk of both colorectal AND small intestinal adenocarcinoma.
Summary of Key Robbins Points
| Topic | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Location | Any GI segment, terminal ileum most common | Rectum + colon only, always rectum |
| Pattern | Skip lesions | Continuous |
| Depth | Transmural | Mucosal/submucosal only |
| Hallmark micro feature | Noncaseating granulomas (35%) | No granulomas |
| Key gross finding | Cobblestone mucosa, creeping fat, fistulae | Pseudopolyps, broad-based ulcers |
| Serology | ASCA positive, p-ANCA ~10% | p-ANCA ~75% |
| Cancer risk | Colorectal + small bowel | Colorectal only |
| Surgery | NOT curative, recurrence common | Curative (colectomy) |
| Smoking effect | Worsens disease | Cessation triggers disease |
| Unique complication | Fistulae, malabsorption, abscesses | Toxic megacolon |
- Robbins, Cotran & Kumar: Pathologic Basis of Disease, pp. 744-749
- Robbins & Kumar: Basic Pathology, pp. 577-582
This is a shared conversation. Sign in to Orris to start your own chat.