Diagnosis and Treatment for herper
Reading File
Finding Sources
Searching PubMed
herpes simplex virus diagnosis treatment
Searching Images
herpes simplex lesions clinical presentation
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is a thorough clinical overview:
Herpes Simplex Virus (HSV) — Diagnosis & Treatment
Overview
Herpes simplex virus infection is a lifelong viral infection caused by HSV-1 or HSV-2. Transmission occurs via contact with infected secretions through breaks in skin or intact mucous membranes. The virus ascends sensory nerves to dorsal root ganglia, where it establishes latency and may reactivate periodically. Incubation period is typically 4 days (range 2–12 days).
- HSV-1: predominantly orolabial ("cold sores"), but increasingly responsible for genital infections
- HSV-2: predominantly genital; higher recurrence rate than HSV-1
Clinical Presentation
Primary Infection
- Cluster of small erythematous painful vesicles that rapidly ulcerate
- Locations: external genitalia, perineum, buttocks, vagina, rectum, oropharynx (lips/perioral)
- Systemic symptoms: fever, malaise, headache, tender regional lymphadenopathy
- Dysuria common (genital involvement)
- Untreated primary infection resolves spontaneously in 2–4 weeks
Recurrent Infection
- Less severe and shorter duration than primary
- Often preceded by prodromal symptoms: itching, burning, paresthesias
- Triggered by: acute illness, immunosuppression, psychological stress, menses
- Recurrences become less frequent over time
- Asymptomatic viral shedding occurs even without visible lesions
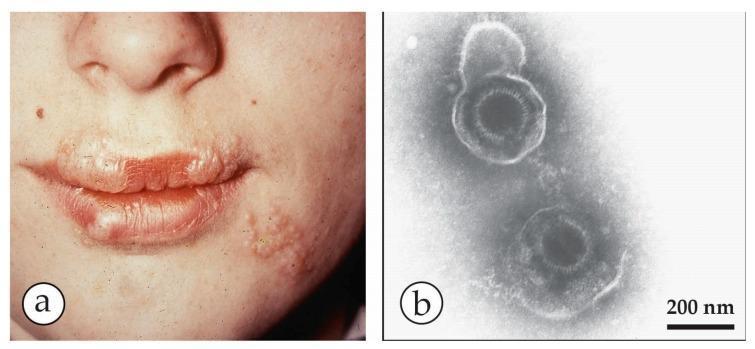
Clinical Images
(a) HSV-1 perioral "cold sores" — clustered vesicles on erythematous base at the vermillion border:
(b) HSV-2 genital lesions on the penile shaft — grouped vesicles with ulceration:

Complications
| Complication | Notes |
|---|---|
| Meningoencephalitis | HSV most common cause of sporadic encephalitis; treat immediately with IV acyclovir |
| Transverse myelitis | |
| Hepatitis / Pneumonitis | |
| Disseminated infection | Especially in immunocompromised |
| Neonatal herpes | From vertical transmission at delivery; high morbidity/mortality |
| Ocular herpes | Corneal dendrites/ulcers; uveitis — treat with trifluridine eye drops |
| HIV facilitation | Ulcerating HSV increases HIV transmission/acquisition |
Diagnosis
Clinical Diagnosis
- Often made on the basis of characteristic vesicular lesions in a typical distribution
- Clinical diagnosis alone is insensitive and nonspecific — laboratory confirmation is preferred
Laboratory Tests (in order of preference)
| Test | Notes |
|---|---|
| HSV NAAT (PCR) | Test of choice — highest sensitivity and specificity; performed on lesion swab |
| Viral culture | Highly specific but less sensitive than PCR; useful for active lesions |
| Direct Fluorescent Antibody (DFA) | Available but less commonly used |
| HSV type-specific serology | Useful for screening/counseling; does not confirm active infection |
| Tzanck smear | Non-specific (detects multinucleated giant cells); not recommended as sole diagnostic test |
| Darkfield microscopy + syphilis serology | To differentiate from syphilitic chancre |
Key point: In the ED, test results are delayed. Treatment is typically started empirically based on clinical findings. — ROSEN's Emergency Medicine
Treatment
Antiviral Agents
Three first-line antivirals are considered equivalent in safety and efficacy:
- Acyclovir (oldest; requires more frequent dosing)
- Valacyclovir (prodrug of acyclovir; better oral bioavailability, less frequent dosing)
- Famciclovir (prodrug of penciclovir; similar efficacy)
All inhibit viral DNA polymerase after phosphorylation by the viral thymidine kinase.
Dosing Regimens (Fitzpatrick's Dermatology / Rosen's EM)
Genital Herpes — Primary Episode
(Duration: 7–10 days or until clinical resolution)
| Drug | Dose |
|---|---|
| Acyclovir | 400 mg PO TID or 200 mg PO 5×/day |
| Valacyclovir | 1 g PO BID |
| Famciclovir | 250 mg PO TID |
Genital Herpes — Recurrent Episodes
(Duration: 5 days)
| Drug | Dose |
|---|---|
| Acyclovir | 400 mg PO TID or 800 mg PO BID |
| Valacyclovir | 500 mg PO BID or 1 g PO once daily |
| Famciclovir | 125 mg PO BID |
Suppressive Therapy (for frequent recurrences ≥6/year)
| Drug | Dose |
|---|---|
| Acyclovir | 400 mg PO BID |
| Valacyclovir | 500 mg PO once daily |
| Famciclovir | 250 mg PO BID |
Orolabial Herpes (HSV-1 "Cold Sores")
- Valacyclovir 2 g PO BID × 1 day (episodic)
- Acyclovir 400 mg PO 5×/day × 5 days
- Topical: Docosanol 10% cream (OTC) — reduces healing by ~18 hours
- Topical acyclovir/penciclovir cream — not significantly effective; not recommended
Severe / Disseminated / Encephalitis
- IV Acyclovir 10–15 mg/kg every 8 hours is the treatment of choice
- Neonatal herpes: IV acyclovir 20 mg/kg per dose every 8 hours
Special Populations
| Situation | Recommendation |
|---|---|
| HIV-infected patients | Acyclovir 400 mg TID or Famciclovir 500 mg BID or Valacyclovir 1 g BID until lesions healed |
| Pregnancy | Neither acyclovir nor valacyclovir is associated with congenital malformations; IV acyclovir for life-threatening maternal HSV infection |
| Immunocompromised (acyclovir-resistant HSV) | Foscarnet IV (alternative for resistant strains) |
| Herpes keratitis | Trifluridine (Viroptic) eye drops |
When to Hospitalize
- Meningoencephalitis, hepatitis, pneumonitis, disseminated infection → parenteral acyclovir
- Neonatal herpes
Prevention & Counseling
- Condom use reduces but does not eliminate transmission risk
- Suppressive antiviral therapy in discordant couples (HSV+ / HSV−) reduces transmission by ~50%
- Patients should be counseled that transmission occurs even without visible lesions (asymptomatic shedding)
- Reactivation triggers to avoid: stress, illness, immunosuppression, UV exposure
Sources: ROSEN's Emergency Medicine, 10e (p. 1377); Fitzpatrick's Dermatology, 8e (p. 3060); Dermatology 2-Volume Set 5e; Goldman-Cecil Medicine
Diagnosis and treatment for type 2 diabetes
Reading File
Finding Sources
Searching PubMed
"type 2 diabetes mellitus" AND management
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
type 2 diabetes pathophysiology insulin resistance
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.