Coronary physiology of heart
Reading File
Finding Sources
Finding Sources
Searching PubMed
coronary physiology microcirculation
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the content needed for a comprehensive answer. Let me compile the full response.
Coronary Physiology of the Heart
1. Coronary Anatomy Overview
The heart receives its blood supply from two main coronary arteries - the left coronary artery (LCA) and the right coronary artery (RCA) - which are the first arterial branches of the aorta, each originating from its respective sinus of Valsalva.
-
Left main coronary artery (LMCA): Courses posterolateral to the pulmonary trunk ~1 cm before dividing into:
- Left anterior descending (LAD): Runs along the interventricular septum, supplying the LV free wall and septum
- Left circumflex (LCx): Travels in the atrioventricular groove, giving off obtuse marginal branches
-
Right coronary artery (RCA): Runs in the anterior AV sulcus, supplying the RV free wall; typically bifurcates into the posterior descending artery (PDA) and right posterolateral artery. In ~85% of people, the PDA arises from the RCA (right-dominant circulation).
-
AV nodal artery: Usually a branch of the RCA - its compromise causes arrhythmias or heart block.
2. Determinants of Coronary Blood Flow - Poiseuille's Law
Coronary blood flow is governed by Poiseuille's law: flow is directly proportional to the arterial-venous pressure gradient and inversely related to vascular resistance.
Flow ∝ Pressure gradient / Resistance, where Resistance ∝ 1/r⁴
Key implications:
- Small changes in vessel caliber cause disproportionately large changes in resistance (4th-power relationship with radius)
- Resting coronary blood flow: ~250 mL/min (1 mL/min/g), representing ~5% of cardiac output
- Vessel length remains essentially constant in the intact heart
- Blood viscosity (governed mainly by hemoglobin concentration) plays a minor role unless marked polycythemia or profound hemodilution is present
Coronary perfusion pressure (CPP) = Aortic diastolic pressure - LV end-diastolic pressure (coronary venous pressure is negligible)
3. Phasic Nature of Coronary Blood Flow
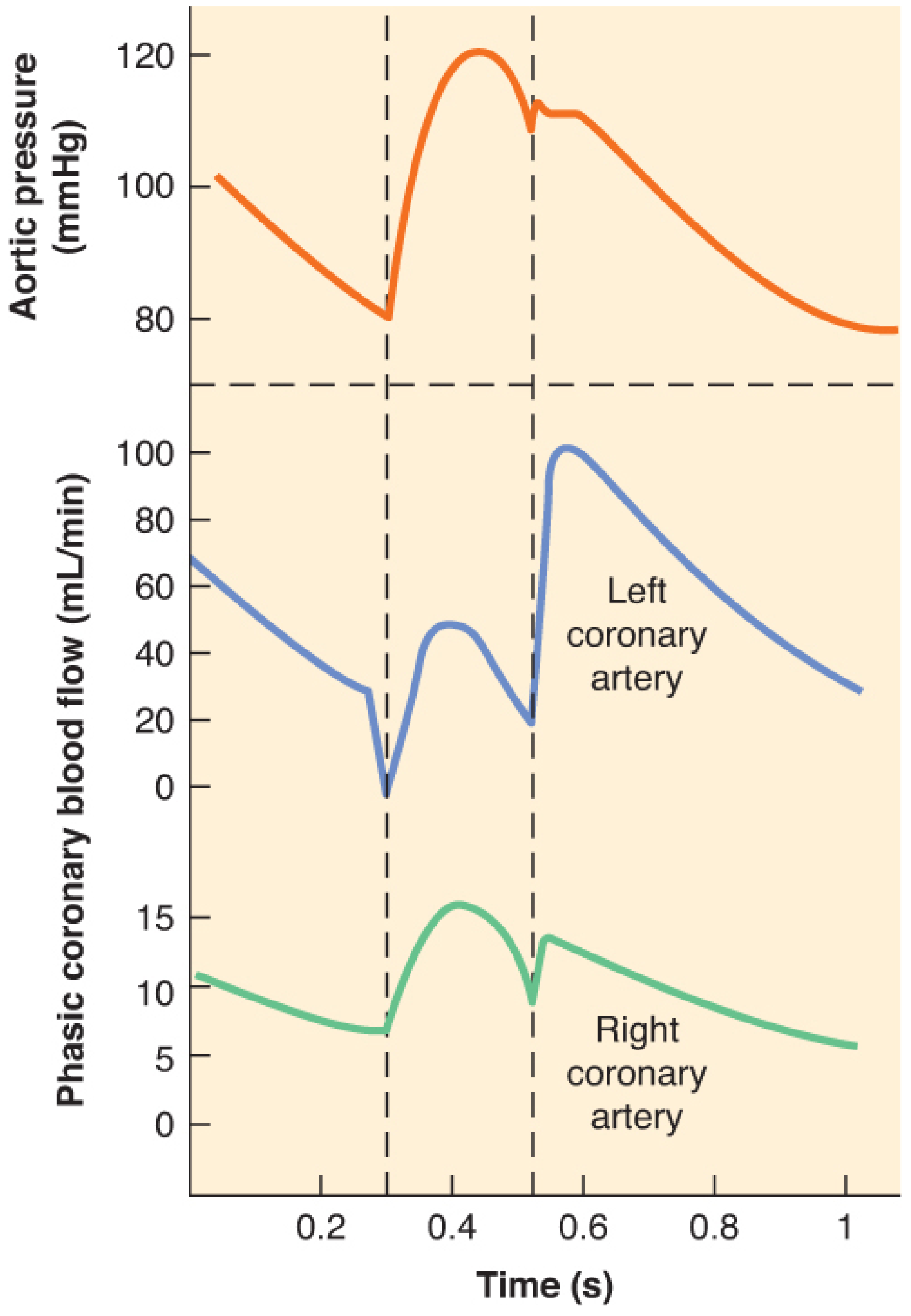
- LV coronary flow: Occurs almost entirely during diastole because extravascular compressive forces impede subendocardial intramural vessels during systole
- Despite systolic limitation, uniform transmural LV perfusion is preserved (subepicardial:subendocardial ratio = 1:1) via metabolically mediated arteriolar dilation during diastole
- RV, LA, RA: Pressures remain below aortic pressure throughout the cycle, so compressive forces do not impede flow - right coronary flow occurs in both systole and diastole
Heart rate and tachycardia: Increased heart rate shortens diastole but subendocardial flow is usually maintained by recruiting coronary flow reserve. However, tachycardia can cause subendocardial ischemia when a flow-limiting stenosis or pressure-overload hypertrophy is present.
4. Myocardial Oxygen Supply-Demand Balance
The Heart is Aerobic and Has Limited O₂ Reserve
- The heart depends almost entirely on aerobic metabolism - myocardial O₂ requirements are disproportionately high (7% of total body O₂) relative to its mass (0.5% of body weight)
- ~75% of O₂ carried by hemoglobin is extracted at baseline (coronary sinus O₂ tension = only 20 mmHg)
- Unlike skeletal muscle, the LV has minimal O₂ extraction reserve - it must increase flow to meet increased demand
- Contraction ceases within 10-15 seconds of acute coronary occlusion without collateral flow
- Primary substrates: fatty acids, glucose, and lactate (via mitochondrial oxidative phosphorylation)
Determinants of Myocardial O₂ Supply
| Factor | Notes |
|---|---|
| Coronary perfusion pressure | Aortic diastolic - LVEDP |
| Diastolic duration | Shortened by tachycardia |
| Coronary vascular resistance | Controlled by arteriolar tone |
| Hemoglobin/O₂ content | Polycythemia or anemia affects viscosity and O₂ delivery |
Determinants of Myocardial O₂ Demand
| Factor | Notes |
|---|---|
| Heart rate | Most important - doubles demand per beat increment |
| Wall stress (afterload) | ↑ with systemic hypertension, aortic stenosis |
| Contractility | Sympathetic activation increases demand |
| Preload (wall tension) | Laplace's law: T = P × r |
5. Metabolic Regulation of Coronary Blood Flow
Flow-metabolism coupling is the principal regulatory mechanism: the myocardium releases vasodilatory mediators proportional to energy utilization ("feed-forward" mechanism). Key mediators include:
Nitric Oxide (NO) - Primary Vasodilator
- Synthesized by endothelial NO synthase (eNOS)
- Stimulated by ↑ intracellular Ca²⁺ (via bradykinin, acetylcholine) or wall shear stress
- Diffuses into arteriolar smooth muscle → stimulates cGMP → vasodilation
- Short half-life; rapidly scavenged by hemoglobin
- Inhibited by atherosclerosis, diabetes, and hypercholesterolemia - leading to dysregulated coronary flow
KATP Channels
- Open when ATP decreases → smooth muscle hyperpolarization → inhibit Ca²⁺ entry → vasodilation
- Mediate basal coronary tone and response to reduced perfusion pressure, increased O₂ demand, and reactive hyperemia
Adenosine
- ATP metabolite; relevant mainly during tissue hypoxia (when it is released)
- Previously thought to be the primary mediator - now recognized as a hypoxia-specific dilator
Prostacyclin (PGI₂)
- Arachidonic acid metabolite; opens KATP channels
- Inhibits platelet aggregation + causes arteriolar vasodilation
- Plays a minor role in routine metabolic regulation
Endothelin-1 (ET-1)
- Potent endogenous vasoconstrictor produced by endothelium
- Acts on ET-A and ET-B receptors on smooth muscle
- Counterbalanced by tonic NO under normal conditions
- Pathologic vasoconstriction occurs when NO release is impaired (hypertension, diabetes, heart failure)
6. Coronary Flow Reserve
Coronary flow reserve (CFR) = Maximum / Baseline coronary blood flow
- Normal CFR: 500-600% in LV and RV
- Measured by reactive hyperemia (brief occlusion) or pharmacologic vasodilation
CFR is reduced by:
- Coronary artery stenosis
- Pressure-overload hypertrophy
- Microvascular dysfunction
Stenosis thresholds:
- 50% luminal diameter reduction: CFR first becomes detectable
- ~90% diameter reduction: Peak reactive hyperemia is abolished; associated with angina at minimal exertion (threshold for unstable angina)
7. Pressure-Flow Autoregulation
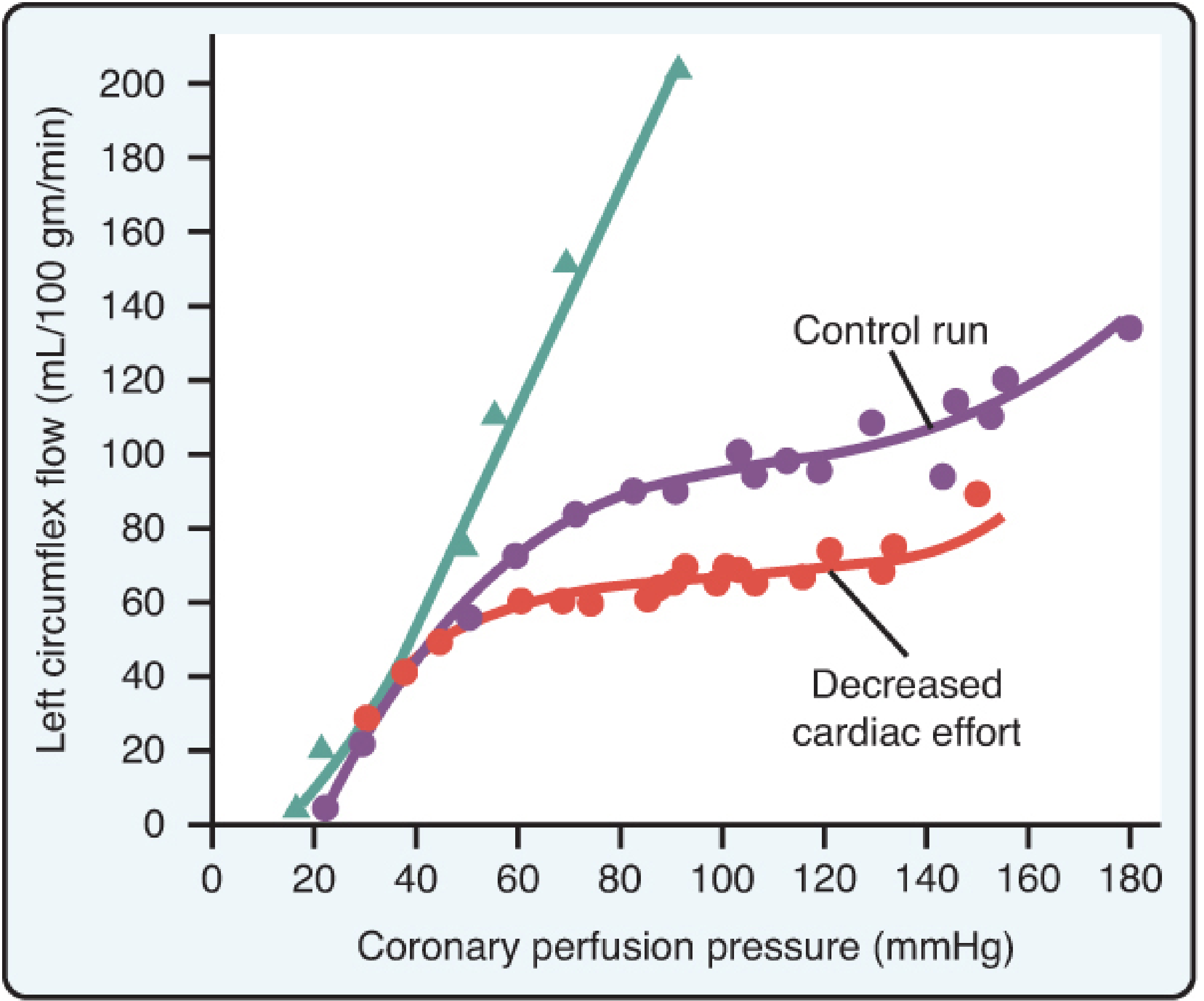
The coronary circulation maintains relatively constant blood flow across a wide range of perfusion pressures (60-140 mmHg) through compensatory adjustments in arteriolar vasomotor tone:
- Below 60 mmHg: Maximal vasodilation; vasodilator reserve is exhausted; flow falls passively
- Above 140 mmHg: Coronary vessels are distended beyond the capacity of smooth muscle to constrict; flow rises passively
- Autoregulation is independent of the autonomic nervous system - it is an intrinsic myogenic phenomenon
- The autoregulatory plateau shifts downward with decreased myocardial O₂ demand (and upward with increased demand)
8. Neural Control of Coronary Circulation
| Receptor | Location | Effect |
|---|---|---|
| α₁-adrenoceptors | Large/intermediate vessels | Vasoconstriction (minor effect on resistance) |
| α₂-adrenoceptors | Arterioles (predominant) | Vasoconstriction; exaggerated with atherosclerosis |
| β₁-adrenoceptors | Arterioles | Vasodilation |
| Muscarinic M₃ receptors | Endothelium + smooth muscle | NO-cGMP vasodilation (normal); vasoconstriction (dysfunctional endothelium) |
Net effect of sympathetic stimulation: LV coronary flow increases because the large increase in myocardial O₂ demand triggers metabolic vasodilation that overwhelms α₂-mediated vasoconstriction.
Net effect of parasympathetic stimulation: Coronary flow decreases because reduced myocardial O₂ demand triggers local metabolic vasoconstriction.
9. Subendocardial Vulnerability
The cardiac subendocardium is particularly susceptible to ischemia because:
- Myocardial contraction itself impedes blood flow to this innermost layer
- It has the highest O₂ demand (greatest wall stress per Laplace's law)
- The transmural perfusion gradient that normally favors the subendocardium during diastole is lost when diastole is shortened (tachycardia) or CPP falls
10. Coronary Microvascular Dysfunction (CMV)
Endothelial health is central to coronary physiology. Risk factors (hypertension, hyperlipidemia, tobacco, diabetes) cause endothelial dysfunction characterized by reduced bioavailable NO, promoting an inflammatory atherogenic environment. A 2024 meta-analysis (PMID 38549197) showed coronary microvascular dysfunction significantly impacts outcomes in heart failure with preserved ejection fraction. A 2025 systematic review (PMID 40068789) provides updated therapeutic strategies for CMV.
Sources:
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - "Coronary Physiology," pp. 857-864
- Sabiston Textbook of Surgery, The Biological Basis of Modern Surgical Practice - "Coronary Artery Anatomy and Physiology," pp. 2483-2484
This is a shared conversation. Sign in to Orris to start your own chat.