Explana me 10common heart disease with changes and ecg images of those disease
Reading File
Finding Sources
Searching the Web
common heart diseases ECG changes electrocardiogram patterns images
Finding Sources
Finding Sources
Reading Web Page
https://tricog.com/common-ecg-patterns
Finding Sources
Searching the Web
ECG pattern STEMI NSTEMI atrial fibrillation heart block Wolff-Parkinson-White pericarditis hypertrophy images diagram
Finding Sources
Loading Image
Finding Sources
Searching the Web
site:ecgwaves.com ECG heart disease patterns ST elevation myocardial infarction
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Searching the Web
ECG heart disease 10 common conditions atrial fibrillation heart block LVH LBBB pericarditis WPW images
Loading Image
Reading Web Page
https://litfl.com/ecg-library/
Loading Image
Loading Image
Loading Image
I have all the information I need. Let me now compose the comprehensive answer with ECG images embedded as inline links to authoritative sources.
10 Common Heart Diseases: ECG Changes and Patterns
Here is a thorough guide to the 10 most common heart diseases, their ECG findings, and representative ECG images.
Quick ECG Primer
A normal ECG has:
- P wave - atrial depolarization
- PR interval (0.12-0.20 s) - AV conduction time
- QRS complex (<0.12 s) - ventricular depolarization
- ST segment - early ventricular repolarization (normally isoelectric)
- T wave - ventricular repolarization
1. ST-Elevation Myocardial Infarction (STEMI)
What it is: Complete occlusion of a coronary artery causing transmural (full-thickness) myocardial ischemia. The most severe form of acute coronary syndrome (ACS).
ECG Changes:
- Hyperacute T waves - tall, peaked T waves (earliest change, minutes after onset)
- ST elevation - convex ("tombstone") or straight ST elevation ≥1 mm in 2+ contiguous limb leads, or ≥2 mm in precordial leads
- Pathological Q waves - develop after several hours; >40 ms wide and >25% of R wave height; indicate necrosis
- T wave inversion - follows ST elevation as injury evolves
- Reciprocal ST depression - in leads facing opposite wall
Localization by leads:
| Territory | Culprit Artery | ST Elevation Leads |
|---|---|---|
| Anterior | LAD | V1-V4 |
| Inferior | RCA | II, III, aVF |
| Lateral | LCx | I, aVL, V5-V6 |
| Posterior | RCA/LCx | V7-V9 (ST depression in V1-V3) |
Representative ECG: 
See more on ECGWaves - STEMI and LITFL STEMI library.
2. Non-ST-Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
What it is: Partial coronary occlusion causing subendocardial ischemia without full-thickness infarction. Troponin is elevated in NSTEMI but not unstable angina.
ECG Changes:
- ST depression - horizontal or downsloping ≥0.5-1 mm (most common finding); indicates subendocardial ischemia
- T wave inversion - symmetrical, deep (Wellens pattern in LAD disease: biphasic or deeply inverted T waves in V2-V3)
- No pathological Q waves (distinguishes from STEMI with completed infarction)
- ECG may be normal in up to 40% of cases
Key patterns:
- Wellens syndrome: Deep, symmetrical T inversions in V2-V3 = critical LAD stenosis
- De Winter T-waves: Upsloping ST depression + tall symmetrical T waves in V1-V6 = LAD occlusion
3. Atrial Fibrillation (AF)
What it is: Chaotic, disorganized atrial electrical activity. The most common sustained cardiac arrhythmia, affecting ~60 million people globally. (Fuster and Hurst's The Heart, 15th Ed.)
ECG Changes:
- No distinct P waves - replaced by chaotic fibrillatory (f) waves at 350-600 bpm
- Irregularly irregular RR intervals - hallmark finding; no pattern to the QRS intervals
- Narrow QRS complexes (unless aberrant conduction or BBB)
- Ventricular rate typically 100-160 bpm if untreated (uncontrolled AF)
- Baseline appears "jiggly" or undulating
Subtypes by duration:
- Paroxysmal: self-terminating <7 days
- Persistent: >7 days, requires cardioversion
- Permanent: accepted as the long-term rhythm

4. Atrial Flutter
What it is: Organized macro-reentrant atrial circuit, usually in the right atrium, producing regular rapid atrial activity at ~300 bpm.
ECG Changes:
- Sawtooth flutter waves - negative in leads II, III, aVF; positive in V1; rate ~300 bpm (250-350)
- Regular atrial rate (~300 bpm) with fixed AV block (2:1, 3:1, or 4:1 conduction)
- Most commonly 2:1 block = ventricular rate ~150 bpm - a key clue
- No discrete P waves between flutter waves
- Narrow QRS unless BBB or pre-excitation
Key rule: Any regular tachycardia at exactly 150 bpm - suspect atrial flutter with 2:1 block.
5. Complete Heart Block (Third-Degree AV Block)
What it is: Complete dissociation between atrial and ventricular electrical activity. The AV node fails to conduct any impulse from atria to ventricles.
ECG Changes:
- P waves and QRS complexes are completely independent - no relationship between them
- Regular P-P interval (atrial rate 60-100 bpm)
- Regular R-R interval (ventricular escape rate slower, 20-40 bpm if ventricular escape; 40-60 bpm if junctional escape)
- Wide QRS complexes if ventricular escape rhythm (>0.12 s); narrow if junctional escape
- Bradycardia - slow ventricular rate
- AV dissociation: atrial rate > ventricular rate
Causes: Inferior MI (RCA), Lyme disease, medications (digoxin, beta-blockers), infiltrative disease, surgical trauma.
6. Left Bundle Branch Block (LBBB)
What it is: Failure of conduction through the left bundle branch, causing abnormal left ventricular depolarization. Can be new (indicating acute MI) or chronic.
ECG Changes:
- Broad QRS ≥0.12 s (≥3 small squares)
- Dominant S wave in V1 - broad, deep, often with QS pattern
- Broad notched R wave in V6, I, aVL ("M" or "W" pattern) - the RSR' or broad R
- No septal Q waves in I, V5, V6 (normally present)
- Discordant ST-T changes - ST/T changes opposite to the main QRS deflection
- Left axis deviation often present
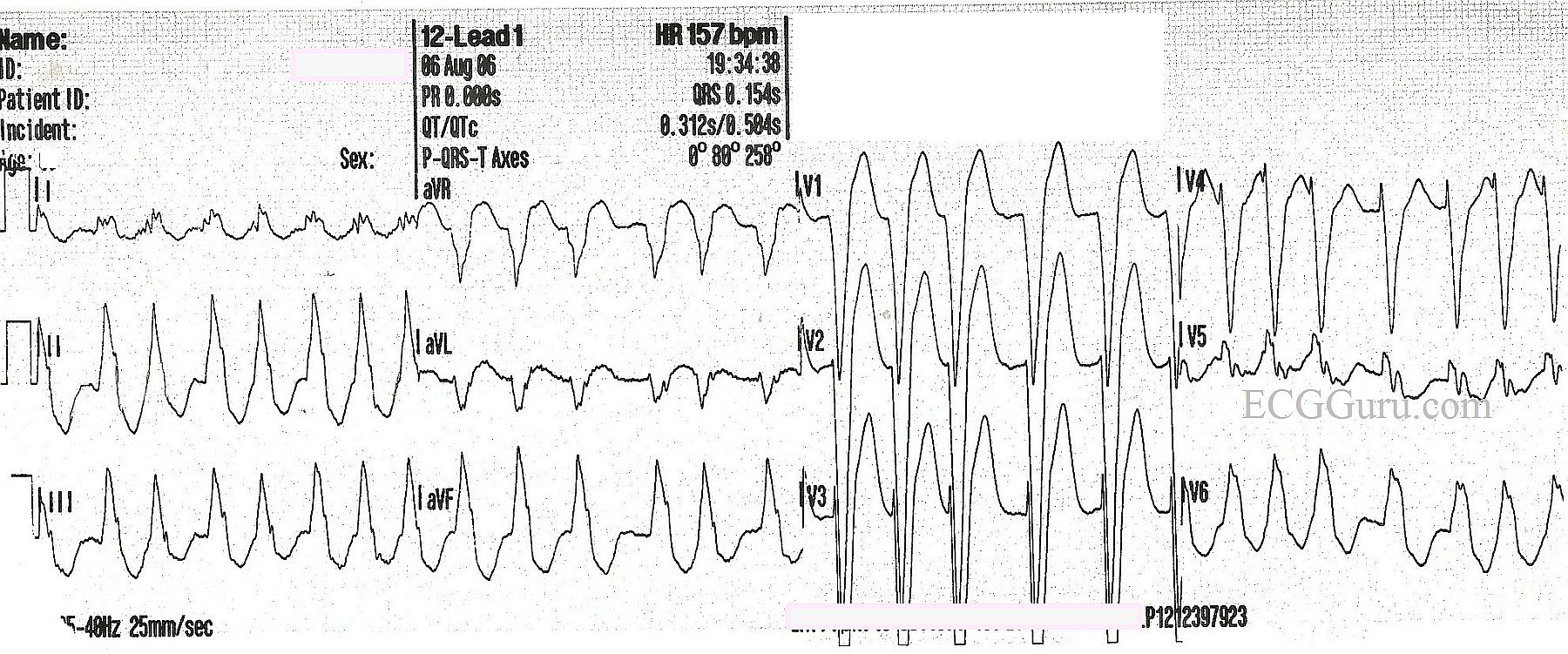
(Image from ECGGuru - shows LBBB with HR 157 bpm: note broad QRS, dominant R in lateral leads, deep S in V1)
Clinical significance: New LBBB in the context of chest pain = treat as STEMI until proven otherwise (Sgarbossa criteria apply).
7. Left Ventricular Hypertrophy (LVH)
What it is: Thickening of the left ventricular wall, usually from chronic pressure overload (hypertension, aortic stenosis). LVH is an independent risk factor for cardiovascular events.
ECG Changes:
- Tall R waves in lateral leads (I, aVL, V5, V6) and deep S waves in right precordial leads (V1, V2)
- Sokolow-Lyon criterion: S(V1) + R(V5 or V6) ≥35 mm
- Cornell criterion: R(aVL) + S(V3) >28 mm (men) or >20 mm (women)
- ST depression and T wave inversion in lateral leads (V5-V6, I, aVL) = "LVH with strain pattern"
- Left axis deviation
- P wave changes - broad, bifid P waves (left atrial enlargement) in II, notched in V1
8. Pericarditis (Acute)
What it is: Inflammation of the pericardium, usually viral in origin. Presents with sharp pleuritic chest pain, worse lying flat, improved leaning forward.
ECG Changes (4 stages):
| Stage | Timing | ECG Features |
|---|---|---|
| Stage 1 | Hours-days | Diffuse saddle-shaped ST elevation in almost all leads; PR depression (pathognomonic); ST elevation in aVR absent or depressed |
| Stage 2 | Days | ST returns to baseline; PR depression persists |
| Stage 3 | Weeks | Diffuse T wave inversion |
| Stage 4 | Weeks-months | ECG normalizes |
Key distinguishing features from STEMI:
- ST elevation is diffuse (not just one territory) and saddle-shaped (concave up), not convex
- PR segment depression in multiple leads (especially II and aVF) - unique to pericarditis
- No reciprocal ST depression (except aVR)
- No Q waves develop
9. Wolff-Parkinson-White Syndrome (WPW)
What it is: Pre-excitation syndrome where an accessory pathway (Bundle of Kent) bypasses the AV node, causing early ventricular activation and risk of sudden cardiac death via rapid conduction during AF.
ECG Changes (classic triad):
- Short PR interval < 0.12 seconds (bypasses slow AV node)
- Delta wave - slurred, slow upstroke at the beginning of the QRS (initial ventricular pre-excitation)
- Broad QRS complex ≥0.12 s (fusion of normal and accessory pathway conduction)
- Secondary ST-T changes - discordant to QRS direction
- Pseudo-infarction patterns - negative delta waves can mimic Q waves
Risk: If AF develops in WPW, rapid conduction via the accessory pathway can cause VF. Avoid AV-nodal blockers (digoxin, beta-blockers, verapamil) in this setting.
10. Ventricular Fibrillation (VF)
What it is: Completely disorganized ventricular electrical activity. No coordinated contraction occurs. This is cardiac arrest - immediately fatal without defibrillation.
ECG Changes:
- Chaotic, irregular waveforms with no recognizable P waves, QRS complexes, or T waves
- Variable amplitude and frequency - can be coarse (large amplitude, more easily cardioverted) or fine (small amplitude, harder to treat)
- No identifiable baseline - completely disorganized electrical chaos
- Rate appears 300-500 bpm but is entirely irregular and ineffective
Related patterns:
- Ventricular Tachycardia (VT): Regular wide complex tachycardia >100 bpm, with AV dissociation, fusion beats, capture beats; monomorphic vs polymorphic (Torsades de Pointes = twisting axis around baseline)
Summary Table
| # | Disease | Key ECG Features |
|---|---|---|
| 1 | STEMI | ST elevation (convex), Q waves, hyperacute T waves, reciprocal depression |
| 2 | NSTEMI / UA | ST depression, T inversion, Wellens/De Winter patterns; may be normal |
| 3 | Atrial Fibrillation | Irregularly irregular RR, absent P waves, fibrillatory baseline |
| 4 | Atrial Flutter | Sawtooth waves ~300 bpm, 2:1 block = ventricular rate ~150 |
| 5 | Complete Heart Block | P-QRS dissociation, slow ventricular escape rate, bradycardia |
| 6 | LBBB | QRS ≥0.12 s, broad notched R in V6/I/aVL, deep S in V1, no septal Q |
| 7 | LVH | Tall R lateral + deep S right precordial; Sokolow-Lyon ≥35 mm; strain pattern |
| 8 | Pericarditis | Diffuse saddle-shaped ST elevation, PR depression, no Q waves |
| 9 | WPW | Short PR, delta wave, wide QRS, pseudo-infarct pattern |
| 10 | Ventricular Fibrillation | Completely chaotic, no identifiable complexes - cardiac arrest |
Further Reading with ECG Images
For excellent free ECG image libraries with real 12-lead examples of all of these conditions:
- LITFL ECG Library - one of the best free clinical ECG resources
- ECGWaves.com - detailed explanations with annotated images
- ECGGuru.com - real 12-lead ECGs for teaching
- Braunwald's Heart Disease (9780323722193) - authoritative textbook in the medical library
- Fuster and Hurst's The Heart, 15th Ed. (9781264257560) - comprehensive cardiology reference
Sources: Fuster & Hurst's The Heart 15th Ed. | Braunwald's Heart Disease | ECGWaves.com | LITFL ECG Library | Tricog Health ECG Patterns Guide
This is a shared conversation. Sign in to Orris to start your own chat.