Why axillary tail is the site of high percentage of breast tumor
Reading File
Finding Sources
Finding Sources
Searching the Web
axillary tail of Spence breast cancer high incidence anatomy reason
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Here is a thorough explanation of why the axillary tail is a high-percentage site for breast tumors:
Why the Axillary Tail Is a High-Percentage Site for Breast Tumors
1. The Axillary Tail Is Part of the Upper Outer Quadrant (UOQ) - the Largest Glandular Mass
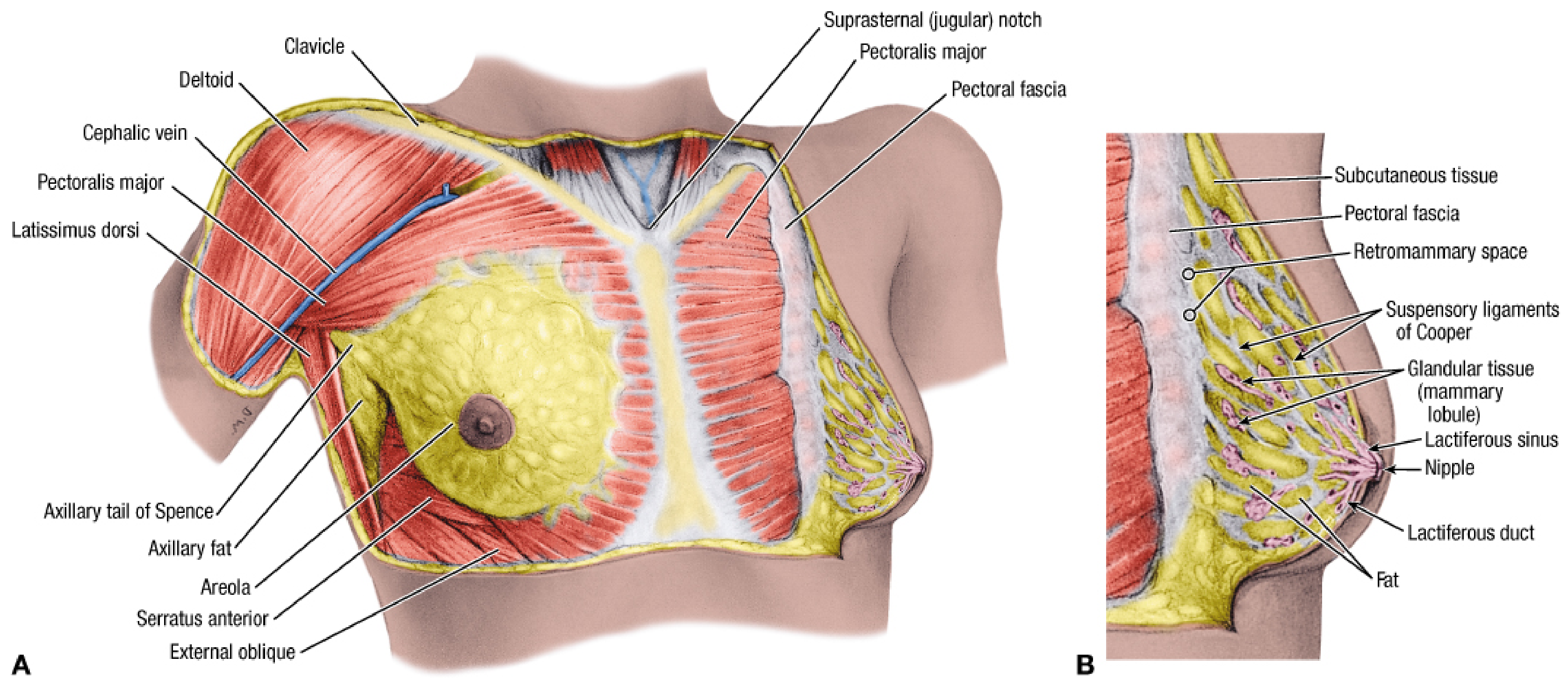
The axillary tail of Spence is an extension of breast tissue from the upper outer quadrant (UOQ) that passes around the inferolateral edge of the pectoralis major and projects into the axilla, often perforating the deep (clavipectoral) fascia through the foramen of Langer.
The key anatomical fact is stated directly in Fischer's Mastery of Surgery:
"Axillary tail of Spence is an extension of breast tissue into the axilla, hence the upper outer quadrant of the breast contains significantly more glandular tissue than any other quadrant."
- Fischer's Mastery of Surgery, 8th ed.
Because breast cancers originate in glandular epithelium (acini, lobules, and lactiferous ducts), the quadrant/region with the highest density of glandular tissue will statistically develop the most tumors - simply by mass and cell number.
2. Reasons the UOQ + Axillary Tail Has the Most Glandular Tissue
| Factor | Explanation |
|---|---|
| Axillary tail extension | Glandular breast tissue extends into axilla, enlarging the effective surface area and cell population of this region |
| 15-20 radial lobes | The glandular lobes radiate toward the nipple; the lateral lobes are more abundant and larger in the UOQ |
| Proportional tissue mass | Approximately 50% of all breast glandular tissue is concentrated in the UOQ - the axillary tail adds to this |
| Ductal anatomy | Lactiferous ducts in this region drain a larger territory, increasing the at-risk epithelial cell population |
3. Rich Lymphatic Drainage Facilitates Spread (and Detection)
Gray's Anatomy for Students notes:
"The upper lateral region of the breast can project around the lateral margin of the pectoralis major muscle and into the axilla. This axillary process may perforate deep fascia and extend as far superiorly as the apex of the axilla."
The axillary tail is directly adjacent to axillary lymph nodes (Levels I, II, III). This means:
- Tumors arising here have immediate access to lymphatic channels
- They tend to present with early nodal metastasis
- CATS (carcinoma of axillary tail of Spence) carries a worse prognosis than standard UOQ cancer - higher grade, more ER/PR-negative tumors, more positive nodes
4. Why Tumors Here Are Clinically Significant
- Tumors in the axillary tail can mimic axillary lymphadenopathy, leading to delayed diagnosis
- They may be understaged on standard mammography (the MLO view specifically images this region, but lesions can be missed)
- They must be distinguished from: axillary lymph node metastases, ectopic accessory breast tissue, and axillary soft tissue tumors
- During mastectomy or breast-conserving surgery, the axillary tail must be actively assessed and removed if involved
5. Summary of Reasons
- Most glandular tissue in the body of the breast concentrates in the UOQ and its axillary extension - more tissue = more cells at risk for malignant transformation
- Hormonal responsiveness - this glandular tissue responds to estrogen/progesterone, driving proliferation and mutation risk
- Ductal epithelium - the axillary tail contains ductal epithelium connected to the main duct system, which is the primary site of ductal carcinoma in situ (DCIS) and invasive ductal carcinoma
- Proximity to lymphatics - rich drainage to axillary nodes makes spread rapid and nodal involvement common
Note on incidence clarification: The question asks about the "axillary tail" being a site of "high percentage" of tumors. This is accurate in the context of the upper outer quadrant (~50% of all breast cancers). However, carcinoma specifically arising from the axillary tail itself (CATS) is actually rare (~0.1-1% of breast cancers) per published literature. The high incidence refers to the UOQ as a whole, of which the axillary tail is the most lateral and glandular-dense component. - PMC case report (Park et al., 2022)
Why there is no fat below nipple and aerola
Finding Sources
Finding Sources
Searching the Web
why no subcutaneous fat beneath nipple areola breast anatomy lactiferous ducts
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Here is the complete answer:
Why There Is No Fat Below the Nipple and Areola
The Direct Answer
The nipple and areola are structurally devoid of fat - this is a well-established anatomical fact explicitly stated in authoritative sources:
"The nipple usually has no sweat glands, fat, or hairs." "The areola is devoid of fat and hair."
- StatPearls: Anatomy, Thorax: Mammary Gland (NCBI)
"The NAC (Nipple-Areola Complex) has no subcutaneous tissue."
- Zucca-Matthes et al., Anatomy of the nipple and breast ducts, Gland Surgery
Reasons Why - The Structural Occupants
The subareolar space is completely occupied by specialized functional structures that leave no room for adipose tissue:
1. Dense Smooth Muscle Layers Replace Subcutaneous Fat
Directly beneath the skin of the nipple-areola complex, instead of subcutaneous fat, there are two layers of smooth muscle:
| Muscle Layer | Orientation | Function |
|---|---|---|
| Muscle of Sappey | Circular (circumferential) | Wraps around the lactiferous duct openings; causes nipple erection on stimulation |
| Muscle of Meyerholz | Radial (longitudinal) | Runs from areola to nipple alongside lactiferous ducts; assists in milk ejection |
These muscle layers occupy the dermis-to-subdermal layer where subcutaneous fat would normally sit. As the surgical anatomy literature states: "The skin of the nipple-areolar complex does not lie on the subcutaneous tissue but on the thin layer of smooth muscles."
2. Lactiferous Ducts Run Directly Under the Skin
Schwartz's Principles of Surgery explains:
"Each lobe of the breast terminates in a major (lactiferous) duct (2-4 mm in diameter), which opens through a constricted orifice into the ampulla of the nipple. Immediately below the nipple-areola complex, each major duct has a dilated portion (lactiferous sinus)."
- Schwartz's Principles of Surgery, 11th Ed.
The 15-20 lactiferous ducts (now considered ~9-10 by ultrasound studies) converge in this region and run almost parallel to each other toward the nipple orifices. This radial arrangement of converging ducts densely packs the subareolar space.
3. Dense Connective Tissue + Suspensory Attachments
In the peri-areolar area, the skin is attached directly to glandular tissue by:
- Suspensory ligaments of Cooper (particularly dense here)
- Subcutaneous smooth muscle fibers
This dense fibrous scaffolding further excludes adipose lobules from taking root in this zone.
4. Fat Only Appears Peripherally - and Disappears Toward the Nipple
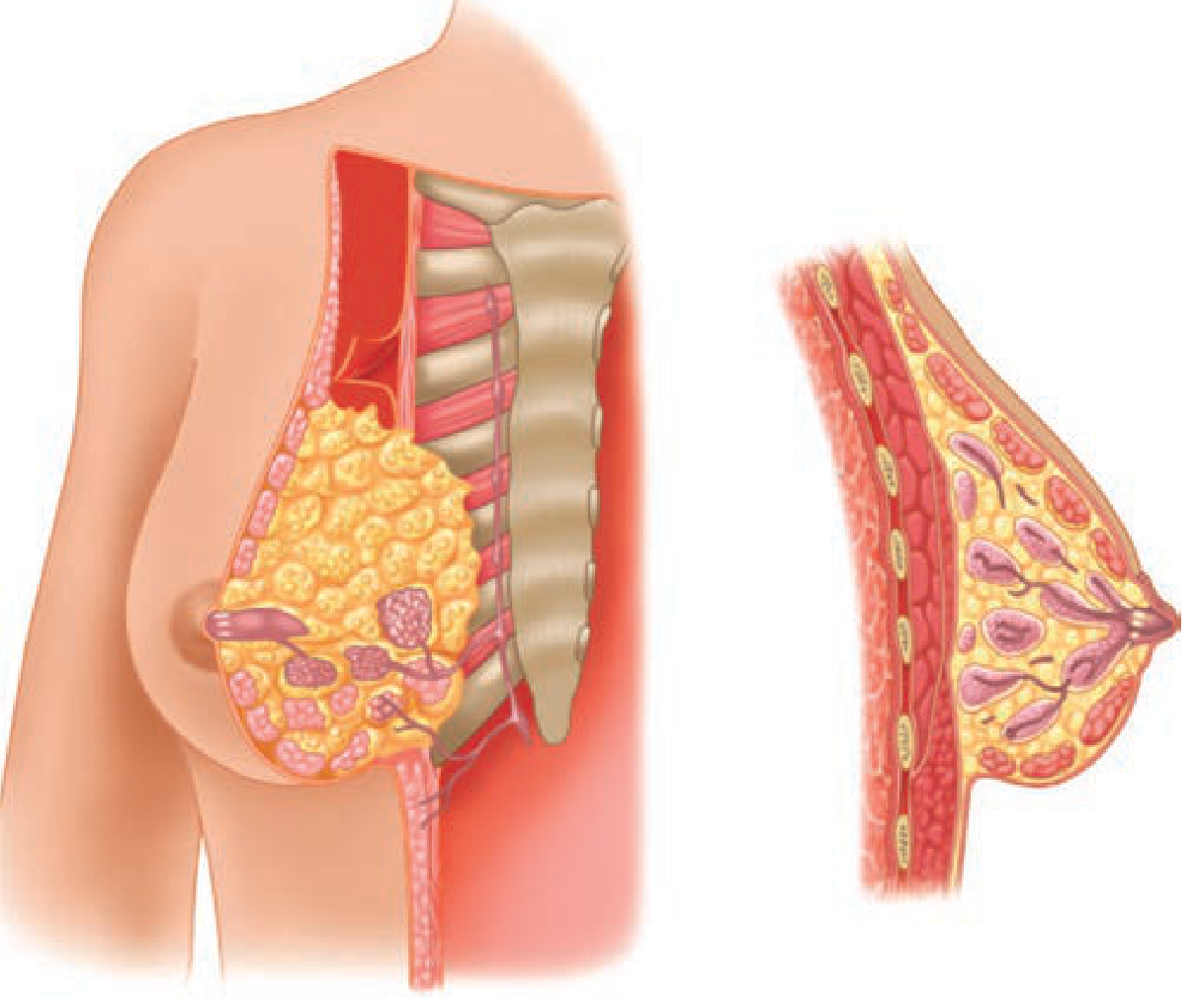
The progression of fat in the breast is gradient-based:
- Periphery of breast: abundant fat lobules between the glandular lobes
- Below the areola: a thin pre-mammary fat layer is present
- Toward the nipple: this fat layer progressively disappears
As stated in the surgical anatomy source: "The layer under the muscles below the areola is made of adipose tissue, which disappears towards the nipple."
Summary Diagram (Conceptual)
NIPPLE TIP
→ No fat, no hair, no sweat glands
→ Smooth muscle (Sappey + Meyerholz)
→ Lactiferous duct orifices
AREOLA
→ No fat, no hair
→ Smooth muscle bundles
→ Montgomery's tubercles (modified sebaceous glands)
→ Dense connective tissue attached to skin
SUB-AREOLAR ZONE
→ Thin fat layer, disappearing toward nipple
→ Converging lactiferous ducts/sinuses
BREAST PERIPHERY
→ Fat lobules abundant, between glandular lobes
Clinical Significance
- Because the nipple-areola lacks fat, incisions here must be radial (not circumferential) to avoid cutting through multiple converging lactiferous ducts - Schwartz's Principles of Surgery, 11th Ed.
- The absence of a fat buffer means tumors arising in this zone cause early skin tethering and nipple retraction - direct involvement of Cooper's ligaments occurs early
- Subareolar abscesses are common because the duct openings are exposed without a protective fat layer
Internal thoracic artery
Finding Sources
Searching the Web
internal thoracic artery anatomy origin branches clinical significance
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Here is a comprehensive overview of the internal thoracic artery:
Internal Thoracic Artery (ITA)
Also known as the internal mammary artery (IMA)
Origin
The ITA arises from the inferior (concave) surface of the first part of the subclavian artery, just distal to the vertebral artery and proximal to the thyrocervical trunk. It is the third named branch of the subclavian artery.
- Gray's Anatomy for Students confirms: "Each internal thoracic artery arises as a major branch of the subclavian artery in the neck."
Course
| Segment | Relations |
|---|---|
| Neck | Passes anteriorly over the cervical dome of the pleura, posterior to the clavicle and large veins (subclavian/brachiocephalic) |
| Superior thoracic aperture | Descends through the aperture into the thorax |
| Anterior thoracic wall | Runs posterior to the costal cartilages of ribs 1-6, ~1 cm lateral to the sternal border, anterior to the transversus thoracis muscle |
| Termination | At the level of the 6th intercostal space, divides into two terminal branches |
Branches
Anterior (Collateral) Branches
| Branch | Distribution |
|---|---|
| Anterior intercostal arteries (spaces 1-6) | Lateral branches supplying upper 6 intercostal spaces; anastomose with posterior intercostals from aorta |
| Perforating branches | Pass forward between costal cartilages to supply pectoral muscles, skin of anterior chest; travel with anterior cutaneous branches of intercostal nerves |
| Medial mammary arteries | Perforating branches from spaces 2-4 that supply the medial breast (this is why parasternal lymph nodes matter in breast cancer spread) |
Posterior (Mediastinal) Branches
| Branch | Distribution |
|---|---|
| Pericardiacophrenic artery | Descends with phrenic nerve; supplies pericardium and diaphragm |
| Mediastinal branches | Thymus, loose areolar tissue of anterior mediastinum |
| Sternal branches | Supply the sternum |
| Bronchial/tracheal branches | Minor contributions |
Terminal Branches (at 6th intercostal space)
| Branch | Course | Supply |
|---|---|---|
| Superior epigastric artery | Passes through diaphragm into rectus sheath | Anterior abdominal wall; anastomoses with inferior epigastric artery (from external iliac) |
| Musculophrenic artery | Runs along costal margin, through diaphragm | Lower intercostal spaces (7-9), diaphragm |
"At approximately the level of the sixth intercostal space, it divides into two terminal branches: the superior epigastric artery... and the musculophrenic artery, which passes along the costal margin, goes through the diaphragm, and ends near the last intercostal space."
- Gray's Anatomy for Students
Relations (Surgical Landmarks)
- Lies ~1 cm from lateral sternal border at upper spaces, increasing to 1.1-1.3 cm by the 6th space
- Accompanied throughout by the internal thoracic vein (drains to brachiocephalic vein)
- Lies between the internal intercostal muscle and the transversus thoracis muscle
- The phrenic nerve crosses it superficially in the neck
Areas of Supply (Summary)
- Anterior chest wall (skin, pectoral muscles, ribs, intercostal muscles)
- Medial breast (via perforating branches)
- Sternum and mediastinum (thymus, pericardium)
- Diaphragm (via pericardiacophrenic and musculophrenic)
- Superior anterior abdominal wall (via superior epigastric)
Important Anastomoses
| Anastomosis | Significance |
|---|---|
| Superior epigastric ↔ Inferior epigastric | Connects subclavian → aortic territory; collateral route in aortic coarctation |
| Anterior ↔ Posterior intercostals | Collateral circulation if aorta or ITA is occluded |
| ITA perforators ↔ lateral thoracic a. | Breast blood supply |
Clinical Significance
1. Coronary Artery Bypass Grafting (CABG)
The Left ITA (LITA) is the conduit of choice for bypassing the left anterior descending (LAD) coronary artery. This is because:
- It is an arterial conduit (not a vein), so it resists atherosclerosis long-term
- Its 10-year patency is >90%, far superior to saphenous vein grafts
- The right ITA (RITA) is used for additional grafts in multiple-vessel disease
- As noted in Sabiston Textbook of Surgery: LITA-to-LAD remains the gold-standard for surgical coronary revascularization
2. Breast Cancer Lymphatics
Perforating branches (spaces 2-4) accompany parasternal lymph nodes - this is the route by which medial breast cancers spread to the internal thoracic (parasternal) nodal chain, making them harder to detect and treat. - Gray's Anatomy for Students
3. Needle/Catheter Procedures
When performing pericardiocentesis, mediastinoscopy, or parasternal nerve blocks, the ITA must be avoided by staying close to the sternal edge (within 5 mm) where it has not yet moved laterally.
4. Aortic Coarctation Collaterals
In coarctation of the aorta, blood bypasses the obstruction via ITA → anterior intercostal arteries ↔ posterior intercostal arteries → descending aorta. This produces the classic "rib notching" on chest X-ray.
5. Reconstructive Surgery
The ITA and its perforators are used in pedicled flaps for chest wall reconstruction after mastectomy or radiotherapy damage.
Anatomical Variations
- ITA may arise from the distal subclavian rather than proximal portion (in some cadavers)
- Common origin with branches of the thyrocervical trunk (rare)
- Trifurcation with a xiphoid branch as a third terminal branch (20-30% of cadavers) - StatPearls, NCBI
This is a shared conversation. Sign in to Orris to start your own chat.