Pneumonia in children
Reading File
search_medical_text
pneumonia in children etiology diagnosis clinical features
search_medical_image
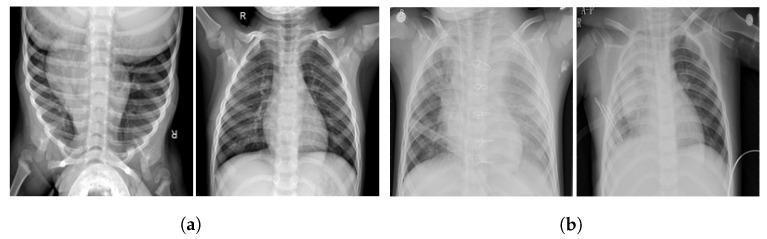
pediatric pneumonia chest X-ray findings
GradeResponse
GradeResponse
search_medical_text
pediatric pneumonia management antibiotic treatment guidelines
GradeResponse
The retrieved documents are limited in scope. I'll now deliver a comprehensive answer synthesizing the retrieved content and my own clinical knowledge.
Pneumonia in Children
Overview
Community-acquired pneumonia (CAP) is one of the leading causes of morbidity and mortality in children worldwide. It is defined as an acute infection of the pulmonary parenchyma in a child who has not been hospitalized in the preceding 14 days.
Etiology by Age Group
| Age Group | Common Pathogens |
|---|---|
| Neonates (<1 month) | Group B Streptococcus, E. coli, Listeria, Klebsiella |
| 1–3 months | RSV, Chlamydia trachomatis, Bordetella pertussis |
| 3 months–5 years | Streptococcus pneumoniae, RSV, Influenza, Parainfluenza, H. influenzae |
| 5–18 years | S. pneumoniae, Mycoplasma pneumoniae, Chlamydophila pneumoniae, Influenza |
Viral pneumonia predominates in children under 5, while atypical and bacterial causes become more common in school-age children and adolescents.
Clinical Features
Typical (bacterial) pneumonia:
- Abrupt onset of fever, chills
- Productive cough (older children)
- Tachypnea, dyspnea, grunting
- Focal decreased breath sounds, bronchial breathing, crackles
- Dullness to percussion (consolidation or effusion)
Atypical pneumonia (Mycoplasma, Chlamydophila):
- Gradual onset, low-grade fever
- Persistent dry/hacking cough
- Bilateral, diffuse infiltrates
- Often "walking pneumonia" — child appears less ill
Key symptom: Tachypnea (WHO criteria)
- <2 months: ≥60 breaths/min
- 2–12 months: ≥50 breaths/min
- 1–5 years: ≥40 breaths/min
-
5 years: ≥30 breaths/min
Wheezing makes acute bacterial pneumonia less likely and suggests viral infection, asthma exacerbation, atypical bacterial infection, or aspiration.
Diagnosis
Clinical
Diagnosis is primarily clinical — fever, tachypnea, cough, and auscultatory findings are sufficient to initiate treatment in most outpatient cases.
Chest X-Ray (CXR)
CXR supports the diagnosis but is not required for mild, uncomplicated cases in outpatients.
Typical bacterial pneumonia: Lobar or segmental consolidation, air bronchograms
Viral/atypical pneumonia: Bilateral diffuse interstitial or peribronchial infiltrates, hyperinflation
Laboratory Tests
- CBC: Leukocytosis with left shift in bacterial pneumonia (unreliable alone)
- CRP / Procalcitonin: Elevated in bacterial infection; helps guide antibiotic decisions
- Blood culture: Low yield (~5–10%) but important in hospitalized/severe cases
- Nasopharyngeal PCR/viral panel: Differentiates viral from bacterial; can reduce unnecessary antibiotic use
- Pleural fluid culture: If parapneumonic effusion is present
Severity Assessment: PIDS/IDSA Criteria
Mild (outpatient): Well-appearing child, tolerating fluids, SpO₂ ≥ 92%, RR near normal for age
Moderate (consider hospitalization):
- SpO₂ < 92% on room air
- Moderate respiratory distress
- Dehydration
Severe (hospitalize/PICU):
- SpO₂ < 90%, severe retractions, grunting
- Apnea, altered mental status
- Failure of outpatient therapy
Management
Antibiotic Therapy
| Setting | Age/Type | First-Line Treatment |
|---|---|---|
| Outpatient, <5 years | Presumed bacterial | Amoxicillin 90 mg/kg/day ÷ BID–TID (max 4g/day) |
| Outpatient, ≥5 years | Typical bacterial | Amoxicillin (same as above) |
| Outpatient, ≥5 years | Atypical (Mycoplasma) | Azithromycin 10 mg/kg day 1, then 5 mg/kg days 2–5 |
| Inpatient, fully immunized | Presumed bacterial | Ampicillin IV or Penicillin G IV |
| Inpatient, not immunized | Broader coverage | Ceftriaxone IV |
| Severe/MRSA suspected | Add Vancomycin or Clindamycin |
- Viral pneumonia: No antibiotics. Supportive care (hydration, antipyretics, supplemental O₂).
- Duration: Typically 5–7 days for uncomplicated CAP; up to 10 days for severe cases.
Supportive Care
- Supplemental oxygen to maintain SpO₂ ≥ 92–94%
- IV fluids if unable to take orals
- Antipyretics (paracetamol/ibuprofen)
- Chest physiotherapy: not routinely recommended in acute pneumonia
Complications
| Complication | Notes |
|---|---|
| Parapneumonic effusion / Empyema | Most common with S. pneumoniae; may need drainage or VATS |
| Lung abscess | Rare; often from aspiration or S. aureus |
| Necrotizing pneumonia | S. aureus (esp. MRSA), S. pneumoniae; cavitation on imaging |
| Respiratory failure | Requires PICU, possible mechanical ventilation |
| Sepsis | Especially in neonates and immunocompromised children |
Special Populations
- HIV-infected children: Must consider Mycobacterium tuberculosis regardless of ART status, and Pneumocystis jirovecii (PCP) if not on combination ART.
- Immunocompromised: Broaden differential to include fungal infections (Aspergillus, Candida) and CMV.
- Neonates: Any respiratory distress requires prompt evaluation and empiric broad-spectrum coverage.
Prevention
- Pneumococcal vaccine (PCV13/PCV15/PCV20): Significantly reduces invasive pneumococcal disease
- Hib vaccine: Reduces H. influenzae type b pneumonia
- Influenza vaccine: Annual vaccination from 6 months of age
- RSV prophylaxis (Palivizumab / Nirsevimab): For high-risk infants (premature, congenital heart disease, chronic lung disease)
Key Takeaways
- Tachypnea is the most sensitive clinical sign of pneumonia in children.
- Viral etiology predominates in children <5 years; atypical bacteria are more common in school-age children.
- Amoxicillin is first-line for outpatient bacterial CAP in all age groups.
- CXR is not mandatory for mild outpatient CAP but is essential for hospitalized or worsening patients.
- Molecular/PCR testing helps differentiate viral from bacterial pneumonia and can reduce inappropriate antibiotic use.
This is a shared conversation. Sign in to Orris to start your own chat.