10 ECG of heart disease
Reading File
Searching Images
ECG electrocardiogram heart disease patterns
Finding Sources
Searching Images
myocardial infarction ST elevation ECG
Searching Images
atrial fibrillation ECG irregular rhythm
Searching Images
complete heart block third degree AV block ECG
Searching Images
Wolff-Parkinson-White WPW delta wave ECG pre-excitation
Searching Images
ventricular tachycardia VT wide complex tachycardia ECG
Searching Images
long QT syndrome QTc prolongation ECG torsades de pointes
Searching Images
left bundle branch block LBBB ECG
Searching Images
pericarditis saddle shaped ST elevation diffuse ECG
I now have excellent ECG images for 10 distinct heart disease patterns. Here is a comprehensive ECG atlas covering 10 important cardiac conditions:
10 ECGs of Heart Disease
1. Anterior STEMI — ST-Elevation Myocardial Infarction
Key findings: Convex ("tombstone") ST-segment elevation in V2–V5 and lateral leads I/aVL, with reciprocal ST depression in inferior leads (II, III, aVF). Sinus bradycardia present.
Cause: Proximal left anterior descending (LAD) artery occlusion causing transmural ischemia of the anterior and lateral walls. Requires emergent reperfusion (PCI or thrombolysis).
2. Inferior + Anterior Multi-territory STEMI
Key findings: ST elevation in inferior leads (II, III, aVF) with reciprocal depression in aVL, plus ST elevation in anteroseptal leads V1–V3 with "tombstone" morphology.
Cause: Multi-vessel coronary occlusion or a wrap-around LAD occluding both territories. Indicates extensive infarction with high mortality risk.
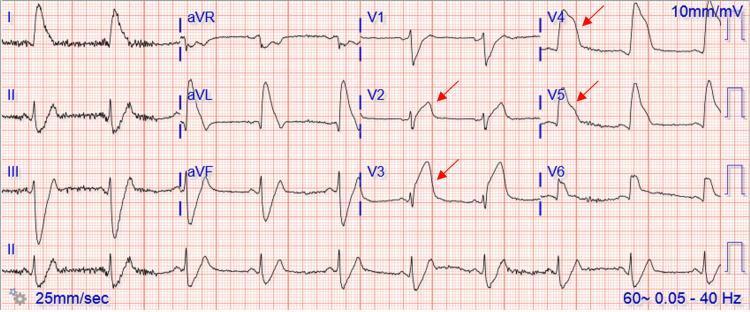
3. Wellens' Syndrome — Pre-Infarction LAD Stenosis
Key findings: Biphasic T-waves in V2–V3 (Type A) and deep symmetric T-wave inversions in V4–V5 during chest pain-free period. Normal ST segments in limb leads.
Cause: Critical proximal LAD stenosis. This pattern warns of impending massive anterior MI — stress testing is contraindicated; urgent angiography required.
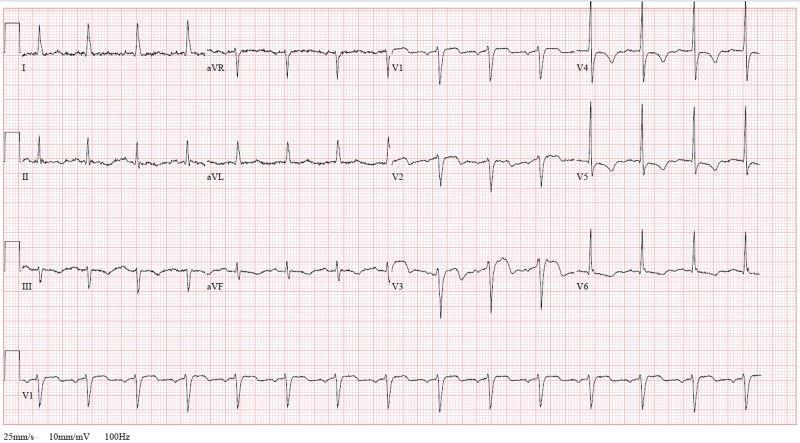
4. Left Ventricular Hypertrophy (LVH) with Strain
Key findings: Tall R-waves in V5–V6 and deep S-waves in V1–V2 meeting Sokolow-Lyon criteria. ST depression and T-wave inversions in inferolateral leads (II, III, aVF, V5–V6) — the "strain pattern."
Cause: Chronic pressure overload from hypertension, aortic stenosis, or hypertrophic cardiomyopathy. Strain pattern signals increased cardiovascular risk.
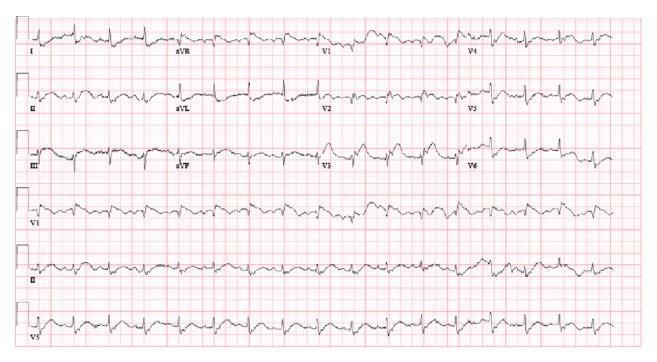
5. Atrial Fibrillation (AF)

Key findings: Irregularly irregular R-R intervals, absent P waves replaced by fine fibrillatory (f) waves (best seen in V1 and lead II), rapid ventricular response >100 bpm, narrow QRS complexes.
Cause: Disorganized atrial electrical activity; associated with hypertension, heart failure, valvular disease, hyperthyroidism, and post-surgery. Risk of thromboembolic stroke.
6. Third-Degree (Complete) AV Block

Key findings: Complete AV dissociation — P waves (fast atrial rate) bear no relationship to QRS complexes (slow ventricular escape rhythm). Wide QRS indicates infra-Hisian escape pacemaker.
Cause: AV nodal failure from ischemia, surgery, fibrosis, or endocarditis. Life-threatening bradycardia — requires urgent permanent pacemaker.
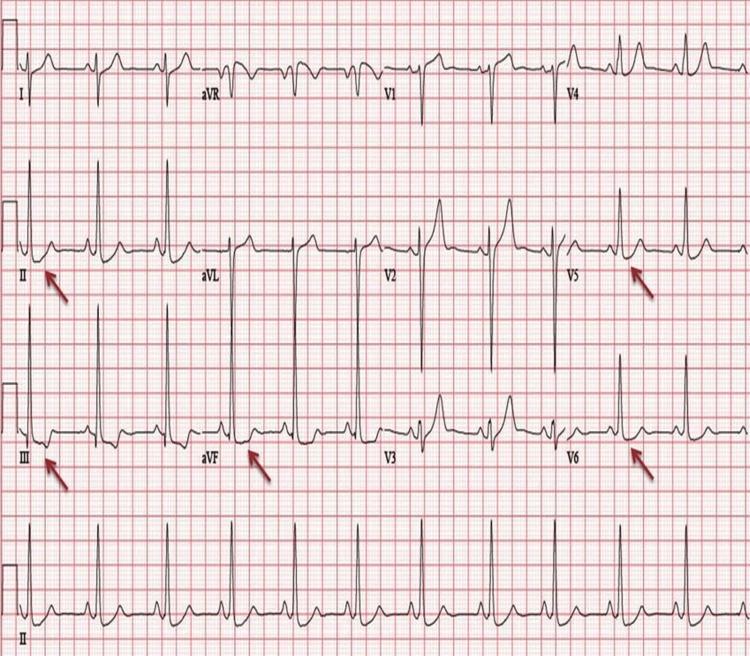
7. Wolff-Parkinson-White (WPW) Syndrome
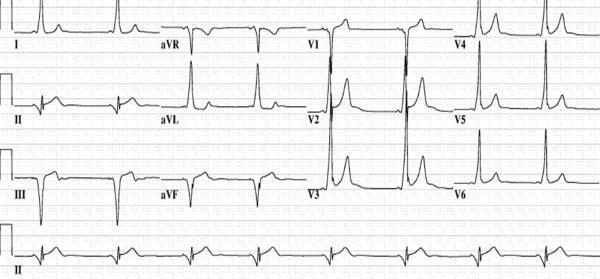
Key findings: Short PR interval (<120 ms), widened QRS with delta wave (slurred upstroke), secondary ST-T changes discordant with QRS. Negative delta waves in inferior leads indicate posteroseptal accessory pathway.
Cause: Bundle of Kent — anomalous AV bypass tract causing ventricular pre-excitation. Risk of sudden death via AF with rapid accessory pathway conduction; treat with catheter ablation.
8. Monomorphic Ventricular Tachycardia (VT)

Key findings: Wide complex tachycardia (~150–200 bpm), uniform QRS morphology, superior axis (negative in II, III, aVF), positive concordance across precordial leads V1–V6, no preceding P waves.
Cause: Structural heart disease (dilated cardiomyopathy, post-MI scar reentry). Hemodynamically unstable — cardiovert immediately; stable VT may be treated with amiodarone or lidocaine.
9. Long QT Syndrome (LQTS) with Torsades de Pointes
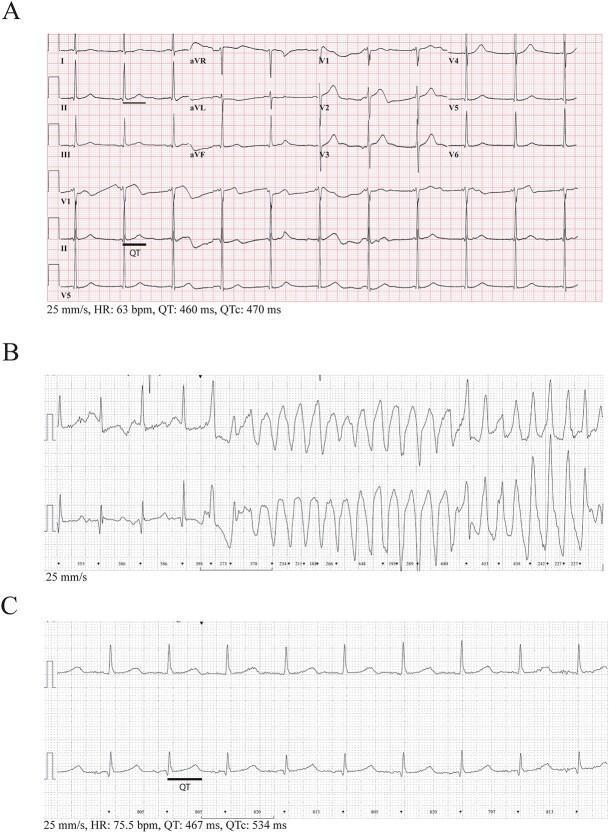
Key findings: Markedly prolonged QTc (≥470 ms in panel), broad flat T-waves in baseline. Transition to Torsades de Pointes (TdP) — polymorphic VT with "twisting" QRS complexes around the isoelectric line.
Cause: Congenital channelopathy (KCNQ1, KCNH2, SCN5A mutations) or acquired (drugs, hypokalemia, hypomagnesemia). Magnesium IV is first-line for TdP; avoid QT-prolonging drugs.
10. Acute Pericarditis

Key findings: Diffuse concave ("saddle-shaped") ST elevation across I, II, III, aVF, V2–V6. PR-segment depression in II/inferior leads, PR elevation in aVR (Spodick's sign). No reciprocal changes (unlike STEMI). Sinus tachycardia.
Cause: Pericardial inflammation (viral, post-MI/Dressler's, autoimmune, uremic). Treated with NSAIDs + colchicine. Key distinction from STEMI: diffuse distribution not following one coronary territory.
Quick Reference Summary
| # | Condition | Key ECG Feature |
|---|---|---|
| 1 | Anterior STEMI | Convex ST↑ V2–V5, reciprocal inferior ST↓ |
| 2 | Multi-territory STEMI | ST↑ inferior + anteroseptal simultaneously |
| 3 | Wellens' Syndrome | Biphasic/deep T inversions V2–V4 (pain-free) |
| 4 | LVH + Strain | High voltage + lateral ST↓, T-wave inversions |
| 5 | Atrial Fibrillation | Irregularly irregular, no P waves, fibrillatory baseline |
| 6 | 3° AV Block | Complete AV dissociation, slow escape rhythm |
| 7 | WPW Syndrome | Short PR, delta wave, widened QRS |
| 8 | Ventricular Tachycardia | Wide complex tachycardia, no P waves, AV dissociation |
| 9 | Long QT / TdP | QTc >470 ms → twisting polymorphic VT |
| 10 | Acute Pericarditis | Diffuse saddle ST↑, PR depression, no reciprocal changes |
This is a shared conversation. Sign in to Orris to start your own chat.