Adult tof
Reading File
Finding Sources
Searching PubMed
"tetralogy of Fallot" AND adult
Finding Sources
Searching PubMed
"tetralogy of Fallot" AND "repaired" AND outcomes
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have excellent content from Braunwald's. Let me compile the comprehensive answer.
Adult Tetralogy of Fallot (TOF)
Overview
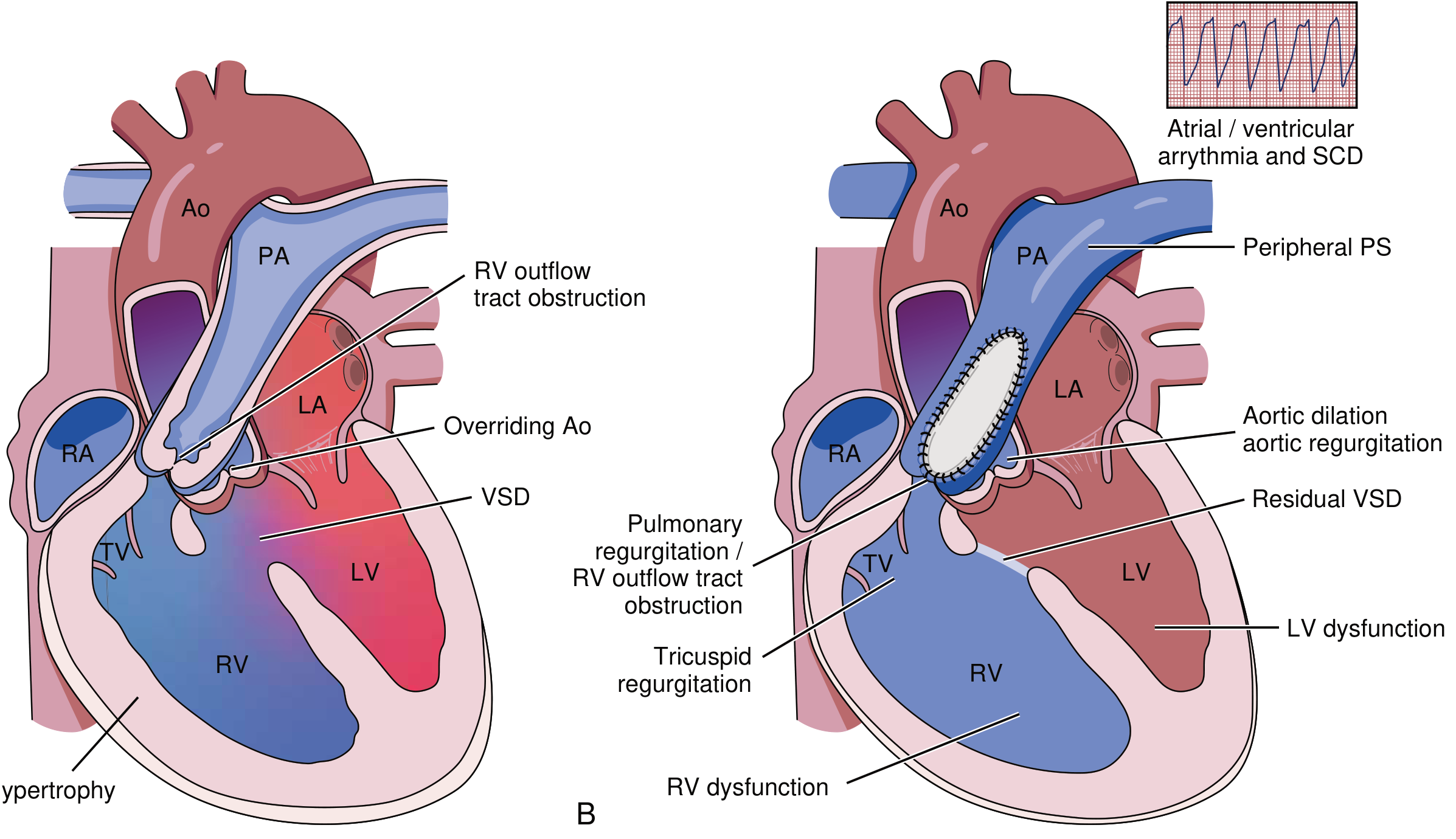
TOF is the most common cyanotic congenital heart defect. It consists of four components:
- Ventricular septal defect (VSD)
- Right ventricular outflow tract (RVOT) obstruction - subpulmonary stenosis from anterocephalad deviation of the outlet septum
- Overriding aorta
- Right ventricular hypertrophy
Patients with repaired TOF now constitute one of the largest groups of adult congenital heart disease (ACHD) patients. Life expectancy is excellent for those with uncomplicated anatomy, early primary repair, and preserved biventricular function.
Anatomy and Variants
| Variant | Features |
|---|---|
| TOF with pulmonary atresia + MAPCAs | ~15% of cases; no direct heart-PA connection; repair via unifocalization + conduit |
| TOF with absent pulmonary valve | Markedly stenotic/absent PV leaflets; severely aneurysmal PAs; may compress airways at birth |
| Right aortic arch | ~25% of patients |
| Anomalous coronary arteries | LAD from RCA crossing RVOT - surgically important, may require RV-PA conduit |
Clinical Features in Adults
Symptoms:
- Exertional dyspnoea
- Palpitations
- Syncope
Examination findings:
- Normal oxygen saturations (post-repair)
- Diastolic to-and-fro murmur at pulmonary area = pulmonary regurgitation (PR)
- RV heave + single second heart sound if PR is severe
- Overt RHF (hepatomegaly, elevated JVP, edema) is uncommon
ECG: Complete right bundle branch block (RBBB) common in older adults, related to surgical technique
BNP: Predictive of mortality
Long-Term Problems in Repaired TOF
RV volume overload from:
- Pulmonary regurgitation (most common long-term issue)
- Tricuspid regurgitation
- Residual VSD, ASD, systemic-pulmonary collaterals
RV pressure overload from:
- RVOT obstruction or branch PA stenosis
- Pulmonary vascular disease
- Pulmonary venous hypertension (from LV diastolic dysfunction)
Other issues:
- RV systolic and diastolic dysfunction
- LV systolic and diastolic dysfunction
- Aortic root dilatation and aortic regurgitation
- Ventricular conduction delay and dyssynchrony
- Arrhythmias: Atrial flutter/fibrillation, ventricular tachycardia (VT)
Diagnostic Workup
| Modality | Role |
|---|---|
| Echocardiography | Screening for PR, RV dilatation, RVOT obstruction, TR severity, diastolic dysfunction, residual VSD; restrictive RV pattern (antegrade "a" wave in RVOT on pulse wave Doppler) |
| CMR (gold standard) | Accurate RV volume/function, PR quantification, RVOT aneurysm/akinesis, coronary proximity, ascending aorta size; late gadolinium enhancement (LGE) - correlates with adverse prognosis |
| Cardiopulmonary exercise testing | Objective exercise capacity - related to prognosis and guides valve replacement timing |
| CCT | Coronary artery relationships; RVOT calcification extent; pre-TPVI planning |
| Ambulatory ECG / EP study | Arrhythmia evaluation; inducible VT at EP study has prognostic value |
| Cardiac catheterization | Rarely needed for diagnostics alone; required for TOF with pulmonary atresia pre-operatively |
Indications for Pulmonary Valve Replacement (PVR)
Triggered by severe PR when:
- RV end-systolic volume index reaches 80 mL/m² or end-diastolic volume index reaches 160 mL/m² - these thresholds predict normalization of RV volume after intervention
- RV dysfunction
- Symptomatic patients
Transcatheter pulmonary valve implantation (TPVI): Option when RVOT and coronary anatomy are favorable. Patients with previous surgical PVR (homograft or xenograft) are usually suitable.
For RVOT obstruction:
- Symptomatic with severe obstruction → intervention indicated
- Asymptomatic → intervention based on objective exercise capacity, declining RV function, increasing TR, or significant RV-PA gradient
Arrhythmia Management
Atrial arrhythmias: Catheter ablation for symptomatic cases; pulmonary valve replacement may reduce substrate
Ventricular tachycardia (VT):
- Anatomical isthmuses can be targeted prophylactically by VT ablation (data on patient-specific risk stratification still evolving)
- VT ablation preferred in patients with good RV/LV function at expert centres
- ICD for secondary prevention in survivors of sustained VT or cardiac arrest
- Preoperative RV dysfunction and RVH confer ongoing risk even after PVR
Primary prevention ICD - considered in selected patients with multiple risk factors:
- LV dysfunction
- Non-sustained/symptomatic VT
- QRS duration ≥ 180 ms
- Extensive RV scarring on CMR
- Inducible VT at programmed electrical stimulation
- (Generally requires estimated mortality ≥3.5%/year)
Key AHA Scientific Statement (2024)
A recent AHA Scientific Statement on "Long-Term Management of Right Ventricular Outflow Tract Dysfunction in Repaired TOF" was published in Circulation (Dec 2024) - PMID 39569497 - providing updated guidance on RVOT management in this population.
Source: Braunwald's Heart Disease, 12th ed., Chapter 82 - Adult Congenital Heart Disease
How adult tof differs from peds tof
Finding Sources
Searching PubMed
"tetralogy of Fallot" AND adult AND "long-term outcomes"
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have rich content from both Braunwald's (adult TOF) and Rosen's/Harriet Lane (pediatric TOF). Let me compile a comprehensive comparison.
Adult TOF vs. Pediatric TOF: Key Differences
The core anatomy of TOF (VSD + RVOT obstruction + overriding aorta + RVH) is the same in both groups, but the clinical context, dominant problems, and management priorities differ substantially.
1. Clinical Context and Disease Phase
| Feature | Pediatric TOF | Adult TOF |
|---|---|---|
| Disease phase | Unrepaired or early post-repair | Almost always post-repair (>95%) |
| Main concern | Cyanosis, palliation, achieving repair | Long-term sequelae of repair |
| Physiology | Active right-to-left shunting across VSD | PR-dominant RV volume overload |
| Survival without treatment | Compatible with survival into childhood if mild; fatal if severe | Most adults have been repaired |
2. Presentation and Symptoms
| Feature | Pediatric TOF | Adult TOF |
|---|---|---|
| Cyanosis | Cardinal feature; degree depends on RVOT obstruction severity | Absent (normal SpO2 post-repair) |
| Clubbing | Present due to chronic hypoxemia | Typically absent |
| Polycythemia | Compensatory, common | Not a feature |
| "Pink TOF" | Mild obstruction - acyanotic infant | Not applicable |
| Exertional symptoms | Cyanotic spells during feeding/crying/exertion | Exertional dyspnoea, palpitations, syncope |
| Tet spells | Defining pediatric emergency (peak 2-4 months) | Do not occur post-repair |
| Squatting | Classic: child squats to increase SVR and reduce shunting | Not relevant |
3. The "Tet Spell" - Purely Pediatric
The hypercyanotic (tet) spell does not occur in adults. It is a pediatric emergency:
- Trigger: Crying, defecation, feeding - anything that suddenly drops SVR or causes tachycardia/hypovolemia
- Mechanism: Acute drop in SVR → massive R→L shunt → hypoxia → hyperpnea → increased venous return → worsening shunt (vicious cycle)
- Management (Harriet Lane / Rosen's):
- Knee-to-chest position (↑ SVR, ↓ shunting)
- 100% oxygen (limited benefit alone)
- Morphine 0.05-0.2 mg/kg or fentanyl 1 μg/kg (calms agitation, suppresses hyperpnea)
- Ketamine 1-2 mg/kg IV/IM (sedation + ↑ SVR)
- Phenylephrine 5-20 mcg/kg IV (α-agonist, ↑ SVR)
- Propranolol 0.15-0.25 mg/kg slow IV (↓ HR, ↑ ventricular filling)
- NaHCO₃ for acidosis
- Refractory → emergent surgery or palliation
In adults, this entire concept is irrelevant post-repair.
4. Investigations
| Investigation | Pediatric TOF | Adult TOF |
|---|---|---|
| Chest X-ray | Boot-shaped heart ("coeur en sabot"), decreased pulmonary vascular markings, possible right arch | Post-repair; RBBB pattern on ECG; CXR less specific |
| ECG | RVH + right axis deviation | Complete RBBB (from ventriculotomy/repair); QRS ≥180 ms = arrhythmia risk marker |
| Echocardiography | Delineates native anatomy, RVOT gradient, VSD, aortic override for surgical planning | Screens for PR severity, RV dilatation, RVOT obstruction, TR, diastolic dysfunction, restrictive RV physiology |
| CMR | Less central pre-operatively | Gold standard for RV volumes, PR quantification, RVOT aneurysm, LGE fibrosis mapping |
| Cardiopulmonary exercise test | Not typically used | Used for objective exercise capacity - guides PVR timing |
| EP study | Not relevant | Used for VT risk stratification; inducible VT has prognostic significance |
| BNP | Not a routine marker | Predictive of mortality |
5. Complications
| Complication | Pediatric | Adult |
|---|---|---|
| Pulmonary regurgitation | Minimal pre-repair; may arise early post-repair | Dominant long-term problem - progressive RV dilatation |
| RV volume overload | Not a primary concern | Central issue; drives intervention timing |
| Ventricular tachycardia / SCD | Rare | Major concern; driven by RVOT scar/fibrosis, QRS prolongation |
| Atrial arrhythmias | Uncommon | Atrial flutter/fibrillation from RA dilatation |
| Aortic root dilatation + AR | Occasionally noted | Significant long-term issue; aortic root may progressively enlarge |
| RV/LV dysfunction | Not typically present | Occurs after years of volume/pressure overload |
| RVOT aneurysm | Not present | Common in older adults after transannular patch repair |
| Residual VSD | Active target - surgical closure | Small residuals may persist; need surveillance |
6. Management Focus
| Domain | Pediatric TOF | Adult TOF |
|---|---|---|
| Primary goal | Achieve complete repair (VSD closure + RVOT reconstruction) | Manage long-term sequelae; timely re-intervention |
| Timing of repair | Early primary repair (ideally 3-6 months); earlier if severe cyanosis or tet spells | Repair already done; focus on pulmonary valve replacement (PVR) |
| Palliation | Blalock-Taussig-Thomas (BTT) shunt if anatomy unfavorable for early repair | Not applicable |
| Pulmonary valve replacement | Occasionally needed post-repair in childhood | Major indication: RV EDVi ≥160 mL/m², ESVi ≥80 mL/m², or RV dysfunction |
| Transcatheter PVI (TPVI) | Less common in children | Increasingly used in adults with favorable RVOT anatomy |
| ICD | Extremely rare | Indicated for secondary prevention (post-VT/VF); considered for primary prevention with multiple risk factors (QRS ≥180ms, inducible VT, extensive LGE, LV dysfunction) |
| Arrhythmia ablation | Rare | VT ablation targeting anatomical isthmuses; atrial ablation |
| Pregnancy counseling | Not applicable | Required (moderate-to-high risk; needs specialist ACHD centre) |
| Exercise restriction | Activity often limited pre-repair | Guided by RV function, PR severity, arrhythmia risk |
7. Summary Table
| Domain | Pediatric | Adult |
|---|---|---|
| Disease state | Unrepaired/early repair | Post-repair sequelae |
| Cyanosis | Yes (pre-repair) | No |
| Tet spells | Yes | No |
| ECG | RVH, RAD | RBBB; QRS duration matters |
| Key investigation | Echo for surgical planning | CMR for RV volumes + LGE |
| Dominant problem | RVOT obstruction, VSD, cyanosis | Pulmonary regurgitation → RV dilatation |
| Main intervention | Primary surgical repair | Pulmonary valve replacement (surgical or transcatheter) |
| Arrhythmia risk | Low | High (VT, AF/flutter, SCD) |
| ICD use | Rare | Defined indications |
Sources: Braunwald's Heart Disease 12e (ACHD chapter); Rosen's Emergency Medicine 9e; Harriet Lane Handbook 23e
Recent update: A 2025 review in Heart Failure Reviews (PMID 41351752) covers the evolving landscape from repair to right heart failure in TOF - directly relevant to the adult trajectory.
This is a shared conversation. Sign in to Orris to start your own chat.