Harrison's chapter 57 skin disease summary
Harrison's chapter 57 skin diseases overview approach to patient
skin disease classification morphology primary secondary lesions dermatology
eczema atopic dermatitis contact dermatitis seborrheic dermatitis treatment
psoriasis clinical features diagnosis management biologic therapy
Chapter 57 — Eczema, Psoriasis, Cutaneous Infections, Acne, and Other Common Skin Disorders
1. Eczema (Dermatitis)
Atopic Dermatitis (AD)
- Epidemiology: Most common chronic inflammatory skin disease; onset usually in childhood; strong association with asthma, allergic rhinitis, and food allergies (atopic triad).
- Pathogenesis: Th2-skewed immune response, defective skin barrier (filaggrin mutations), IgE elevation. IL-4, IL-13, and IL-31 are key cytokines.
- Clinical features:
- Infants: face, scalp, extensor surfaces
- Children/adults: flexural areas (antecubital and popliteal fossae), neck
- Lichenification, prurigo nodules in chronic disease
- Diagnosis: Clinical (Hanifin-Rajka criteria)
- Management:
- Emollients (cornerstone of therapy)
- Topical corticosteroids (first-line)
- Topical calcineurin inhibitors (tacrolimus, pimecrolimus) — steroid-sparing
- Dupilumab (anti-IL-4Rα) — FDA-approved for moderate-severe AD
- Oral antihistamines for pruritus
- Bleach baths to reduce S. aureus colonization
Contact Dermatitis
| Type | Mechanism | Examples |
|---|---|---|
| Irritant (ICD) | Non-immunologic, direct cytotoxic damage | Soaps, detergents, acids, alkalis |
| Allergic (ACD) | Type IV (delayed) hypersensitivity | Nickel, poison ivy (urushiol), latex, fragrances |
- Diagnosis: Patch testing for ACD
- Treatment: Identify/avoid trigger; topical corticosteroids; systemic corticosteroids for severe/widespread ACD
Seborrheic Dermatitis
- Greasy, yellowish scales on erythematous base in sebum-rich areas (scalp, nasolabial folds, eyebrows, central chest)
- Associated with Malassezia (lipophilic yeast) overgrowth
- In adults: dandruff; in infants: "cradle cap"
- Treatment: Antifungal shampoos (ketoconazole, selenium sulfide, zinc pyrithione); topical corticosteroids; topical calcineurin inhibitors
Dyshidrotic Eczema (Pompholyx)
- Vesicles on lateral fingers, palms, soles
- Triggers: stress, hyperhidrosis, metals
- Treatment: topical steroids, potassium permanganate soaks
Nummular Eczema
- Coin-shaped, pruritic, crusted plaques; common in elderly and dry climates
- Treatment: topical steroids, emollients
2. Psoriasis
- Prevalence: ~2% of the population worldwide; chronic, immune-mediated
- Pathogenesis: Th17/IL-17 and Th1/TNF-driven keratinocyte hyperproliferation; epidermal turnover ↑ (3–4 days vs. normal 28 days); HLA-Cw6 association
- Triggers: Stress, streptococcal infection (guttate), trauma (Koebner phenomenon), medications (lithium, beta-blockers, antimalarials, NSAIDs), HIV
Clinical Forms
| Type | Features |
|---|---|
| Plaque (Vulgaris) | Most common (90%); well-demarcated erythematous plaques with silvery scales; extensor surfaces, scalp, lumbosacral area |
| Guttate | Small "drop-like" lesions; young adults; post-streptococcal |
| Inverse | Flexural areas (axillae, groin, inframammary); minimal scale |
| Pustular | Sterile pustules; localized (palmoplantar) or generalized (von Zumbusch — medical emergency) |
| Erythrodermic | >90% BSA; medical emergency — thermoregulation and hemodynamic instability |
| Nail psoriasis | Pitting, oil spots, onycholysis, subungual hyperkeratosis |
| Psoriatic arthritis | Occurs in ~30%; inflammatory arthropathy (DIP involvement, pencil-in-cup deformity) |
Auspitz Sign
Management
- Corticosteroids
- Vitamin D analogues (calcipotriol)
- Retinoids (tazarotene)
- Calcineurin inhibitors (facial/intertriginous)
- Narrowband UVB (nbUVB) — preferred
- PUVA (psoralen + UVA)
| Drug | Mechanism | Notes |
|---|---|---|
| Methotrexate | Anti-folate, anti-inflammatory | Monitor LFTs, CBC |
| Cyclosporine | Calcineurin inhibitor | Short-term; nephrotoxic |
| Acitretin | Retinoid | Teratogenic; good for pustular/erythrodermic |
| Apremilast | PDE4 inhibitor | Oral; milder disease |
| Class | Drugs |
|---|---|
| Anti-TNF | Etanercept, infliximab, adalimumab |
| Anti-IL-12/23 (p40) | Ustekinumab |
| Anti-IL-17A | Secukinumab, ixekizumab |
| Anti-IL-17RA | Brodalumab |
| Anti-IL-23 (p19) | Guselkumab, risankizumab, tildrakizumab |
3. Cutaneous Infections
Bacterial
| Condition | Organism | Features | Treatment |
|---|---|---|---|
| Impetigo | S. aureus, S. pyogenes | Honey-colored crusted lesions; children | Mupirocin (topical); oral cephalexin or dicloxacillin |
| Folliculitis | S. aureus | Perifollicular pustules | Topical or oral antibiotics |
| Cellulitis | S. aureus, S. pyogenes | Spreading erythema, warmth, edema, no defined border | Oral/IV antibiotics based on severity |
| Erysipelas | S. pyogenes | Well-demarcated, raised erythema; facial or lower limb | Penicillin |
| Necrotizing fasciitis | Mixed or Group A Strep | Severe pain, systemic toxicity, "dishwater" drainage | Surgical debridement + broad-spectrum antibiotics |
| MRSA skin infections | S. aureus (MRSA) | Furuncles, carbuncles, abscesses | Drainage + TMP-SMX or doxycycline |
Fungal
| Condition | Organism | Features | Treatment |
|---|---|---|---|
| Tinea corporis | Dermatophytes | Annular, scaly plaques with central clearing | Topical azoles/terbinafine |
| Tinea pedis | Dermatophytes | Interdigital maceration, "moccasin" pattern | Topical antifungals |
| Tinea versicolor | Malassezia furfur | Hypo/hyperpigmented macules; trunk | Topical/oral azoles, selenium sulfide |
| Candidiasis | Candida spp. | Intertriginous, satellite lesions | Topical nystatin or azoles |
| Onychomycosis | Dermatophytes | Nail thickening, yellowing, subungual debris | Oral terbinafine or itraconazole |
Viral
| Condition | Organism | Features | Treatment |
|---|---|---|---|
| Herpes simplex | HSV-1, HSV-2 | Grouped vesicles on erythematous base; recurrent | Acyclovir, valacyclovir |
| Varicella-zoster (shingles) | VZV | Dermatomal vesicular eruption; post-herpetic neuralgia | Valacyclovir; steroids controversial |
| Molluscum contagiosum | Poxvirus | Umbilicated flesh-colored papules | Curettage, cantharidin; self-limited |
| Warts (verruca) | HPV | Hyperkeratotic papules; various types | Salicylic acid, cryotherapy |
4. Acne Vulgaris
- Pathogenesis: Four key factors — follicular hyperkeratosis, excess sebum, Cutibacterium acnes (formerly Propionibacterium acnes) colonization, inflammation
- Triggers: Androgens, occlusion, certain medications (steroids, lithium), cosmetics
Clinical Forms
| Type | Lesions |
|---|---|
| Comedonal | Open (blackheads), closed (whiteheads) |
| Inflammatory | Papules, pustules |
| Nodular/cystic | Deep nodules/cysts; risk of scarring |
Management (Stepwise)
| Severity | Treatment |
|---|---|
| Mild (comedonal) | Topical retinoids (tretinoin, adapalene) |
| Mild-moderate (inflammatory) | Topical retinoid + topical antibiotic (clindamycin) ± benzoyl peroxide |
| Moderate-severe | Add oral antibiotics (doxycycline, minocycline) |
| Severe/nodular | Oral isotretinoin (13-cis-retinoic acid) — most effective |
| Females | OCP, spironolactone (anti-androgen) |
Isotretinoin: Highly teratogenic (iPLEDGE program required); monitor triglycerides, LFTs; causes mucocutaneous dryness.
5. Rosacea
- Chronic facial condition: erythema, telangiectasias, papulopustules (no comedones), phymatous changes (rhinophyma), ocular rosacea
- Triggers: heat, sun, alcohol, spicy food, Demodex mites
- Management:
- Topical metronidazole, azelaic acid, ivermectin
- Oral doxycycline (sub-antimicrobial doses)
- Laser for telangiectasias; isotretinoin for severe phymatous disease
6. Other Common Disorders
Urticaria (Hives)
- Transient, pruritic wheals; angioedema may accompany
- Acute (<6 weeks): usually allergic/infectious; Chronic (>6 weeks): autoimmune or idiopathic
- Treatment: non-sedating antihistamines (cetirizine, loratadine); omalizumab for refractory chronic urticaria
Pityriasis Rosea
- Herald patch → widespread "Christmas tree" distribution on trunk
- Self-limiting (6–8 weeks); etiology linked to HHV-6/7
- Treatment: symptomatic; oral erythromycin or acyclovir may shorten course
Lichen Planus
- Pruritic, polygonal, purple, planar papules (6 P's); lacy white Wickham's striae in oral mucosa
- May be drug-induced (thiazides, antimalarials, beta-blockers)
- Treatment: topical/systemic corticosteroids; topical retinoids
Acanthosis Nigricans
- Velvety, hyperpigmented thickening in flexures (neck, axillae, groin)
- Strong association with insulin resistance, type 2 diabetes, obesity, internal malignancy (especially gastric adenocarcinoma when extensive/rapid onset)
Key Takeaways
- Eczema = impaired barrier + Th2 inflammation; dupilumab is transformative for moderate-severe AD
- Psoriasis = Th17-driven; biologic therapies (anti-IL-17, anti-IL-23) offer near-complete clearance
- Acne = isotretinoin is the most effective agent for severe disease; always counsel on teratogenicity
- Cutaneous infections require identifying organism type (bacterial/fungal/viral) to direct targeted therapy
- Common skin disorders frequently signal systemic disease (acanthosis nigricans → insulin resistance; extensive psoriasis → consider HIV)
Enlist all papulosquamous skin disorders, bullous and other disorders in classification
papulosquamous skin disorders classification complete list Harrison's
bullous skin disorders classification vesiculobullous diseases pemphigus pemphigoid
Harrison's skin manifestations internal disease vesicular bullous pustular table classification
Harrison's table selected causes vesicular bullous skin lesions classification systemic primary
Classification of Papulosquamous, Bullous, and Other Skin Disorders
I. PAPULOSQUAMOUS SKIN DISORDERS
A. Primary Cutaneous Disorders
- Psoriasis — widespread/resistant disease may indicate HIV infection
- Tinea (dermatophytosis) — widespread disease may indicate immunosuppression
- Pityriasis rosea
- Lichen planus
- Parapsoriasis
- Small plaque parapsoriasis
- Large plaque parapsoriasis
- Bowen's disease (squamous cell carcinoma in situ)
- Lichen simplex chronicus
- Seborrheic dermatitis
- Pityriasis rubra pilaris
- Ichthyosis vulgaris
B. Drug-Induced
- Drug-induced papulosquamous eruptions (lithium, beta-blockers, antimalarials, gold, NSAIDs)
C. Systemic Diseases
- Lupus erythematosus — primarily subacute or chronic (discoid) lesions
- Cutaneous T-cell lymphoma (CTCL) — in particular, mycosis fungoides
- Secondary syphilis
- Reactive arthritis (formerly Reiter's syndrome) — keratoderma blennorrhagica
- Sarcoidosis — with scale less common than without scale
- Bazex syndrome (acrokeratosis paraneoplastica)
II. BULLOUS (VESICULOBULLOUS) SKIN DISORDERS
A. Primary Cutaneous Disorders
Intraepidermal (Suprabasal / Subcorneal)
- Pemphigus vulgaris — suprabasal split; anti-desmoglein 1 & 3 IgG
- Pemphigus foliaceus — subcorneal split; anti-desmoglein 1 IgG
- Pemphigus erythematosus (localized form of pemphigus foliaceus)
- Pemphigus vegetans
- IgA pemphigus
- Paraneoplastic pemphigus
Subepidermal
- Bullous pemphigoid — most common autoimmune blistering disease; anti-BP180 & BP230 IgG; affects elderly
- Mucous membrane pemphigoid (cicatricial pemphigoid) — anti-BP180, laminin-332
- Pemphigoid gestationis (herpes gestationis) — pregnancy-associated
- Dermatitis herpetiformis — IgA deposits at dermal papillae; associated with celiac disease; anti-endomysial/tissue transglutaminase antibodies
- Linear IgA bullous dermatosis (LABD) — IgA at BMZ; drug-induced (vancomycin) or idiopathic
- Epidermolysis bullosa acquisita (EBA) — anti-type VII collagen
- Anti-p200 pemphigoid
Genetic/Inherited
- Epidermolysis bullosa (EB) — simplex, junctional, dystrophic subtypes
Infectious
- Bullous impetigo — S. aureus (exfoliative toxin)
- Staphylococcal scalded skin syndrome (SSSS)
- Herpes simplex — grouped vesicles
- Varicella-zoster / Herpes zoster — dermatomal vesicles
- Hand-foot-mouth disease — Coxsackievirus A16
Contact/Irritant
- Bullous contact dermatitis (e.g., poison ivy, strong irritants)
B. Systemic Diseases Causing Bullae
- Porphyria cutanea tarda — photodistributed bullae on dorsal hands; uroporphyrinogen decarboxylase deficiency
- Diabetic bullae (bullosis diabeticorum)
- Systemic lupus erythematosus — bullous LE (anti-type VII collagen)
- Erythema multiforme — targetoid lesions ± bullae; HSV or drug-triggered
- Stevens-Johnson syndrome (SJS) — <10% BSA epidermal detachment; drug-induced
- Toxic epidermal necrolysis (TEN) — >30% BSA; full-thickness epidermal necrosis; drug-induced
III. OTHER NOTABLE DISORDER CLASSIFICATIONS (Harrison's Framework)
A. Eczematous Disorders
- Atopic dermatitis
- Irritant contact dermatitis
- Allergic contact dermatitis
- Seborrheic dermatitis
- Nummular eczema
- Dyshidrotic eczema (pompholyx)
- Stasis dermatitis
B. Pustular Disorders
- Acne vulgaris
- Rosacea
- Folliculitis
- Pustular psoriasis (localized palmoplantar / generalized von Zumbusch)
- Disseminated gonococcal infection
- Viral pustular eruptions
C. Urticarial/Reactive Disorders
- Urticaria (acute and chronic)
- Angioedema
- Erythema multiforme
- Erythema nodosum (panniculitis)
- Pityriasis rosea
D. Hyperpigmented / Hypopigmented Disorders
- Acanthosis nigricans
- Vitiligo
- Melasma
- Post-inflammatory hyperpigmentation
- Pityriasis versicolor
E. Vascular / Purpuric Disorders
- Leukocytoclastic vasculitis
- Henoch-Schönlein purpura
- Livedo reticularis
- Purpura fulminans
Summary Table
| Category | Mechanism | Key Examples |
|---|---|---|
| Papulosquamous | Epidermal hyperproliferation + scale | Psoriasis, lichen planus, tinea, mycosis fungoides |
| Intraepidermal bullous | Loss of keratinocyte adhesion (acantholysis) | Pemphigus vulgaris, pemphigus foliaceus |
| Subepidermal bullous | Autoimmune attack at BMZ | Bullous pemphigoid, dermatitis herpetiformis, EBA |
| Infectious bullous | Toxin-mediated or direct viral | Bullous impetigo, SSSS, HSV, VZV |
| Drug/reactive bullous | Cytotoxic T-cell epidermal destruction | SJS, TEN |
| Metabolic/systemic bullous | Porphyrin photosensitization, ischemia | PCT, diabetic bullae |
Metabolic causes of hyperpigmentation
metabolic causes hyperpigmentation skin disorders
hyperpigmentation Addison's disease hemochromatosis porphyria acanthosis nigricans metabolic endocrine
porphyria cutanea tarda hemochromatosis pellagra hyperpigmentation skin mechanism
Whipple's disease vitamin B12 deficiency folate malabsorption skin hyperpigmentation features
Metabolic Causes of Hyperpigmentation
Full Classification Context — Diffuse Hyperpigmentation
| Category | Conditions |
|---|---|
| Endocrinopathies | Addison's disease, Nelson syndrome, Ectopic ACTH syndrome, Hyperthyroidism |
| Metabolic | PCT, Hemochromatosis, Vit B₁₂/Folate deficiency, Pellagra, Malabsorption (incl. Whipple's) |
| Melanosis | Secondary to metastatic melanoma |
| Autoimmune | Primary biliary cholangitis, Systemic sclerosis, POEMS syndrome, Eosinophilia-myalgia syndrome |
| Drugs/Metals | Cyclophosphamide, silver (argyria), amiodarone, minocycline |
Metabolic Causes — Detailed
1. Porphyria Cutanea Tarda (PCT)
- Defect: Uroporphyrinogen decarboxylase deficiency → accumulation of porphyrins
- Mechanism of pigmentation: Porphyrins are photoreactive — UV light activates accumulated porphyrins → reactive oxygen species → melanocyte stimulation → hyperpigmentation
- Distribution: Sun-exposed areas (face, dorsal hands, forearms)
- Associated features: Photodistributed bullae, skin fragility, milia, hypertrichosis (especially facial)
- Associations: Hepatitis C, alcohol, estrogens, iron overload, HIV
2. Hemochromatosis (Type 1)
- Defect: HFE gene mutation → excess iron deposition in tissues
- Mechanism: Elevated iron in the skin directly stimulates melanin pigment production by melanocytes
- Classic appearance: "Bronze diabetes" — generalised bronze/grey-brown discolouration
- Distribution: Diffuse, most prominent in sun-exposed areas, genitalia, old scars
- Associated features: Liver cirrhosis, diabetes mellitus, cardiomyopathy, hypogonadism, arthropathy
3. Pellagra (Niacin / Nicotinic Acid Deficiency)
- Defect: Vitamin B₃ (niacin) deficiency — dietary, or secondary to:
- Vitamin B₆ deficiency (needed for tryptophan → niacin conversion)
- Functioning carcinoid tumors (excess tryptophan consumed for serotonin → niacin depleted)
- Isoniazid therapy (inhibits B₆)
- Hartnup disease (impaired tryptophan absorption)
- Mechanism: Niacin is essential for NAD/NADP redox reactions; deficiency → impaired DNA repair in UV-exposed skin → inflammatory pigmentation
- Appearance: Brown discolouration with a thin, varnish-like scale
- Distribution: Sun-exposed areas — classic "Casal's necklace" on the neck
- Classic triad: Dermatitis, Diarrhoea, Dementia ("3 Ds")
4. Vitamin B₁₂ Deficiency
- Mechanism: B₁₂ is required for melanin synthesis regulation; deficiency → increased melanin production, possibly via decreased inhibition of tyrosinase
- Appearance: Diffuse hyperpigmentation, often accentuated on knuckles, palmar creases, oral mucosa, nail beds (longitudinal melanonychia)
- Associated features: Megaloblastic anaemia, subacute combined degeneration of the cord, glossitis
5. Folic Acid (Folate) Deficiency
- Mechanism: Similar to B₁₂ — folate participates in one-carbon metabolism affecting melanin pathway; deficiency disrupts this balance
- Appearance: Diffuse hyperpigmentation; can mimic B₁₂ deficiency skin changes
- Associated features: Megaloblastic anaemia, neural tube defects (in pregnancy)
6. Malabsorption Syndromes (including Whipple's Disease)
- Whipple's disease: ~50% of patients have associated hyperpigmentation
- Caused by Tropheryma whipplei
- Malabsorption → combined niacin, B₁₂, and folate deficiencies → pigmentation
- Other features: diarrhoea, arthralgias, weight loss, lymphadenopathy, CNS involvement
- Other malabsorption states (Crohn's, celiac, short bowel syndrome) → nutrient deficiencies → similar pigmentary changes
Summary Table
| Condition | Mechanism | Distribution | Key Clue |
|---|---|---|---|
| PCT | Photoreactive porphyrins → melanocyte stimulation | Sun-exposed | Bullae + hypertrichosis + fragile skin |
| Hemochromatosis | Iron deposition → ↑ melanin production | Diffuse, bronze | Bronze skin + diabetes + cirrhosis |
| Pellagra | Niacin deficiency → impaired UV-damaged skin repair | Sun-exposed + Casal's necklace | Varnish-like scale; 3 Ds |
| Vit B₁₂ deficiency | Dysregulation of melanin synthesis | Knuckles, mucosa, nails | Megaloblastic anaemia + neurological signs |
| Folate deficiency | One-carbon metabolism disruption | Diffuse | Megaloblastic anaemia; no neuro signs |
| Whipple's / Malabsorption | Combined nutritional deficiencies | Diffuse | Diarrhoea + arthralgias + weight loss |
Role of peripheral blood smear in systemic diseases with examples of abnormal findings. Harrison's chapter 62
peripheral blood smear systemic diseases Harrison's chapter 62
abnormal red blood cell morphology blood smear findings systemic disease schistocytes spherocytes
peripheral blood smear white blood cell abnormalities leukemia lymphoma neutrophil platelet findings
blood smear rouleaux formation target cells sickle cells Howell-Jolly bodies malaria parasites findings
Peripheral Blood Smear in Systemic Diseases
Harrison's Principles of Internal Medicine, 21st Edition — Chapter 62
"Every internist should know how to examine a peripheral blood smear." — Harrison's, p. 1714
Why the Peripheral Blood Smear Matters
I. RED BLOOD CELL (RBC) ABNORMALITIES
A. Size Abnormalities
| Finding | Description | Associated Conditions |
|---|---|---|
| Microcytes | Small RBCs (MCV <80 fL) | Iron deficiency anaemia, thalassaemia, anaemia of chronic disease, sideroblastic anaemia |
| Macrocytes | Large RBCs (MCV >100 fL) | Vitamin B₁₂/folate deficiency, liver disease, hypothyroidism, MDS, medications (hydroxyurea, methotrexate) |
| Megalocytes | Oval macrocytes | Megaloblastic anaemia (B₁₂/folate deficiency) |
| Anisocytosis | Variable RBC size | Non-specific; seen in mixed deficiencies, haemolytic anaemia, MDS |
B. Shape Abnormalities (Poikilocytosis)
| Cell | Morphology | Disease Association |
|---|---|---|
| Schistocytes | Helmet-shaped cell fragments | Microangiopathic haemolytic anaemia (MAHA): TTP, HUS, DIC, malignant hypertension, eclampsia; also prosthetic heart valves |
| Spherocytes | Round, dense, no central pallor | Hereditary spherocytosis, autoimmune haemolytic anaemia (AIHA), ABO incompatibility transfusion reactions, burns |
| Sickle cells (Drepanocytes) | Elongated, crescent-shaped | Sickle cell disease (HbSS, HbSC) |
| Target cells (Codocytes) | Central density + peripheral ring ("bull's eye") | Liver disease, obstructive jaundice, thalassaemia, HbC disease, iron deficiency, post-splenectomy |
| Dacrocytes | Teardrop-shaped | Myelofibrosis (classic), severe iron deficiency, thalassaemia, haemolytic anaemia, MDS |
| Elliptocytes | Oval/elliptical | Hereditary elliptocytosis, iron deficiency, megaloblastic anaemia, thalassaemia, MDS |
| Acanthocytes | Irregular spicules (unevenly distributed) | Abetalipoproteinaemia, chronic renal disease, post-splenectomy, liver disease — irreversible |
| Echinocytes (Burr cells) | Evenly distributed spicules | Uraemia (renal failure), malnutrition, stored blood artefact — often reversible |
| Stomatocytes | Mouth-like (slit) central pallor | Hereditary stomatocytosis, liver disease (especially alcoholic), Rh-null disease |
| Rouleaux | RBCs stacked like coins | Multiple myeloma, Waldenström's macroglobulinaemia, chronic inflammation (elevated fibrinogen/globulins) |
C. Colour / Staining Abnormalities
| Finding | Description | Associated Conditions |
|---|---|---|
| Hypochromia | Increased central pallor (>1/3 diameter) | Iron deficiency anaemia, thalassaemia, sideroblastic anaemia |
| Polychromasia | Blue-grey tint (reticulocytes) | Active haemolysis, haemorrhage with compensatory erythropoiesis, bone marrow recovery |
| Hyperchromia | Dense staining (spherocytes, not truly hyperchromic) | Seen with spherocytes |
D. Inclusions Within RBCs
| Inclusion | Stain | Significance |
|---|---|---|
| Howell-Jolly bodies | Wright's stain — dark purple dots | Hyposplenism / Post-splenectomy, megaloblastic anaemia, severe haemolytic anaemia |
| Basophilic stippling | Coarse blue dots (aggregated ribosomes) | Lead poisoning, thalassaemia, MDS, sideroblastic anaemia, pyrimidine 5'-nucleotidase deficiency |
| Pappenheimer bodies | Iron-containing granules (Prussian blue +) | Sideroblastic anaemia, haemolytic anaemia, post-splenectomy |
| Heinz bodies | Denatured Hb (supravital stain only) | G6PD deficiency, unstable haemoglobinopathies, oxidant drug toxicity |
| Cabot rings | Ring/figure-8 nuclear remnants | Megaloblastic anaemia, severe dyserythropoiesis |
| Malaria parasites | Ring forms, trophozoites, gametocytes | Plasmodium spp. — species identification critical for treatment |
| Babesia | "Maltese cross" (tetrad form) | Babesiosis — Babesia microti |
II. WHITE BLOOD CELL (WBC) ABNORMALITIES
A. Quantitative Changes
| Finding | Conditions |
|---|---|
| Leukocytosis | Infection, leukaemia, steroids, stress response, malignancy |
| Leukopenia | Viral infections, bone marrow failure, SLE, drug toxicity, hypersplenism |
| Eosinophilia | Allergic/atopic disease, parasitic infections, drug reactions, eosinophilic granulomatosis with polyangiitis (EGPA), Addison's disease, malignancy |
| Basophilia | CML (hallmark), myeloproliferative neoplasms, hypothyroidism |
| Monocytosis | TB, infective endocarditis, CMML, inflammatory bowel disease |
| Lymphocytosis | Viral infections (EBV, CMV), CLL, pertussis |
B. Morphological WBC Abnormalities
| Finding | Description | Associated Conditions |
|---|---|---|
| Hypersegmented neutrophils | Neutrophil with ≥5 lobes (or single cell with ≥6 lobes) | Megaloblastic anaemia (B₁₂/folate deficiency) — classic finding |
| Left shift (bands, metamyelocytes) | Immature neutrophils in peripheral blood | Severe bacterial infection, leukaemoid reaction, CML |
| Toxic granulation | Coarse dark granules in neutrophils | Severe bacterial sepsis, inflammatory states |
| Döhle bodies | Blue cytoplasmic inclusions in neutrophils | Sepsis, burns, pregnancy, May-Hegglin anomaly |
| Pelger-Huët anomaly | Bilobed "pince-nez" neutrophils | Inherited or pseudo-Pelger-Huët in MDS — important marker |
| Blast cells | Large cells with prominent nucleoli, high N:C ratio | Acute leukaemia (AML/ALL) — medical emergency |
| Smudge (basket) cells | Fragile lymphocytes smeared on slide | CLL — pathognomonic finding |
| Atypical lymphocytes | Large, irregular, abundant cytoplasm | EBV (infectious mononucleosis), CMV, viral hepatitis |
| Auer rods | Pink needle-like cytoplasmic inclusions | AML — pathognomonic (especially AML-M3/APL) |
| Leukoerythroblastic picture | Immature WBCs + nucleated RBCs together | Myelophthisic anaemia: myelofibrosis, bone marrow infiltration (metastatic cancer, TB, lymphoma) |
III. PLATELET ABNORMALITIES
| Finding | Description | Associated Conditions |
|---|---|---|
| Thrombocytopenia | Decreased platelets on smear | ITP, TTP, HUS, DIC, hypersplenism, bone marrow failure, heparin-induced (HIT) |
| Thrombocytosis | Increased platelets | Essential thrombocythaemia, reactive (infection, post-splenectomy, iron deficiency) |
| Giant platelets | Platelets ≥ RBC size | Bernard-Soulier syndrome, MDS, May-Hegglin anomaly, ITP |
| Platelet clumping | Artefactual aggregation | EDTA-induced pseudothrombocytopenia — must verify with citrate tube |
| Schistocytes + thrombocytopenia | Combined finding | TTP (ADAMTS13 deficiency) / HUS / DIC — diagnostic pentad in TTP |
IV. SYSTEMIC DISEASES — PBS Correlation Summary
| Systemic Disease | Key PBS Findings |
|---|---|
| Iron deficiency anaemia | Microcytes, hypochromia, elliptocytes, target cells |
| B₁₂/Folate deficiency | Macro-ovalocytes, hypersegmented neutrophils, pancytopenia |
| Thalassaemia | Microcytes, hypochromia, target cells, basophilic stippling, nucleated RBCs |
| Sickle cell disease | Sickle cells, target cells, Howell-Jolly bodies (functional asplenia), nucleated RBCs |
| Autoimmune haemolytic anaemia | Spherocytes, polychromasia, nucleated RBCs |
| TTP / HUS | Schistocytes + thrombocytopenia + polychromasia |
| DIC | Schistocytes, thrombocytopenia, fibrin thrombi evidence |
| Malaria | Intra-RBC ring forms / trophozoites / gametocytes (species-specific morphology) |
| CLL | Lymphocytosis + smudge cells |
| CML | Left shift, basophilia, eosinophilia, all myeloid stages visible |
| AML | Blasts + Auer rods (AML-M3) |
| Multiple myeloma | Rouleaux formation, normochromic normocytic anaemia, background blue staining (hyperproteinaemia) |
| Myelofibrosis | Dacrocytes (teardrops), leukoerythroblastic picture |
| Lead poisoning | Basophilic stippling, microcytic anaemia |
| Hyposplenism/Post-splenectomy | Howell-Jolly bodies, target cells, Pappenheimer bodies, thrombocytosis |
| Liver disease | Target cells, acanthocytes, stomatocytes, macrocytes, thrombocytopenia |
| Renal failure (uraemia) | Echinocytes (burr cells), normochromic normocytic anaemia |
| MDS | Pseudo-Pelger-Huët, hypogranular neutrophils, macrocytosis, hypolobated megakaryocytes |
| G6PD deficiency | Heinz bodies (supravital stain), bite cells, polychromasia after oxidant stress |
Key Teaching Points (Harrison's, p. 1714)
- PBS is indispensable — automated analysers miss morphological detail
- Always examine the feathered edge of the smear (optimal RBC distribution)
- Findings in PBS must be interpreted alongside the clinical context and CBC
- Leukoerythroblastic picture on PBS = bone marrow infiltration until proven otherwise — warrants bone marrow biopsy
- Schistocytes on PBS in the right clinical context = haematological emergency (TTP/HUS/DIC)
- Hypersegmented neutrophils may be the earliest finding in megaloblastic anaemia, preceding macrocytosis
Psuedotumor cerebri
pseudotumor cerebri idiopathic intracranial hypertension etiology pathophysiology causes
pseudotumor cerebri diagnosis criteria clinical features headache papilledema visual loss management treatment
idiopathic intracranial hypertension modified Dandy criteria lumbar puncture CSF opening pressure MRI findings empty sella
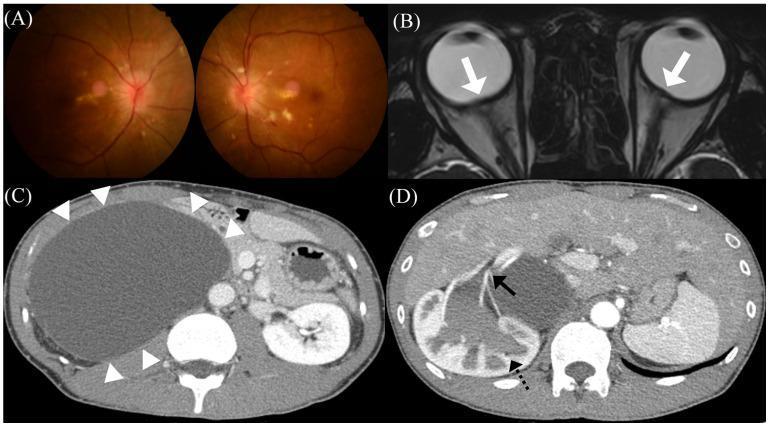
pseudotumor cerebri papilledema optic disc swelling MRI findings
Pseudotumor Cerebri (Idiopathic Intracranial Hypertension)
Definition & Nomenclature
The term "benign" is now discouraged because up to 25% of patients suffer permanent visual loss.
Epidemiology
| Parameter | Details |
|---|---|
| Overall incidence | ~1 per 100,000 in the general US population |
| High-risk group | Women aged 20–44 with obesity: 15–19 per 100,000 |
| Sex ratio | Almost exclusively female (F:M ≈ 9:1) |
| Peak age | Reproductive years (20s–40s) |
| Obesity | Present in >90% of affected women; strong independent risk factor |
| Paediatric IIH | Associated with obesity; higher incidence in post-pubertal adolescents than prepubertal children |
Etiology & Risk Factors
A. Obesity & Hormonal
- Obesity — most significant modifiable risk factor (mechanism possibly related to increased intra-abdominal pressure → elevated venous pressure → impaired CSF absorption)
- Weight gain — even modest increases can precipitate IIH
- Pregnancy
- Polycystic ovarian syndrome (PCOS)
B. Drugs & Medications
| Drug Category | Examples |
|---|---|
| Tetracyclines | Tetracycline, minocycline, doxycycline |
| Vitamin A / Retinoids | Hypervitaminosis A, isotretinoin (Accutane), all-trans retinoic acid |
| Corticosteroids | Steroid withdrawal (not initiation) |
| Hormonal | OCP, levonorgestrel (Mirena IUD) |
| Others | Growth hormone, lithium, nalidixic acid, nitrofurantoin, cyclosporine |
C. Systemic / Metabolic Conditions
- Addison's disease (adrenal insufficiency)
- Hypoparathyroidism
- Severe anaemia (especially iron deficiency)
- Sleep apnoea
- Chronic kidney disease
D. Venous Sinus Pathology
- Cerebral venous sinus thrombosis (most important secondary cause)
- Bilateral internal jugular vein obstruction
- Superior vena cava syndrome
- Arteriovenous malformations
Pathophysiology
- Impaired CSF absorption at arachnoid granulations (most favoured)
- Increased CSF production (acetazolamide lowers ICP by reducing this)
- Venous hypertension → elevated venous sinus pressure → impaired CSF outflow → raised ICP
- Transverse sinus stenosis is found in >90% of IIH patients (may be cause or consequence)
- Obesity-related mechanisms: Increased intra-abdominal and intrathoracic pressure → elevated cerebral venous pressure → raised ICP; adipose tissue may also produce hormones (adipokines) that alter CSF dynamics
Clinical Features
Symptoms
| Symptom | Details |
|---|---|
| Headache | Most common (>90%); daily, diffuse, worse on waking, with Valsalva, positional; migraine-like in character |
| Transient visual obscurations (TVOs) | Seconds-long monocular or binocular visual greyouts, often provoked by postural change — highly characteristic |
| Pulsatile tinnitus | "Whooshing" or heartbeat-like sound in the ears — very characteristic |
| Diplopia | Usually due to unilateral or bilateral VI (abducens) nerve palsy (false localising sign of raised ICP) |
| Photophobia / Phonophobia | Common |
| Visual loss | Progressive if untreated — the most feared complication |
| Neck/back pain | From raised CSF pressure radiating down the spinal axis |
Signs
| Sign | Details |
|---|---|
| Papilledema | Cardinal sign — bilateral optic disc swelling from raised ICP; may be asymmetric |
| VI nerve palsy | Esotropia with inability to abduct the eye — false localising sign |
| Visual field defects | Enlarged blind spot (earliest); inferior nasal quadrant loss progressing to generalised constriction |
| Reduced visual acuity | Late and serious — indicates optic nerve compromise |
Note: Neurological examination is otherwise normal — no focal deficits, no altered consciousness, no meningism (which differentiates it from intracranial mass/meningitis)
Diagnostic Criteria (Modified Dandy Criteria / Friedman & Jacobson 2013)
- Signs/symptoms of raised ICP (headache, papilledema, TVOs, diplopia)
- No other neurological abnormality (excluding CN VI palsy)
- Neuroimaging: Normal brain parenchyma, no hydrocephalus, no mass lesion, no structural cause; MRI may show IIH-specific features (see below)
- Normal CSF composition (cell count, protein, glucose)
- Elevated CSF opening pressure:
- ≥25 cmH₂O in adults (measured in lateral decubitus position)
- ≥28 cmH₂O in children
- 20–25 cmH₂O = borderline (requires additional supportive features)
- No other cause identified for raised ICP
"An elevated pressure, with normal cerebrospinal fluid, points by exclusion to the diagnosis of pseudotumor cerebri." — Harrison's, p. 964
Investigations
1. Neuroimaging (MRI Brain ± MRV)
| Finding | Significance |
|---|---|
| Empty sella | Flattening of pituitary from chronically raised ICP |
| Posterior globe flattening | Pressure transmitted to optic nerve sheath → flattens posterior sclera |
| Optic nerve sheath distension | Dilation >5 mm reflects raised ICP in perioptic subarachnoid space |
| Transverse sinus stenosis | Present in >90%; bilateral; seen on MRV |
| Vertical tortuosity of optic nerve | Undulation of the optic nerve due to raised ICP |
| Enlarged Meckel's cave / empty sella | Sign of chronic pressure elevation |
2. Lumbar Puncture
- Must be done in lateral decubitus position (sitting position falsely elevates pressure)
- Measure opening pressure (normal <20 cmH₂O)
- Send CSF for cell count, protein, glucose, culture — will be normal in IIH
- LP is both diagnostic and temporarily therapeutic (symptom relief after CSF removal)
3. Ophthalmological Assessment
- Fundoscopy: Grade papilledema (Frisén scale 0–5)
- Visual field testing (perimetry): Humphrey visual fields — enlarged blind spot, arcuate defects
- OCT (Optical Coherence Tomography): Measures retinal nerve fibre layer (RNFL) thickness — objective monitoring of papilledema and optic nerve damage
- Visual acuity: Snellen chart
Imaging Illustration
Management
Step 1: Treat Underlying Cause
- Stop offending drugs (tetracyclines, retinoids, steroids)
- Treat venous sinus thrombosis if present
- Correct endocrine/metabolic disorders
Step 2: Weight Loss (Cornerstone)
- 5–10% body weight reduction significantly lowers ICP and improves symptoms
- Bariatric surgery: Indicated in patients who cannot achieve adequate weight loss through diet — highly effective (Harrison's, p. 964)
Step 3: Medical Therapy
| Drug | Mechanism | Dose | Notes |
|---|---|---|---|
| Acetazolamide | Carbonic anhydrase inhibitor → ↓ CSF production | 1–4 g/day | First-line; improves visual fields (IIHTT trial); monitor electrolytes, renal stones |
| Topiramate | Carbonic anhydrase inhibitor + aids weight loss | 50–200 mg/day | Second-line; useful if headache predominates |
| Furosemide | Loop diuretic → ↓ CSF production | 20–40 mg/day | Adjunctive to acetazolamide |
| Corticosteroids | ↓ Inflammation, ↓ CSF production | Short course only | Used in fulminant IIH with acute vision loss; avoid long-term (causes obesity, rebound) |
Step 4: Repeated Lumbar Punctures
- Temporary relief; not a long-term solution
- Used in pregnancy (where medications may be limited) and acute severe cases
Step 5: Surgical Interventions
| Procedure | Indication | Notes |
|---|---|---|
| CSF shunting (LP shunt or VP shunt) | Severe or progressive vision loss | Most effective for vision preservation; shunt failure/revision common (Harrison's, p. 964) |
| Optic nerve sheath fenestration (ONSF) | Threatened vision, especially unilateral | Protects ipsilateral optic nerve; does not address headache; less effective overall (Harrison's, p. 964) |
| Dural venous sinus stenting | Bilateral transverse sinus stenosis + high venous pressure gradient | Emerging therapy; stent placed at transverse-sigmoid sinus junction; promising results (Harrison's, p. 964) |
Complications
| Complication | Details |
|---|---|
| Permanent visual loss / blindness | Most feared; up to 25% of patients; due to optic nerve atrophy from chronic papilledema |
| Chronic daily headache | Most common long-term morbidity |
| Optic atrophy | End-stage of untreated papilledema |
| CSF rhinorrhoea | Spontaneous CSF leak through cribriform plate — associated with empty sella and high ICP |
| Shunt complications | Obstruction, infection, over-drainage (subdural hematoma) |
Special Populations
Pregnancy
- IIH may worsen due to weight gain and hormonal changes
- Acetazolamide is relatively contraindicated in first trimester (teratogenic in animals)
- Serial LP and ONSF are preferred during pregnancy
- Delivery route not affected by IIH alone
Paediatric IIH
- Prepubertal children: more equal sex ratio, less associated with obesity
- Post-pubertal adolescents: epidemiology mirrors adults (female, obese)
- Must exclude all secondary causes rigorously
Summary Algorithm
Suspected IIH (headache + papilledema + obese young woman)
↓
MRI Brain + MRV → exclude mass, hydrocephalus, CVT
↓
Lumbar Puncture (lateral decubitus) → elevated opening pressure + normal CSF
↓
Ophthalmology referral → grade papilledema, visual fields, OCT
↓
Mild-moderate disease Severe/rapid visual loss
↓ ↓
Weight loss + Acetazolamide Urgent shunting / ONSF / stenting
↓
Monitor visual fields every 1–3 months
↓
If no improvement → add topiramate / consider surgery
Harrison's chapter 37 dyspnea summary
Harrison's chapter 37 dyspnea pathophysiology mechanisms afferent signals
dyspnea etiology causes cardiac pulmonary evaluation diagnosis management Harrison's
dyspnea assessment MRC scale quality descriptors air hunger chest tightness work of breathing
dyspnea acute chronic differential diagnosis heart failure COPD pulmonary embolism anemia treatment
Chapter 37 — Dyspnea
Harrison's Principles of Internal Medicine, 21st Edition
Definition
Dyspnea differs from tachypnea (increased respiratory rate) and hyperpnea (increased ventilation) — it is fundamentally a subjective perception, not an objective measurement.
Pathophysiology
Neural Framework — Afferent Signals
1. Chemoreceptors
| Receptor | Location | Stimulus | Sensation Produced |
|---|---|---|---|
| Peripheral chemoreceptors | Carotid body, aortic arch | Hypoxaemia (↓PaO₂), hypercapnia, acidaemia | Air hunger |
| Central chemoreceptors | Medulla oblongata | Hypercapnia (↑PaCO₂), CSF acidosis | Air hunger / urge to breathe |
2. Mechanoreceptors
| Receptor | Location | Activated By | Sensation |
|---|---|---|---|
| Stretch receptors | Lungs (airways/parenchyma) | Lung inflation/deflation | Modulates respiratory effort sensation |
| Irritant receptors | Bronchial epithelium | Chemical irritants, bronchoconstriction | Chest tightness (e.g., asthma, COPD) |
| J receptors (juxtacapillary) | Lung interstitium/alveoli | Pulmonary congestion, oedema, inflammation | Rapid, shallow breathing; dyspnea |
| Muscle spindles | Respiratory muscles, chest wall | Increased work/load (↑airway resistance, ↓compliance) | Work/effort of breathing |
| Tendon organs | Respiratory muscles | Force generation monitoring | Effort sensation |
3. Additional Afferent Sources
- Pulmonary vascular receptors: Respond to changes in pulmonary artery pressure
- Skeletal muscle metaboreceptors: Activated during exercise; contribute to exertional dyspnea
- Upper airway receptors: Cold air, irritants → modify dyspnea perception
4. Efferent–Afferent Mismatch ("Neuromechanical Dissociation")
- Neuromuscular weakness (high drive, low output)
- Severe airflow obstruction (high drive, high resistance)
- Reduced lung compliance (high drive, stiff lungs)
Qualitative Descriptors of Dyspnea
| Descriptor | Likely Mechanism | Associated Conditions |
|---|---|---|
| "Air hunger" / "cannot get enough air" | Chemoreceptor activation (hypoxaemia, hypercapnia) | Heart failure, PE, severe anaemia, COPD exacerbation |
| "Chest tightness" | Airway mechanoreceptors (bronchoconstriction) | Asthma, COPD |
| "Increased work/effort of breathing" | Muscle spindle activation (high resistance or low compliance) | COPD, pulmonary fibrosis, chest wall deformity |
| "Cannot take a deep breath" / "unsatisfying breath" | Cortical/psychological origin | Anxiety, hyperventilation syndrome, vocal cord dysfunction |
| "Suffocating" | Mixed — severe hypoxaemia + high respiratory drive | Pulmonary oedema, severe asthma |
Etiology — Causes of Dyspnea
Acute Dyspnea (minutes to hours)
| Category | Causes |
|---|---|
| Cardiac | Acute decompensated heart failure (pulmonary oedema), acute MI, cardiac tamponade, acute arrhythmia |
| Pulmonary | Acute severe asthma, COPD exacerbation, pulmonary embolism, pneumothorax, pneumonia |
| Upper airway | Anaphylaxis (laryngeal oedema), foreign body obstruction, epiglottitis, angioedema |
| Metabolic | Severe metabolic acidosis (DKA, lactic acidosis), sepsis |
| Neuromuscular | Guillain-Barré syndrome (acute), myasthenic crisis |
| Psychogenic | Panic attack, acute hyperventilation syndrome |
Chronic / Subacute Dyspnea (weeks to months)
| Category | Causes |
|---|---|
| Cardiac | Heart failure (HFrEF, HFpEF), valvular heart disease, constrictive pericarditis, cardiomyopathy |
| Pulmonary | COPD, asthma, interstitial lung disease (ILD/pulmonary fibrosis), pulmonary hypertension, bronchiectasis, pleural effusion |
| Haematological | Anaemia (any cause) |
| Neuromuscular | ALS, myasthenia gravis, diaphragmatic paralysis, Duchenne muscular dystrophy |
| Deconditioning | Obesity, physical deconditioning |
| Psychogenic | Anxiety disorder, depression, chronic hyperventilation |
| Others | Thyrotoxicosis, pregnancy, ascites, kyphoscoliosis, obesity hypoventilation syndrome |
Measurement & Grading
MRC (Medical Research Council) Dyspnea Scale
| Grade | Description |
|---|---|
| 0 | No dyspnea except with strenuous exercise |
| 1 | Dyspnea when hurrying on level ground or walking up a slight hill |
| 2 | Walks slower than people of same age on level ground due to breathlessness, or stops for breath while walking at own pace |
| 3 | Stops for breath after walking ~100 m or after a few minutes on level ground |
| 4 | Too breathless to leave the house, or breathless when dressing/undressing |
Modified Borg Scale
- 0 (nothing at all) to 10 (maximal) — used during exercise testing and inpatient assessment
NYHA Classification (for Cardiac Dyspnea)
| Class | Description |
|---|---|
| I | No symptoms with ordinary activity |
| II | Symptoms with moderate exertion |
| III | Symptoms with minimal exertion |
| IV | Symptoms at rest |
Clinical Evaluation
History — Key Questions
| Domain | Questions |
|---|---|
| Onset | Acute (minutes) vs. subacute (days) vs. chronic (weeks/months)? |
| Timing | Nocturnal (PND, cardiac asthma)? Positional (orthopnoea → HF; platypnoea → hepatopulmonary syndrome)? |
| Triggers | Exertion, allergens, cold air, lying flat? |
| Quality | Air hunger, chest tightness, effort, unsatisfying breath? |
| Associated symptoms | Cough, wheeze, sputum, haemoptysis, chest pain, palpitations, ankle swelling, fever? |
| Risk factors | Smoking (COPD), cardiac history, DVT/PE risk factors, occupational exposures (ILD), travel (PE) |
| Medications | Beta-blockers (bronchospasm), ACE inhibitors (cough misinterpreted as dyspnea), amiodarone (pulmonary toxicity) |
Positions and Dyspnea
| Positional Pattern | Mechanism | Condition |
|---|---|---|
| Orthopnoea | ↑ venous return when supine → ↑ pulmonary congestion | Heart failure, bilateral diaphragmatic paralysis |
| Paroxysmal nocturnal dyspnea (PND) | Reabsorption of peripheral oedema at night → pulmonary oedema | Heart failure |
| Platypnoea | Dyspnea when upright, relieved lying down | Hepatopulmonary syndrome, intracardiac shunts, orthodeoxia |
| Trepopnoea | Dyspnea in one lateral decubitus position | Unilateral lung or pleural disease |
Physical Examination
| Finding | Suggests |
|---|---|
| Wheeze | Asthma, COPD, cardiac asthma |
| Crackles (basal) | Pulmonary oedema, ILD, pneumonia |
| Absent breath sounds | Pneumothorax, large pleural effusion |
| Elevated JVP + S3 + oedema | Heart failure |
| Barrel chest + prolonged expiration | COPD |
| Clubbing | ILD, bronchiectasis, lung cancer |
| Cyanosis | Severe hypoxaemia |
| Stridor | Upper airway obstruction |
| Kussmaul breathing | Metabolic acidosis (DKA) |
Diagnostic Approach (Harrison's, p. 1112)
"As many as two-thirds of patients will require diagnostic testing beyond the initial clinical presentation."
Initial Investigations (First-line for all)
| Test | What it Evaluates |
|---|---|
| Pulse oximetry | Oxygen saturation; quick screen for hypoxaemia |
| CXR | Pulmonary oedema, pneumothorax, effusion, consolidation, cardiomegaly |
| ECG | Arrhythmia, ischaemia, RV strain (PE), LV hypertrophy |
| ABG | PaO₂, PaCO₂, pH, A-a gradient; hypoxaemia type |
| CBC | Anaemia |
| BMP/CMP | Metabolic acidosis, renal function |
| BNP / NT-proBNP | Heart failure (elevated in HF; normal effectively excludes HF as cause) |
Second-line Investigations
| Test | Indication |
|---|---|
| Echocardiography | Heart failure, valvular disease, pulmonary hypertension, pericardial effusion |
| Pulmonary function tests (PFTs) | Obstructive (COPD/asthma) vs. restrictive (ILD) pattern |
| CT pulmonary angiography (CTPA) | Pulmonary embolism (Wells score ≥2 or high clinical suspicion) |
| HRCT chest | ILD, bronchiectasis |
| D-dimer | Exclude PE in low-probability cases |
| Troponin | ACS as cause of acute dyspnea |
| Thyroid function tests | Hyperthyroidism (↑ ventilatory drive) |
| Cardiopulmonary exercise testing (CPET) | Integrative assessment when cause remains unclear; differentiates cardiac vs. pulmonary vs. deconditioning vs. psychogenic |
Algorithmic Approach
Dyspnea
↓
Acute or Chronic?
↓ ↓
ACUTE CHRONIC
History + Exam History + Exam
Pulse oximetry, CXR, ECG CXR, ECG, CBC, BNP, PFTs
BNP, ABG, troponin Echocardiogram if cardiac
↓ ↓
Life-threatening first: Still unclear?
Pneumothorax → chest drain ↓
Pulmonary oedema → diuretics CPET / HRCT / CTPA /
Severe asthma → bronchodilators Subspecialty referral
PE → anticoagulation
Tamponade → pericardiocentesis
Management
Disease-Specific Treatment
| Condition | Treatment |
|---|---|
| Heart failure | Diuretics, ACE inhibitors/ARBs, beta-blockers, SGLT2 inhibitors |
| COPD | Bronchodilators (LABA, LAMA), ICS, pulmonary rehabilitation, oxygen |
| Asthma | ICS, SABA for rescue, LABA, biologics (severe) |
| Pulmonary embolism | Anticoagulation (LMWH/DOAC); thrombolysis if massive PE |
| Pneumothorax | Observation (small) or chest drain (large/tension) |
| Anaemia | Iron, B₁₂, folate supplementation; transfusion if severe |
| Pulmonary fibrosis | Antifibrotics (nintedanib, pirfenidone) |
| Pulmonary hypertension | Prostacyclins, endothelin antagonists, PDE5 inhibitors |
Symptomatic / Palliative Management of Dyspnea
| Intervention | Evidence |
|---|---|
| Low-dose opioids (morphine) | Most evidence-based pharmacological treatment for refractory dyspnea; reduces air hunger and ventilatory drive without significant respiratory depression at low doses |
| Supplemental oxygen | Beneficial if hypoxaemic (SpO₂ <88%); no benefit in normoxaemic patients with COPD or cancer dyspnea |
| Fan / cool air directed to face | Stimulates facial receptors (V2 branch of trigeminal nerve) → reduces dyspnea perception |
| Pulmonary rehabilitation | Improves dyspnea, exercise tolerance, quality of life in COPD/ILD |
| Anxiolytics (benzodiazepines) | Adjunctive in anxiety-related dyspnea; limited evidence as sole therapy |
| Heliox (helium-oxygen) | Reduces airway resistance; used in upper airway obstruction and severe asthma |
| Non-invasive ventilation (NIV/CPAP/BiPAP) | Acute hypercapnic COPD exacerbation, acute cardiogenic pulmonary oedema |
Special Situations
Dyspnea in the Absence of Hypoxaemia
- Common in anaemia, deconditioning, pulmonary hypertension (may maintain saturation until late)
- Normal SpO₂ does not exclude significant dyspnea or serious pathology
Dyspnea with Normal PFTs and Normal Imaging
- Cardiac cause (exercise echocardiography or CPET)
- Pulmonary hypertension (right heart catheterisation)
- Deconditioning
- Psychogenic / functional dyspnea
- Neuromuscular disease (maximal inspiratory/expiratory pressure measurements)
Dyspnea at End of Life
- Opioids remain the cornerstone of palliation
- Oxygen helpful only if hypoxaemic
- Fan therapy, cool room, upright positioning
- Avoid futile investigations — focus on comfort
Key Teaching Points (Harrison's, Ch. 37)
- Dyspnea is multidimensional — its quality (air hunger vs. tightness vs. effort) guides diagnosis
- The efferent–afferent mismatch model best explains dyspnea across conditions
- BNP is the single most useful initial biomarker to differentiate cardiac from pulmonary dyspnea
- CPET is the gold standard when aetiology remains unclear after standard workup
- Orthopnoea and PND are highly specific for heart failure
- In normoxaemic patients, supplemental oxygen does not relieve dyspnea — cool facial airflow (fan) is more effective
- Low-dose opioids are the most evidence-based pharmacological treatment for refractory/palliative dyspnea
- For patients with known cardiopulmonary disease, always ask: has the known disease progressed, or is there a new process? (Harrison's, p. 1112)
Harrisons chapter 13 to 66 cardinal features summarised briefly
Harrison's sections cardinal manifestations chapters 13 14 15 16 17 18 19 20 pain fever headache chest
Harrison's cardinal manifestations table of contents chapters 21 to 40 dyspnea cough edema palpitations syncope
Harrison's table of contents section 2 cardinal manifestations symptoms chapter list
Harrison's chapters pain chest headache abdominal back limb fever chills weight loss fatigue anorexia
Harrison's Chapters 13–66: Cardinal Manifestations — Brief Summaries
Harrison's Principles of Internal Medicine, 21st Edition
Part 2: Cardinal Manifestations and Presentation of Diseases
SECTION 1 — PAIN
Ch. 13 — Pain: Pathophysiology and Management
- Pain = unpleasant sensory/emotional experience from actual or potential tissue damage
- Types: Nociceptive (somatic/visceral), neuropathic, nociplastic
- Transduction → Transmission → Modulation → Perception (4-step pathway)
- Key receptors: Aδ (sharp, fast) and C fibres (burning, slow); first synapse in dorsal horn
- Sensitisation: Peripheral (↑ prostaglandins, bradykinin) and central (wind-up, allodynia)
- Descending modulation: Endogenous opioids, serotonin, noradrenaline pathways
- WHO analgesic ladder: Paracetamol/NSAIDs → weak opioids → strong opioids; adjuvants at each step
- Neuropathic pain: TCAs, SNRIs, gabapentinoids, topical lidocaine
Ch. 14 — Chest Discomfort
- Most critical diagnosis to exclude: ACS (STEMI/NSTEMI/UA)
- Causes classified by structure:
| Origin | Examples |
|---|---|
| Cardiac ischaemic | ACS, stable angina, vasospasm |
| Cardiac non-ischaemic | Pericarditis, myocarditis, aortic dissection |
| Pulmonary | PE, pneumothorax, plpneumonia, pleuritis |
| GI | GERD, oesophageal spasm, peptic ulcer |
| Musculoskeletal | Costochondritis, rib fracture, Tietze syndrome |
| Psychogenic | Panic disorder, anxiety |
- Ischaemic pain: pressure/squeezing, radiation to jaw/left arm, associated diaphoresis
- Key tools: ECG, troponin, CXR; HEART score for risk stratification
Ch. 15 — Abdominal Pain
- Visceral pain: poorly localised, midline, cramping (hollow organs) or aching (solid organs)
- Parietal pain: well-localised, sharp, worsened by movement → peritoneal irritation
- Referred pain: diaphragmatic irritation → shoulder tip; ureteric colic → groin
- Causes by quadrant:
- RUQ: cholecystitis, hepatitis, Fitz-Hugh-Curtis
- LUQ: splenomegaly, gastritis, pancreatitis (tail)
- RLQ: appendicitis, Meckel's, ovarian pathology, Crohn's
- LLQ: diverticulitis, sigmoid volvulus, ovarian cyst
- Diffuse: peritonitis, mesenteric ischaemia, IBD, IBS
- Surgical emergencies: Perforated viscus, acute mesenteric ischaemia, ruptured ectopic, aortic aneurysm
Ch. 16 — Headache
- Most common: Tension-type (bilateral, band-like, no nausea)
- Migraine: Unilateral, pulsating, nausea/vomiting, photo/phonophobia; with or without aura; Tx: triptans, CGRP antagonists
- Cluster: Periorbital, autonomic features (lacrimation, ptosis, rhinorrhoea), circadian; Tx: O₂, sumatriptan
- Secondary causes (red flags — SNOOP4):
- Systemic illness, Neurological deficit, Onset sudden/thunderclap, Older age, Positional, Progressive, Papilledema, Prior headache change
- Thunderclap: SAH until proven otherwise → CT head → LP if CT negative
- Raised ICP: Progressive, worse in morning, with Valsalva, papilledema
Ch. 17 — Back and Neck Pain
- Most common: Non-specific mechanical low back pain (95%)
- Red flags for serious cause (TUMOUR/FRACTURE):
- Age >50, history of cancer, unexplained weight loss, night pain, fever, bowel/bladder dysfunction, saddle anaesthesia
- Lumbar disc herniation: L4-L5 (foot drop), L5-S1 (↓ ankle reflex, calf weakness)
- Spinal stenosis: Neurogenic claudication — bilateral leg pain with walking, relieved by flexion
- Cauda equina syndrome: Surgical emergency — saddle anaesthesia + urinary retention
- Cervical myelopathy: Upper motor neuron signs in legs + lower motor neuron signs at level of lesion
- Investigations: MRI spine (first-line for neurological deficit or red flags)
Ch. 18 — Numbness, Tingling, and Sensory Loss
- Sensory modalities: Pain/temperature (spinothalamic — contralateral) vs. vibration/proprioception (dorsal columns — ipsilateral)
- Peripheral neuropathy: Glove-and-stocking distribution; diabetes, alcohol, B₁₂ deficiency, Guillain-Barré
- Mononeuropathy: Single nerve compression (carpal tunnel, ulnar, common peroneal)
- Spinal cord lesions: Brown-Séquard (hemisection), complete transection, central cord syndrome
- Thalamic lesions: Contralateral hemibody sensory loss
- Cortical lesions: Contralateral limb; discriminative sensation most affected
Ch. 19 — Weakness and Paralysis
- Distinguish UMN vs LMN vs. NMJ vs. Muscle:
| Feature | UMN | LMN |
|---|---|---|
| Tone | ↑ (spastic) | ↓ (flaccid) |
| Reflexes | ↑, Babinski + | ↓, absent |
| Wasting | Minimal | Prominent |
| Distribution | Pyramidal (arm extensors, leg flexors) | Segmental/focal |
- NMJ: Fatigable weakness (myasthenia gravis — ocular, bulbar); Lambert-Eaton (proximal, ↑ with repetition)
- Myopathy: Proximal symmetric weakness, normal sensation, ↑CK
- Causes of acute paralysis: Stroke, GBS, spinal cord compression, hypokalemia, botulism
Ch. 20 — Faintness, Syncope, Dizziness, and Vertigo
- Syncope: Transient loss of consciousness from global cerebral hypoperfusion; self-limited
- Reflex (vasovagal — most common), orthostatic, cardiac (arrhythmia, structural)
- Dangerous: VT, complete heart block, HOCM, aortic stenosis, PE
- Tilt-table test, ECG, Holter monitor, echocardiogram
- Presyncope: Same causes; incomplete episode
- Dizziness: Vertigo (illusion of motion), disequilibrium, lightheadedness
- Vertigo:
- Peripheral: BPPV (most common — Dix-Hallpike +ve, brief, fatigable), Ménière's disease (tinnitus + hearing loss + episodic vertigo), vestibular neuritis (prolonged, viral)
- Central: Brainstem/cerebellar; no latency, non-fatigable; HINTS exam
- BPPV treatment: Epley manoeuvre
Ch. 21 — Syncope
- Reflex syncope: Vasovagal, situational (cough, micturition), carotid sinus hypersensitivity
- Orthostatic hypotension: ≥20 mmHg systolic drop on standing; autonomic neuropathy, hypovolaemia, drugs
- Cardiac syncope: Most dangerous — arrhythmia (prolonged QT, Brugada, WPW), structural (AS, HCM, PE)
- ROSE/SFSR/San Francisco Syncope Rules: Identify high-risk patients requiring admission
- Investigations: ECG (all), echocardiogram, Holter/implantable loop recorder, tilt table
SECTION 2 — ALTERATIONS IN BODY TEMPERATURE
Ch. 22 — Fever
- Fever = Tcore >38°C (100.4°F); hyperpyrexia >41.5°C
- Pyrogens: Exogenous (LPS) → macrophages → endogenous pyrogens (IL-1, IL-6, TNF) → hypothalamus → PGE₂ → ↑ set-point
- Fever vs. hyperthermia: Fever = raised set-point (responds to antipyretics); Hyperthermia = failure of thermoregulation (does NOT respond — heat stroke, malignant hyperthermia, NMS)
- Causes: Infection (most common), malignancy, autoimmune/inflammatory, drugs, endocrine (thyroid storm, phaeochromocytoma)
- FUO (Fever of Unknown Origin): >38.3°C on ≥3 occasions over ≥3 weeks with no diagnosis after 1 week of investigation
- Classic FUO causes: Infection (TB, endocarditis, abscess), malignancy (lymphoma), connective tissue disease (SLE, Still's)
- Antipyretics: Paracetamol, NSAIDs (COX-inhibitors → ↓ PGE₂)
Ch. 23 — Fever and Rash
- Combination of fever + rash narrows differential significantly:
| Rash Type | Key Diagnoses |
|---|---|
| Maculopapular | Viral exanthems, drug reaction, secondary syphilis, typhoid, SLE |
| Petechiae/Purpura | Meningococcaemia, DIC, Rocky Mountain spotted fever, vasculitis, ITP |
| Vesicular | Varicella, herpes zoster, HSV disseminated, enterovirus |
| Urticarial | Drug reaction, serum sickness, viral hepatitis |
| Nodular | Disseminated fungal (histoplasma, coccidioides), Janeway lesions (IE) |
| Desquamating | Toxic shock syndrome (TSS), SSSS, scarlet fever, Kawasaki |
- Meningococcaemia: Non-blanching petechiae/purpura → emergency — immediate IV benzylpenicillin
- RMSF: Centripetal spread of petechiae (wrist/ankles → trunk); Rickettsia rickettsii; Tx: doxycycline
Ch. 24 — Hypothermia and Frostbite
- Hypothermia: Core temp <35°C
- Mild (32–35°C): Shivering, confusion
- Moderate (28–32°C): ↓ shivering, arrhythmias (J/Osborn waves on ECG), hypotension
- Severe (<28°C): VF risk, no shivering, coma
- Rewarming: Passive (mild) → active external (moderate) → active internal (severe: warmed IV fluids, bladder/peritoneal lavage, ECMO in refractory VF)
- "Not dead until warm and dead"
- Frostbite: Ice crystal formation in tissues; superficial vs. deep; Tx: rapid rewarming in 40°C water, ibuprofen, TPA for severe cases
SECTION 3 — NERVOUS SYSTEM DYSFUNCTION
Ch. 25 — Confusion and Delirium
- Delirium: Acute disturbance of attention + cognition with fluctuating course; reversible
- Hyperactive (agitation, hallucinations) vs. Hypoactive (withdrawn, quiet — often missed) vs. Mixed
- Causes — AEIOU TIPS: Alcohol/drugs, Epilepsy, Infection, Overdose, Uraemia, Trauma, Insulin (hypo/hyperglycaemia), Psychiatric, Stroke/structural
- Predisposing (baseline vulnerability): Age, dementia, sensory impairment, dehydration
- Precipitating: Infection, surgery, medications (anticholinergics, opioids, benzodiazepines), sleep deprivation
- CAM (Confusion Assessment Method): Acute onset + inattention + (disorganised thinking OR altered consciousness)
- Management: Treat cause; non-pharmacological first (reorientation, day/night cues, avoid restraints); haloperidol if agitated and dangerous
Ch. 26 — Dementia
- Progressive cognitive decline affecting ≥2 domains; interferes with daily function
- Alzheimer's disease (most common, 60–70%): β-amyloid plaques, neurofibrillary tangles; episodic memory first; MMSE/MoCA; Tx: cholinesterase inhibitors (donepezil), memantine
- Vascular dementia: Stepwise decline; risk factors = stroke risk factors; neuroimaging shows infarcts
- Lewy body dementia: Fluctuating cognition, visual hallucinations, parkinsonism, REM sleep behaviour disorder; hypersensitive to antipsychotics
- Frontotemporal dementia (FTD): Behavioural changes or language dysfunction; younger onset; tau/TDP-43 pathology
- Reversible causes (must exclude): B₁₂ deficiency, hypothyroidism, neurosyphilis, normal pressure hydrocephalus (NPH — triad: dementia, gait apraxia, urinary incontinence), subdural haematoma, depression (pseudodementia)
Ch. 27 — Aphasia, Memory Loss, and Other Focal Cerebral Disorders
- Aphasia:
- Broca's (expressive): Non-fluent, good comprehension, poor repetition; frontal lobe
- Wernicke's (receptive): Fluent but paraphasic, poor comprehension; temporal lobe
- Global: Both expression and comprehension impaired; large MCA territory infarct
- Conduction: Good fluency + comprehension, poor repetition; arcuate fasciculus
- Memory: Declarative (hippocampus) vs. procedural (basal ganglia/cerebellum)
- Amnesia: Anterograde (can't form new memories) vs. retrograde (can't recall past)
- Neglect: Non-dominant parietal lobe; inattention to contralateral space
- Apraxia: Inability to perform learned motor acts despite intact motor/sensory function
- Agnosia: Inability to recognise objects despite intact sensory function
Ch. 28 — Sleep Disorders
- Sleep stages: NREM (N1→N2→N3/slow wave) + REM; ~90 min cycles
- Insomnia: Most common; acute (stress) or chronic (>3 months); CBT-I first-line over pharmacotherapy
- Obstructive sleep apnoea (OSA): Repetitive upper airway collapse; snoring, apnoeas, EDS; AHI ≥5; CPAP is gold standard; associated with HTN, AF, metabolic syndrome
- Narcolepsy: Excessive daytime sleepiness + cataplexy (type 1); hypocretin/orexin deficiency; Tx: modafinil (EDS), sodium oxybate (cataplexy)
- Restless legs syndrome (RLS): Urge to move legs at rest, worse at night, relieved by movement; dopaminergic deficiency; Fe deficiency; Tx: dopamine agonists (pramipexole), gabapentin
- Circadian rhythm disorders: Jet lag, shift work, delayed sleep phase syndrome
- Parasomnias: Sleepwalking, REM sleep behaviour disorder (RBD — acts out dreams; early marker of Parkinson's/Lewy body dementia)
SECTION 4 — DISORDERS OF EYES, EARS, NOSE, AND THROAT
Ch. 29 — Disorders of the Eye
- Visual loss:
- Sudden painless monocular: CRAO (cherry red spot), CRVO, anterior ischaemic optic neuropathy (AION), vitreous haemorrhage, retinal detachment
- Sudden painful: Acute angle-closure glaucoma (fixed mid-dilated pupil, hard eye, corneal oedema)
- Transient monocular (amaurosis fugax): TIA/carotid disease — treat as stroke
- Bilateral: Cortical blindness (occipital stroke), raised ICP, toxic (methanol)
- Afferent pupillary defect (RAPD/Marcus Gunn): Optic nerve or severe retinal disease
- Papilledema: Bilateral disc swelling from raised ICP; visual obscurations; must urgently investigate
- Diplopia: Monocular (refractive) vs. binocular (CN III, IV, VI palsy or NMJ)
- CN III palsy: "Down and out" + ptosis ± dilated pupil (surgical CN III — posterior communicating artery aneurysm)
- Glaucoma: Optic nerve damage from raised IOP; open angle (chronic, asymptomatic) vs. closed angle (acute, emergency); Tx: topical beta-blockers, prostaglandin analogues
Ch. 30 — Disorders of Smell, Taste, and Hearing
- Anosmia: Post-viral (COVID-19), head trauma (cribriform plate), nasal polyps, neurodegenerative (Parkinson's — early sign), tumour (olfactory groove meningioma)
- Dysgeusia/Ageusia: Zinc deficiency, B₁₂ deficiency, post-viral, medication side effect
- Hearing loss:
- Conductive: Outer/middle ear; Rinne (BC>AC), Weber lateralises to affected side; causes: wax, otitis media, otosclerosis
- Sensorineural: Cochlea/VIII nerve; Rinne (AC>BC), Weber lateralises to better ear; causes: presbycusis (ageing), noise-induced, Ménière's, acoustic neuroma, ototoxic drugs (aminoglycosides, cisplatin, loop diuretics)
- Tinnitus: Subjective vs. objective (vascular — AVM, glomus tumour); pulsatile tinnitus in IIH
- Vertigo: See Ch. 20
SECTION 5 — CARDIOVASCULAR SYMPTOMS
Ch. 31 — Palpitations
- Awareness of heartbeat; may represent benign or life-threatening arrhythmia
- Characterise: Regular vs. irregular; onset/offset (sudden = re-entry); triggers; associated presyncope/syncope
- Causes: Ectopics (most common — PACs/PVCs), SVT, AF/flutter, VT, anxiety, hyperthyroidism, anaemia, caffeine, drugs
- Key investigations: 12-lead ECG (during symptoms if possible), Holter monitor (24–48h), event recorder, implantable loop recorder (for infrequent symptoms); TFTs, FBC, electrolytes
- Red flags: Palpitations + syncope + family history of sudden death = urgent cardiology referral
Ch. 32 — Hypertension
- Definition: ≥130/80 mmHg (ACC/AHA 2017) or ≥140/90 (ESC/WHO)
- Primary (essential): 90–95%; no identifiable cause; multifactorial (genetics, RAAS, SNS, salt)
- Secondary causes (5–10%): Renal artery stenosis, primary hyperaldosteronism (Conn's), phaeochromocytoma, Cushing's, coarctation of aorta, OSA, CKD
- Hypertensive urgency: Severe HTN without end-organ damage → oral agents
- Hypertensive emergency: Severe HTN + end-organ damage (hypertensive encephalopathy, aortic dissection, eclampsia, acute MI, acute HF) → IV agents (labetalol, nicardipine, nitroprusside)
- Treatment: Lifestyle → thiazides, ACE inhibitors/ARBs, CCBs, beta-blockers (compelling indications)
- JNC/ESC stages: Stage 1 (130–139/80–89) → Stage 2 (≥140/≥90)
Ch. 33 — Cardiac Arrest and Sudden Cardiac Death
- SCD: Unexpected cardiac death within 1h of symptom onset; most common cause = VF from CAD
- Causes: Structural (CAD, HCM, ARVC, dilated CM) vs. Primary electrical (long QT, Brugada, WPW, CPVT)
- BLS → ACLS: Chest compressions (100-120/min, 5-6cm depth) → defibrillation (shockable: VF/pVT) → adrenaline (1mg IV q3-5min) → amiodarone
- Post-ROSC: Targeted temperature management (32-36°C for 24h), PCI if STEMI/suspected cardiac cause, neuroprognostication at 72h
- Prevention: ICD in high-risk patients (EF ≤35%, sustained VT, survivors of SCD)
Ch. 34 — Shock
- Definition: Inadequate tissue perfusion and oxygen delivery; MAP <65 mmHg with end-organ dysfunction
- 4 types:
| Type | Mechanism | Examples | Haemodynamics |
|---|---|---|---|
| Distributive | Vasodilation | Septic (most common), anaphylactic, neurogenic | ↑CO, ↓SVR |
| Cardiogenic | Pump failure | MI, acute HF, myocarditis, tamponade | ↓CO, ↑SVR |
| Hypovolaemic | ↓ Preload | Haemorrhage, dehydration, burns | ↓CO, ↑SVR |
| Obstructive | Mechanical obstruction | Massive PE, tension pneumothorax, cardiac tamponade | ↓CO, ↑SVR |
- Septic shock: Sepsis + vasopressors + lactate >2 despite fluid resuscitation; Tx: 30 mL/kg crystalloid, noradrenaline (first-line vasopressor), hydrocortisone if refractory, antibiotics within 1h
- Distributive: Beck's triad (tamponade) → pericardiocentesis
Ch. 35 — Dyspnea (see Ch. 37)
Ch. 36 — Cough and Haemoptysis
- Cough: Most common cause of chronic cough = upper airway cough syndrome (UACS/PND), asthma, GERD (the triad)
- ACE inhibitor-induced cough (bradykinin → switch to ARB)
- Acute: Viral URTI; Subacute (3–8 weeks): Post-infectious, pertussis; Chronic (>8 weeks): UACS, asthma, GERD, ILD, bronchiectasis, malignancy, TB
- Red flags: Haemoptysis, weight loss, smoker >40 yrs, new cough → CXR/CT
- Haemoptysis:
- Causes: Bronchitis (most common), bronchogenic carcinoma, TB, bronchiectasis, PE, AVM, mitral stenosis, coagulopathy
- Massive haemoptysis (>200–600 mL/24h): Life-threatening → airway protection, bronchoscopy, bronchial artery embolisation
Ch. 37 — Dyspnea (Full summary covered above)
Ch. 38 — Hypoxia and Cyanosis
- Hypoxia: Inadequate O₂ delivery to tissues
- Hypoxaemic (↓PaO₂): Low FiO₂, hypoventilation, V/Q mismatch, shunt, diffusion impairment
- Anaemic: Normal PaO₂, ↓Hb carrying capacity
- Stagnant/circulatory: Normal PaO₂ + Hb, ↓CO (heart failure, shock)
- Histotoxic: Normal delivery, impaired utilisation (cyanide poisoning)
- A-a gradient: Normal <15 mmHg; elevated in V/Q mismatch, shunt, diffusion; normal in hypoventilation/altitude
- Cyanosis:
- Central: Low SaO₂; tongue + mucous membranes involved; causes = severe lung disease, R→L shunt, methaemoglobinaemia
- Peripheral: Normal SaO₂, ↑O₂ extraction; cold, ↓CO, Raynaud's; spares mucous membranes
- Methaemoglobinaemia: Chocolate-brown blood; saturation gap; Tx: methylene blue
Ch. 39 — Oedema
- Oedema = excess interstitial fluid; clinically apparent when >3L accumulated
- Starling forces: ↑ capillary hydrostatic pressure OR ↓ oncotic pressure → oedema
- Generalised (anasarca):
- Cardiac: Dependent, pitting; JVP ↑, S3, orthopnoea
- Renal (nephrotic): Periorbital (morning), pitting; heavy proteinuria >3.5g/day; ↓albumin
- Hepatic (cirrhosis): Ascites prominent; ↓albumin, ↑portal pressure; spider naevi, palmar erythema
- Nutritional/Kwashiorkor: ↓albumin from malnutrition
- Myxoedema: Non-pitting, hypothyroidism; periorbital; no protein loss
- Localised oedema: DVT, cellulitis, lymphoedema (non-pitting), venous insufficiency
- Idiopathic oedema: Young women; exacerbated by upright posture
Ch. 40 — Atlas of ECG
- Systematic ECG reading: Rate → Rhythm → Axis → P wave → PR interval → QRS → ST segment → T wave → QTc
- Key abnormalities:
- STEMI: ST elevation in anatomical territories; reciprocal changes
- LBBB: Broad notched R in V5/V6, deep S in V1; blocks STEMI diagnosis (Sgarbossa criteria)
- LVH: Sokolow-Lyon (S in V1 + R in V5/V6 >35mm)
- Long QT: QTc >440ms (men), >460ms (women); risk of TdP
- Brugada: Coved ST elevation in V1-V2; risk of VF
- WPW: Short PR, delta wave, broad QRS
SECTION 6 — ALTERATIONS IN GASTROINTESTINAL FUNCTION
Ch. 41 — Nausea, Vomiting, and Indigestion
- Nausea/Vomiting: Mediated via vomiting centre (medullary) + chemoreceptor trigger zone (CTZ, area postrema — outside BBB)
- Causes: GI (gastroenteritis, obstruction, gastroparesis), CNS (raised ICP, migraine, motion sickness), metabolic (DKA, uraemia, Addison's), drugs (opioids, chemotherapy), pregnancy (hCG)
- Projectile vomiting: Pyloric stenosis (infant), raised ICP
- Antiemetics: Ondansetron (5-HT₃), metoclopramide (D₂), domperidone (D₂ — peripheral), prochlorperazine, dexamethasone (chemo), cyclizine (motion sickness, pregnancy)
- Indigestion/dyspepsia: Upper abdominal discomfort; functional vs. organic; investigate if alarm features (weight loss, dysphagia, haematemesis, age >55)
Ch. 42 — Dysphagia
- Oropharyngeal (transfer): Difficulty initiating swallow; neuromuscular causes (stroke, MG, motor neuron disease, Parkinson's); nasal regurgitation, aspiration
- Oesophageal: Food "sticks" after swallowing; structural (stricture, carcinoma, ring/web) or motility (achalasia, diffuse oesophageal spasm)
- Achalasia: ↓ lower oesophageal sphincter relaxation + absent peristalsis; "bird's beak" on barium; manometry gold standard; Tx: pneumatic dilatation, Heller myotomy, POEM, botulinum toxin
- Oesophageal carcinoma: Dysphagia to solids then liquids; progressive weight loss; SCC (upper/mid) vs. adenocarcinoma (lower/GOJ — Barrett's oesophagus)
- Plummer-Vinson syndrome: Post-cricoid web + iron deficiency anaemia + dysphagia; risk of pharyngeal carcinoma
Ch. 43 — Diarrhoea and Constipation
- Acute diarrhoea (<4 weeks): Usually infectious; secretory (watery, persists with fasting), inflammatory (bloody, fever, PMNs)
- Non-inflammatory: Vibrio cholerae, ETEC, viruses
- Inflammatory: Salmonella, Shigella, Campylobacter, C. difficile, EHEC (O157:H7 — HUS risk)
- Chronic diarrhoea (>4 weeks):
- Osmotic: Stops with fasting (lactose intolerance, Mg²⁺, sorbitol)
- Secretory: Persists with fasting (VIPoma, carcinoid, bile acid malabsorption, microscopic colitis)
- Inflammatory: IBD (Crohn's, UC), coeliac
- Malabsorptive: Steatorrhoea; coeliac, chronic pancreatitis, small bowel bacterial overgrowth
- Motility: IBS, hyperthyroidism, diabetic enteropathy
- Constipation: <3 stools/week; primary (functional, slow transit, dyssynergia) vs. secondary (hypothyroidism, hypercalcaemia, drugs — opioids, antacids, CCBs)
Ch. 44 — Weight Loss
- Involuntary weight loss >5% in 6–12 months = clinically significant; always warrants investigation
- Causes:
- Inadequate intake: Depression, dementia, dysphagia, anorexia (cancer, drugs, social)
- ↑ Caloric need: Hyperthyroidism, malignancy, infection (TB, HIV), COPD, heart failure
- Malabsorption: Coeliac, IBD, pancreatic insufficiency, short bowel
- Malignancy is found in ~25% of patients with unexplained weight loss after full workup
- Investigations: CBC, CMP, TFTs, glucose, CXR, FOBT, PSA (men), mammography; CT chest/abdomen if high suspicion
- Cachexia: Weight loss + muscle wasting in context of chronic illness (cancer, HF, CKD, COPD); mediated by TNF, IL-1, IL-6
Ch. 45 — Gastrointestinal Bleeding
- Upper GI bleeding (UGIB): Source proximal to Treitz ligament; haematemesis (bright red or coffee grounds) + melaena
- Causes: Peptic ulcer (most common), oesophageal varices, Mallory-Weiss tear, erosive gastritis, Dieulafoy lesion, angiodysplasia, malignancy
- Rockford/Blatchford Score: Risk stratify pre-endoscopy
- Endoscopy within 24h (12h if high-risk variceal)
- Varices: Terlipressin, octreotide, prophylactic antibiotics (norfloxacin/ceftriaxone), endoscopic banding
- PUD: PPI infusion (80mg bolus + 8mg/h); endoscopic haemostasis
- Lower GI bleeding (LGIB): Source distal to Treitz; haematochezia
- Causes: Diverticulosis (most common), angiodysplasia, colitis (IBD, ischaemic, infectious), colorectal cancer, haemorrhoids, polyps
- Colonoscopy after bowel prep; CT angiography if haemodynamically unstable
Ch. 46 — Jaundice
- Bilirubin metabolism: Haem → unconjugated bilirubin → liver conjugation → conjugated → bile → urobilinogen
- Classification:
- Pre-hepatic (unconjugated): Haemolysis, Gilbert's, Crigler-Najjar; urine normal, ↑LDH, ↓haptoglobin
- Hepatic (mixed): Hepatitis (viral, alcoholic, autoimmune, drugs), cirrhosis; ↑ALT/AST
- Post-hepatic/cholestatic (conjugated): Bile duct obstruction (stones, stricture, carcinoma, PSC, PBC); dark urine, pale stools, pruritus; ↑ALP, ↑GGT
- Gilbert's syndrome: Benign; ↑unconjugated bilirubin with fasting/stress; glucuronosyltransferase mutation; no treatment needed
- Investigations: LFTs, bilirubin fractions, hepatitis serology, ANA/ASMA/AMA, ultrasound (first-line imaging), MRCP, ERCP
Ch. 47 — Abdominal Swelling and Ascites
- Ascites:
- SAAG ≥1.1 g/dL (portal hypertension): Cirrhosis (75%), cardiac ascites, Budd-Chiari
- SAAG <1.1 g/dL (non-portal hypertension): Malignancy (peritoneal carcinomatosis), TB peritonitis, nephrotic syndrome, pancreatitis
- Spontaneous bacterial peritonitis (SBP): PMN >250/mm³ in ascitic fluid; E. coli, Klebsiella; Tx: cefotaxime; prophylaxis: norfloxacin
- Hepatic hydrothorax: Transdiaphragmatic passage of ascitic fluid; right-sided pleural effusion in cirrhosis
- Hepatorenal syndrome: Functional renal failure in decompensated cirrhosis; ↑creatinine, ↓Na; Tx: terlipressin + albumin, TIPS, liver transplantation
SECTION 7 — ALTERATIONS IN RENAL AND URINARY TRACT FUNCTION
Ch. 48 — Azotaemia and Urinary Abnormalities
- Azotaemia: ↑BUN and creatinine
- Pre-renal: ↓GFR from ↓renal perfusion; BUN:Cr >20:1; FENa <1%; responds to fluids
- Intrinsic renal: ATN (ischaemia/nephrotoxins — most common), GN, AIN, vascular; FENa >2%
- Post-renal: Obstruction; bilateral or single kidney; hydronephrosis on US
- Proteinuria: Glomerular vs. tubular; >3.5g/day = nephrotic range
- Haematuria: Microscopic vs. macroscopic; glomerular (dysmorphic RBCs, casts) vs. urological (transitional cell carcinoma, stones, infection)
- Urinary casts:
- RBC casts → glomerulonephritis
- WBC casts → pyelonephritis/interstitial nephritis
- Granular/muddy brown casts → ATN
- Waxy/broad casts → chronic renal failure
- Hyaline casts → normal/concentrated urine
Ch. 49 — Fluid and Electrolyte Disturbances
- Hyponatraemia (<135): Assess osmolality + volume status; SIADH (euvolaemic, ↓uOsm, ↑urine Na); Tx: fluid restriction (SIADH), hypertonic saline (severe/symptomatic); correct slowly (<10 mEq/24h) to avoid osmotic demyelination syndrome (ODS)
- Hypernatraemia (>145): Almost always = free water deficit; diabetes insipidus (central vs. nephrogenic); Tx: free water replacement
- Hypokalaemia (<3.5): Muscle weakness, cramps, U waves on ECG, ileus; causes: diarrhoea, vomiting, diuretics, Conn's, alkalosis, refeeding; Tx: KCl replacement
- Hyperkalaemia (>5.5): Peaked T waves → PR prolongation → sine wave → VF; causes: AKI, Addison's, ACE inhibitors, K-sparing diuretics; Tx: calcium gluconate (membrane stabilise), insulin + glucose, sodium bicarbonate, salbutamol, kayexalate/patiromer, dialysis
- Acid-base: Metabolic acidosis (↑AG: MUDPILES; normal AG: hyperchloraemic) vs. alkalosis; respiratory acidosis/alkalosis; Winter's formula for compensation
Ch. 50 — Acidosis and Alkalosis
- Stepwise approach: pH → primary disorder → compensation → AG → delta-delta
- Metabolic acidosis with elevated AG (MUDPILES): Methanol, Uraemia, DKA, Propylene glycol, Isoniazid/Iron, Lactic acidosis, Ethylene glycol, Salicylates
- Normal AG metabolic acidosis: Diarrhoea (GI bicarbonate loss), renal tubular acidosis (RTA), saline infusion
- Metabolic alkalosis: Vomiting, nasogastric suction, diuretics, Conn's, Bartter/Gitelman syndromes; paradoxical aciduria in severe hypovolaemia
- Lactic acidosis: Type A (tissue hypoperfusion — sepsis, shock) vs. Type B (no hypoperfusion — metformin, liver failure, malignancy)
- Respiratory acidosis: Hypoventilation; COPD, obesity hypoventilation, sedation → ↑PCO₂
- Respiratory alkalosis: Hyperventilation; anxiety, PE, salicylates, altitude, liver failure
SECTION 8 — ALTERATIONS IN THE SKIN
Ch. 51 — Approach to the Patient with Skin Disease (Ch. 56 in Harrison's)
Ch. 52–57 — Specific Skin Disorders (Covered in earlier summaries)
SECTION 9 — HAEMATOLOGICAL ABNORMALITIES
Ch. 58 — Anaemia and Polycythaemia (Ch. 63 in some editions)
- Anaemia: Hb <13 g/dL (men), <12 g/dL (women)
- Classification:
| MCV | Type | Causes |
|---|---|---|
| Microcytic (<80) | Iron deficiency, thalassaemia, ACD, sideroblastic | Ferritin ↓ (IDA), normal/↑ (ACD) |
| Normocytic (80–100) | ACD, haemolysis, aplastic, early deficiencies, CKD | Reticulocyte count key |
| Macrocytic (>100) | B₁₂/folate deficiency (megaloblastic), liver disease, hypothyroidism, MDS | Hypersegmented neutrophils in megaloblastic |
- Haemolytic anaemia: ↑reticulocytes, ↑LDH, ↑unconjugated bilirubin, ↓haptoglobin; Coombs test (AIHA)
- Polycythaemia vera: JAK2 V617F mutation; ↑RBC, WBC, platelets; splenomegaly; risk of thrombosis and myelofibrosis; Tx: phlebotomy, hydroxyurea
Ch. 59 — Bleeding and Thrombosis (Ch. 64)
- Primary haemostasis (platelet plug): vWF → GPIb → platelet adhesion; ADP, TXA₂ → platelet aggregation via GPIIb/IIIa
- Secondary haemostasis (coagulation cascade): Intrinsic (PT → XII, XI, IX, VIII) → Extrinsic (aPTT → VII, TF) → Common (X, V, II, I)
- Bleeding disorders:
- Platelet/vascular: Petechiae, purpura, mucosal bleeding; PT/aPTT normal
- Coagulation factor: Deep haematomas, haemarthroses; prolonged PT/aPTT
- DIC: Simultaneous bleeding + clotting; ↓platelets, ↑PT/aPTT, ↑D-dimer, ↓fibrinogen; treat underlying cause
- Thrombophilia: DVT/PE; Factor V Leiden (most common inherited), prothrombin mutation, protein C/S deficiency, ATIII deficiency, antiphospholipid syndrome (APLS)
Ch. 60 — Enlargement of Lymph Nodes and Spleen (Ch. 65)
- Lymphadenopathy:
- Localised: Drainage territory infection/malignancy; cervical (EBV, head/neck cancer), inguinal (STI, lymphoma), axillary (breast cancer)
- Generalised: EBV, CMV, HIV, SLE, sarcoidosis, lymphoma, leukaemia
- Red flags: Firm/hard/fixed, >2 cm, >4 weeks, B symptoms (fever, night sweats, weight loss), supraclavicular location → biopsy
- Splenomegaly:
- Massive: CML, myelofibrosis, malaria, Gaucher's, hairy cell leukaemia
- Moderate: Lymphoma, portal hypertension, haemolytic anaemia
- Mild: Most infections, SLE, RA (Felty's syndrome)
- Hypersplenism: Pancytopenia from sequestration
Ch. 61 — Disorders of Granulocytes and Monocytes (Ch. 66)
- Neutropenia: ANC <1500; severe <500 → high infection risk (gram-negative bacteraemia, fungal)
- Causes: Drug-induced (chemotherapy, clozapine, carbimazole), viral, aplastic anaemia, SLE, Felty's
- Febrile neutropenia: Oncological emergency — IV broad-spectrum antibiotics within 1h; piperacillin-tazobactam ± aminoglycoside
- Neutrophilia: ANC >7500; causes: bacterial infection, steroid use, AMI, burns, CML
- Eosinophilia: >500; allergic disease, parasites (especially tissue-invasive), EGPA, Addison's, malignancy (Löffler's syndrome)
- Monocytosis: >800; TB, infective endocarditis, CMML, IBD
Ch. 62 — Peripheral Blood Smear (Covered in detail above)
SECTION 10 — MUSCULOSKELETAL
Ch. 63 — Approach to Articular and Musculoskeletal Disease
- Articular vs. periarticular: True joint swelling + restricted active AND passive ROM = articular; periarticular (bursitis, tendinitis) = pain only with resisted active movement
- Inflammatory vs. non-inflammatory:
- Inflammatory: Morning stiffness >1h, warmth, ↑ESR/CRP, systemic features
- Non-inflammatory: Brief stiffness, mechanical, normal inflammatory markers
- Mono- vs. oligo- vs. polyarthritis:
- Monoarthritis: Septic arthritis (emergency), gout, pseudogout, haemarthrosis
- Oligoarthritis (2–4 joints): Reactive arthritis, psoriatic, IBD-associated
- Polyarthritis (>4 joints): RA, SLE, viral arthritis, OA
- Synovial fluid analysis: Cell count, crystals (gout = needle-shaped, negatively birefringent; pseudogout = rhomboid, positively birefringent), Gram stain and culture
Ch. 64 — Osteoporosis
- ↓Bone mineral density (BMD); T-score ≤-2.5 on DEXA = osteoporosis; T-score -1 to -2.5 = osteopaenia
- Risk factors: Female, postmenopausal, ↓calcium/Vit D, smoking, alcohol, steroids, hyperthyroidism, CKD, RA, low BMI
- FRAX score: 10-year fracture probability
- Fragility fractures: Vertebral (most common — often asymptomatic), hip (highest mortality — 20–30% at 1yr), Colles' (distal radius)
- Treatment: Calcium + Vit D → bisphosphonates (alendronate, zoledronate — first-line); denosumab, romosozumab, teriparatide (anabolic — severe/refractory)
- Osteomalacia: Defective mineralisation; ↓Vit D; looser zones; ↑ALP, ↓Ca, ↓PO₄
Ch. 65 — Approach to the Patient with Neurological Disease
- History: Onset (sudden = vascular, gradual = degenerative/mass), location, progression, prior episodes
- Localisation before aetiology: Cortex → subcortex → brainstem → cerebellum → spinal cord → peripheral nerve → NMJ → muscle
- Key neurological examination: Mental status, cranial nerves, motor (tone, power, coordination), reflexes, sensory, gait
- Neuroimaging: CT (quick — haemorrhage, acute stroke); MRI (superior for parenchyma, posterior fossa, spinal cord)
- LP: Meningitis/encephalitis (after CT), SAH, MS (oligoclonal bands), GBS (albuminocytological dissociation)
Ch. 66 — Neuroimaging in Neurological Disease
- CT: Fast, widely available; best for acute haemorrhage, bone, calcification; limited posterior fossa
- MRI: Superior soft tissue contrast; T1 (anatomy — fat bright, CSF dark), T2 (pathology — oedema/CSF bright), FLAIR (suppresses CSF — highlights periventricular lesions in MS), DWI (acute ischaemia — bright within minutes), GRE/SWI (microhaemorrhages)
- MRA/MRV: Non-invasive vascular imaging; aneurysm, AVM, venous sinus thrombosis
- CT angiography: Fast; stroke work-up, aortic dissection
- Functional MRI (fMRI): Pre-surgical mapping of eloquent cortex
- PET: Amyloid PET (Alzheimer's), FDG-PET (epilepsy, tumour vs. radiation necrosis)
- Key patterns:
- MS: Periventricular, juxtacortical, infratentorial T2 lesions; Dawson's fingers
- Acute ischaemic stroke: DWI bright + ADC dark (cytotoxic oedema)
- SAH: Hyperdense CSF in basal cisterns on CT; CT sensitivity ~98% in first 6h
Master Summary Table — Chapters 13–66
| Ch. | Title | Core Concept |
|---|---|---|
| 13 | Pain: Pathophysiology & Management | Nociception, sensitisation, WHO ladder, neuropathic pain |
| 14 | Chest Discomfort | ACS vs. non-cardiac causes; HEART score |
| 15 | Abdominal Pain | Visceral vs. parietal; localisation by quadrant; surgical emergencies |
| 16 | Headache | Migraine/tension/cluster; red flags; thunderclap = SAH |
| 17 | Back & Neck Pain | Mechanical (95%); red flags; disc herniation; cauda equina |
| 18 | Numbness & Sensory Loss | Spinothalamic vs. dorsal column; peripheral vs. central |
| 19 | Weakness & Paralysis | UMN vs. LMN vs. NMJ vs. myopathy |
| 20 | Faintness, Syncope, Vertigo | Reflex/orthostatic/cardiac syncope; BPPV/Ménière's |
| 21 | Syncope | Risk stratification; ROSE rules; cardiac vs. reflex |
| 22 | Fever | Pyrogens; fever vs. hyperthermia; FUO |
| 23 | Fever and Rash | Pattern recognition: petechiae = meningococcaemia |
| 24 | Hypothermia & Frostbite | Core temp; J waves; rewarming strategy |
| 25 | Confusion & Delirium | CAM criteria; hyperactive vs. hypoactive; treat cause |
| 26 | Dementia | AD/VaD/LBD/FTD; reversible causes (B₁₂, NPH, hypothyroid) |
| 27 | Aphasia & Focal Disorders | Broca/Wernicke/Global; neglect; apraxia |
| 28 | Sleep Disorders | OSA/narcolepsy/RLS/insomnia; CBT-I; CPAP |
| 29 | Eye Disorders | Sudden visual loss; RAPD; papilledema; CN III palsy |
| 30 | Smell, Taste & Hearing | Anosmia (COVID/Parkinson's); conductive vs. SNHL |
| 31 | Palpitations | Ectopics/SVT/AF/VT; risk-stratify for SCD |
| 32 | Hypertension | Primary vs. secondary; hypertensive emergency; stepwise Tx |
| 33 | Cardiac Arrest & SCD | BLS/ACLS; post-ROSC care; ICD prevention |
| 34 | Shock | 4 types; septic shock = distributive; vasopressors |
| 36 | Cough & Haemoptysis | Triad of chronic cough; massive haemoptysis management |
| 37 | Dyspnea | Afferent mismatch; descriptors; CPET; opioids for palliation |
| 38 | Hypoxia & Cyanosis | A-a gradient; central vs. peripheral; methaemoglobinaemia |
| 39 | Oedema | Starling forces; cardiac/renal/hepatic/lymphatic causes |
| 40 | ECG Atlas | Systematic reading; STEMI/LVH/LBBB/long QT/Brugada |
| 41 | Nausea, Vomiting & Indigestion | CTZ; antiemetics; alarm features for investigation |
| 42 | Dysphagia | Oropharyngeal vs. oesophageal; achalasia; carcinoma |
| 43 | Diarrhoea & Constipation | Acute/chronic; secretory/osmotic/inflammatory/malabsorptive |
| 44 | Weight Loss | Malignancy in 25%; cachexia; investigate systematically |
| 45 | GI Bleeding | UGIB (PUD/varices) vs. LGIB (diverticulosis); endoscopy |
| 46 | Jaundice | Pre/intra/post-hepatic; Gilbert's; MRCP/ERCP |
| 47 | Ascites & Abdominal Swelling | SAAG ≥1.1 = portal HTN; SBP; hepatorenal syndrome |
| 48 | Azotaemia & Urinary Abnormalities | Pre/intra/post-renal AKI; urinary casts; proteinuria |
| 49 | Fluid & Electrolyte Disturbances | Hypo/hypernatraemia; hypo/hyperkalaemia; acid-base |
| 50 | Acidosis & Alkalosis | AG metabolic acidosis (MUDPILES); respiratory compensation |
| 56 | Approach to Skin Disease | Primary/secondary lesions; distribution; morphology |
| 57 | Common Skin Disorders | Eczema/psoriasis/acne/infections |
| 58 | Skin Manifestations of Internal Disease | Systemic disease → skin clues |
| 59 | Immunologically Mediated Skin Diseases | Pemphigus/pemphigoid/DH |
| 60 | Cutaneous Drug Reactions | SJS/TEN/DRESS/fixed drug eruption |
| 61 | Photosensitivity | Porphyria; drug photosensitivity; photodermatoses |
| 62 | Peripheral Blood Smear | RBC/WBC/platelet morphology in systemic disease |
| 63 | Articular & Musculoskeletal Disease | Articular vs. periarticular; inflammatory vs. mechanical; synovial fluid |
| 64 | Osteoporosis | T-score; FRAX; bisphosphonates; fragility fractures |
| 65 | Approach to Neurological Disease | Localisation; history; examination; investigations |
| 66 | Neuroimaging | CT vs. MRI; DWI/FLAIR/SWI; MS/stroke/SAH patterns |
Key processes and tools in practice of evidence based medicine. Harrisons chapter 4 summary
Harrison's chapter 4 evidence based medicine clinical practice tools processes
evidence based medicine systematic review meta-analysis randomized controlled trial clinical decision making
EBM four steps formulating question searching literature critical appraisal applying evidence patient
sensitivity specificity likelihood ratio NNT NNH absolute relative risk clinical statistics diagnostic testing
Chapter 4 — Evidence-Based Medicine (EBM)
Harrison's Principles of Internal Medicine, 21st Edition
Definition
"Clinical medicine is defined traditionally as a practice combining medical knowledge (including scientific evidence), intuition, and judgment in the care of patients. Evidence-based medicine updates this construct by placing much greater emphasis on the processes by which clinicians gain knowledge of the most up-to-date and relevant clinical research to determine for themselves whether medical interventions alter the disease course and improve the length or quality of life." — Harrison's, p. 269
The 4 Key Steps (Processes) of EBM
Step 1 — Formulate a Focused Clinical Question (PICO)
| Element | Meaning | Example |
|---|---|---|
| P | Patient/Population | Adult with newly diagnosed AF |
| I | Intervention | Apixaban |
| C | Comparison | Warfarin |
| O | Outcome | Stroke, major bleeding, mortality |
- Question types: Therapy, Diagnosis, Prognosis, Harm, Aetiology
- Well-built questions are specific, clinically relevant, and searchable
Step 2 — Search for the Best Available Evidence
| Resource | Description |
|---|---|
| PubMed / MEDLINE | Primary peer-reviewed literature |
| Cochrane Library | Gold standard for systematic reviews and meta-analyses |
| UpToDate / DynaMed | Point-of-care synthesised summaries |
| Clinical Practice Guidelines | Professional society recommendations (AHA, ESC, NICE, WHO) |
| ClinicalTrials.gov | Registered trials; protocol transparency |
| TRIP Database | Evidence-based clinical resources aggregator |
Step 3 — Critically Appraise the Evidence
A. Hierarchy of Evidence (Levels of Evidence)
| Level | Study Type | Strength |
|---|---|---|
| 1a | Systematic review / Meta-analysis of RCTs | Highest |
| 1b | Individual RCT (well-designed) | |
| 2a | Systematic review of cohort studies | |
| 2b | Individual cohort study | |
| 3a | Systematic review of case-control studies | |
| 3b | Individual case-control study | |
| 4 | Case series, case reports | |
| 5 | Expert opinion, mechanistic reasoning | Lowest |
B. Study Design — Key Types
| Design | Key Features | Strengths | Limitations |
|---|---|---|---|
| RCT | Random allocation; blinding; controls | Eliminates confounding; establishes causation | Expensive, time-consuming; may lack external validity |
| Systematic Review / Meta-analysis | Pools multiple studies statistically | High power; reduces random error | Garbage in, garbage out; heterogeneity |
| Cohort Study | Follow exposed vs. unexposed over time | Good for prognosis and rare exposures | Confounding; takes long; attrition bias |
| Case-Control | Compare diseased vs. non-diseased retrospectively | Good for rare diseases; fast; cheap | Recall bias; selection bias; no incidence |
| Cross-Sectional | Snapshot in time; prevalence data | Quick; cheap | Cannot establish causality; no temporality |
| Case Report/Series | Descriptive; individual cases | Hypothesis-generating | No control group; anecdotal |
| N-of-1 Trial | Multiple crossover within single patient | Personalised evidence | Narrow applicability |
C. Assessing Risk of Bias (Internal Validity)
- Was randomisation adequate (allocation concealment)?
- Was blinding implemented (patients, clinicians, outcome assessors)?
- Were all participants accounted for (intention-to-treat analysis)?
- Were groups similar at baseline?
- Was follow-up complete and equal?
| Bias | Definition | Example |
|---|---|---|
| Selection bias | Non-random group assignment | Allocation not concealed |
| Performance bias | Differential care between groups | Unblinded clinicians |
| Detection bias | Outcome assessment influenced by group knowledge | Unblinded outcome assessors |
| Attrition bias | Differential dropout between groups | Per-protocol vs. ITT analysis |
| Reporting bias | Selective publication/reporting of outcomes | Publication bias (positive trials more likely published) |
| Confounding | Third variable associated with both exposure and outcome | Observational studies |
- Cochrane RoB 2 (RCTs)
- ROBINS-I (observational studies)
- GRADE framework (overall quality of evidence → High/Moderate/Low/Very Low)
Step 4 — Apply the Evidence to the Individual Patient
- Best external evidence (research findings)
- Clinical expertise (experience, judgment, knowledge of patient context)
- Patient values and preferences (shared decision-making)
- Is this patient similar to those in the study (external validity/generalisability)?
- Are the outcomes measured the ones that matter to this patient?
- What are the patient's values regarding risk/benefit trade-offs?
Key Tools and Statistical Concepts in EBM
A. Diagnostic Tests
| Measure | Formula | Interpretation |
|---|---|---|
| Sensitivity (Sn) | TP / (TP + FN) | Ability to detect disease; high Sn → good screening test; SnNout (high sensitivity → negative result rules OUT) |
| Specificity (Sp) | TN / (TN + FP) | Ability to confirm absence; high Sp → good confirmatory test; SpPin (high specificity → positive result rules IN) |
| PPV | TP / (TP + FP) | Probability disease present given positive test; depends on prevalence |
| NPV | TN / (TN + FN) | Probability disease absent given negative test; depends on prevalence |
| Likelihood Ratio + | Sn / (1 − Sp) | LR+ >10 = strong evidence of disease |
| Likelihood Ratio − | (1 − Sn) / Sp | LR− <0.1 = strong evidence against disease |
| Pre-test probability | Clinical estimate before test | From history, exam, prevalence |
| Post-test probability | Derived using Bayes' theorem or Fagan nomogram | Pre-test probability + LR → post-test probability |
B. Measures of Treatment Effect
| Measure | Formula | Clinical Use |
|---|---|---|
| Absolute Risk (AR) | Events / Total in group | Baseline risk in control group |
| Absolute Risk Reduction (ARR) | ARcontrol − ARtreatment | Actual reduction in risk attributable to treatment |
| Relative Risk (RR) | ARtreatment / ARcontrol | Risk in treated vs. untreated; RR <1 = benefit |
| Relative Risk Reduction (RRR) | 1 − RR = ARR / ARcontrol | % reduction in risk; can be misleading without ARR |
| Number Needed to Treat (NNT) | 1 / ARR | Number of patients treated for 1 to benefit; lower = better |
| Number Needed to Harm (NNH) | 1 / ARI (absolute risk increase) | Number treated before 1 harm occurs; higher = safer |
| Odds Ratio (OR) | (TP × TN) / (FP × FN) | Used in case-control studies; approximates RR when disease is rare |
| Hazard Ratio (HR) | Instantaneous event rate ratio | Used in survival/time-to-event analyses |
Critical teaching point: RRR is always more impressive-sounding than ARR. A drug reducing events from 2% to 1% has RRR = 50% but ARR = 1% and NNT = 100. Clinicians must focus on ARR and NNT for bedside decision-making.
C. Meta-Analysis Tools
| Tool | Purpose |
|---|---|
| Forest plot | Displays individual study results and pooled estimate; diamond = overall effect; width = CI |
| Funnel plot | Asymmetry suggests publication bias |
| Heterogeneity (I²) | I² >50% = substantial heterogeneity; questions validity of pooling |
| Confidence interval (CI) | Range within which true effect lies 95% of the time; if CI crosses 1.0 (RR/OR/HR) or 0 (ARR) → not statistically significant |
| p-value | Probability of observing results by chance if null hypothesis true; p <0.05 = statistically significant (but does not indicate clinical significance) |
D. GRADE Framework — Evaluating Evidence Quality
| Grade | Meaning |
|---|---|
| High | Confident that true effect is close to estimated effect (usually well-done RCTs) |
| Moderate | Moderate confidence; true effect probably close to estimate |
| Low | Limited confidence; true effect may be substantially different |
| Very Low | Very little confidence; true effect likely different from estimate |
- Strong: "We recommend..." (benefits clearly outweigh risks)
- Weak/Conditional: "We suggest..." (benefits and risks finely balanced or uncertain)
E. Clinical Decision Rules and Scores
| Score | Condition | Purpose |
|---|---|---|
| Wells Score | DVT / PE | Pre-test probability |
| HEART Score | Chest pain / ACS | Risk stratification |
| CHA₂DS₂-VASc | AF | Stroke risk → anticoagulation decision |
| CURB-65 | Pneumonia | Severity → site of care |
| Glasgow Coma Scale | Consciousness | Severity of impaired consciousness |
| Child-Pugh / MELD | Liver disease | Prognosis; transplant listing |
| Framingham Risk Score | Cardiovascular | 10-year CVD risk |
| FRAX | Osteoporosis | 10-year fracture risk |
F. Shared Decision-Making (SDM)
- Clinician provides: Evidence (risks, benefits, alternatives), clinical expertise
- Patient provides: Values, preferences, life goals, acceptable risk threshold
- Together decide: Best option for that individual
- Evidence is uncertain or conflicting
- Multiple equivalent options exist
- Treatment involves significant trade-offs (e.g., cancer screening, elective surgery, anticoagulation)
Limitations of EBM
| Limitation | Explanation |
|---|---|
| Evidence gaps | Many clinical questions lack RCT evidence |
| External validity | Trial populations often differ from real patients (elderly, comorbid, polypharmacy excluded) |
| Publication bias | Positive trials more likely published; negative/null results suppressed |
| Surrogate outcomes | Many trials measure surrogate endpoints (HbA1c, BP) not patient-important outcomes (mortality, QoL) |
| Time lag | Evidence-to-practice gap averages 17 years |
| Overreliance on p-values | Statistical significance ≠ clinical significance |
| Conflicts of interest | Industry-funded trials more likely to show positive results |
| Individual variation | Average RCT results may not apply to individual patients |
Summary: EBM in Practice
Clinical Uncertainty
↓
Step 1: PICO Question
↓
Step 2: Search (PubMed, Cochrane, Guidelines)
↓
Step 3: Appraise (Study design → Bias → Statistics)
↓
Level of evidence (GRADE)
↓
NNT / ARR / LR / CI
↓
Step 4: Apply to patient
↓
Clinical expertise + Patient values
↓
Shared Decision-Making
↓
Best individualised care
Key Teaching Points (Harrison's Ch. 4)
- EBM does not replace clinical judgment — it enhances it by combining evidence, expertise, and patient values
- RCTs are not always the answer — for rare diseases, long latency outcomes, or ethical constraints, observational studies may be the best available evidence
- Always distinguish statistical significance from clinical significance
- NNT and ARR are more clinically useful than RRR — always calculate when appraising therapy trials
- Sensitivity/specificity are fixed properties of a test; PPV/NPV change with disease prevalence — critical for interpreting tests in low vs. high prevalence populations
- LRs are the most useful single statistic for diagnostic test interpretation as they are independent of prevalence when using Bayesian reasoning
- GRADE is the current gold standard for rating evidence quality and translating it into clinical recommendations
- The 17-year evidence-to-practice gap underscores the importance of clinicians actively engaging with the primary literature
Basic principles of screening. Uses and abuses of screening tests. Harrisons chapter 6 based short summary
Harrison's chapter 6 screening principles disease prevention early detection
screening test criteria validity reliability sensitivity specificity lead time bias length bias overdiagnosis
screening principles Wilson Jungner criteria disease test population benefit harm balance
lead time bias screening cancer survival mortality surrogate endpoint uses abuses overdiagnosis overtreatment
Chapter 6 — Screening and Prevention of Disease
Harrison's Principles of Internal Medicine, 21st Edition
"This chapter reviews the basic principles of screening and prevention in the primary care setting." — Harrison's, p. 302
Definition of Screening
- Distinguished from diagnostic testing (applied to symptomatic individuals)
- Screening is applied to apparently healthy populations
- The fundamental goal: detect disease at a pre-symptomatic stage when treatment is more effective
Levels of Prevention
| Level | Definition | Examples |
|---|---|---|
| Primary prevention | Prevent disease occurrence | Vaccination, smoking cessation, statins, folic acid in pregnancy |
| Secondary prevention | Detect disease early before symptoms | Mammography, cervical smear, colonoscopy, BP measurement |
| Tertiary prevention | Reduce impact of established disease | Cardiac rehabilitation, diabetic foot care, stroke physiotherapy |
| Quaternary prevention | Protect from overmedicalisation | Avoiding unnecessary screening, overdiagnosis, overtreatment |
Basic Principles of Screening — Wilson and Jungner Criteria (WHO, 1968)
| # | Criterion | Explanation |
|---|---|---|
| 1 | The condition should be an important health problem | Significant burden — high prevalence, morbidity, or mortality |
| 2 | There should be an accepted treatment for patients with recognised disease | No point detecting disease if no effective intervention exists |
| 3 | Facilities for diagnosis and treatment should be available | Healthcare infrastructure must support follow-up |
| 4 | There should be a recognisable latent or early symptomatic stage | Detectable window between onset and clinical presentation |
| 5 | There should be a suitable test or examination | The test must be acceptable, safe, valid, and reliable |
| 6 | The test should be acceptable to the population | High uptake required for programme effectiveness |
| 7 | The natural history of the condition should be adequately understood | Must know the disease's progression to interpret screening findings |
| 8 | There should be an agreed policy on whom to treat as patients | Clear diagnostic thresholds and management pathways |
| 9 | The cost of case-finding should be economically balanced | Cost-effectiveness analysis; cost per quality-adjusted life year (QALY) |
| 10 | Case-finding should be a continuing process | Not a one-time event; requires periodic re-screening |
Properties of an Ideal Screening Test
A. Validity — Does the test measure what it is meant to measure?
| Property | Formula | Interpretation |
|---|---|---|
| Sensitivity | TP / (TP + FN) | Ability to correctly identify those WITH disease; high Sn → few false negatives; SnNout |
| Specificity | TN / (TN + FP) | Ability to correctly identify those WITHOUT disease; high Sp → few false positives; SpPin |
| PPV | TP / (TP + FP) | Probability of disease given positive test; rises with prevalence |
| NPV | TN / (TN + FN) | Probability of no disease given negative test; falls with prevalence |
Critical point: In low-prevalence screening populations, even a highly specific test generates many false positives — driving unnecessary investigations, anxiety, and harm. This is the fundamental tension in population screening.
B. Reliability (Reproducibility)
- Consistency of results when the test is repeated under same conditions
- Intra-observer and inter-observer variability must be minimised
- Assessed by kappa statistic (κ >0.8 = excellent agreement)
C. Yield
- Number of previously unrecognised cases detected per number screened
- Influenced by: prevalence, test sensitivity, and screening interval
D. Acceptability
- Non-invasive, affordable, with minimal discomfort
- Respects cultural, ethical, and personal patient values
The Screening Process — Key Steps
Define target population (age, sex, risk group)
↓
Apply screening test (first-line, usually cheap/safe/sensitive)
↓
Screen-positive individuals
↓
Diagnostic confirmation (gold standard test)
↓
Treatment / intervention
↓
Outcome monitoring and programme evaluation
Uses of Screening Tests
1. Population-Based (Mass) Screening
- Cervical cancer screening (Pap smear / HPV test)
- Breast cancer (mammography)
- Colorectal cancer (faecal occult blood test / colonoscopy)
- Newborn metabolic screening (PKU, hypothyroidism, CF)
- Neonatal hearing screening
2. Selective (Targeted / High-Risk) Screening
- BRCA1/2 testing in women with strong family history of breast/ovarian cancer
- Lung cancer screening (low-dose CT) in heavy smokers aged 50–80
- Hepatocellular carcinoma screening (USS liver ± AFP) in cirrhosis/hepatitis B
- Abdominal aortic aneurysm (USS) in male smokers aged 65+
- TB screening in healthcare workers, immigrants from endemic areas
3. Opportunistic Screening
- Blood pressure measurement at any GP visit
- Fasting glucose/HbA1c in overweight patients
- Cholesterol in cardiovascular risk assessment
4. Multiphasic Screening
- Health checks (NHS Health Check in UK — BP, cholesterol, glucose, BMI)
- Executive health screenings
Abuses and Limitations of Screening — Critical Biases
1. Lead Time Bias
Without screening: Diagnosis ──────────────────► Death
← Survival time →
With screening: Diagnosis ──────────────────────────► Death
↑ (earlier)
← Longer "survival" → (same death date)
- The patient appears to "survive longer" after diagnosis, but dies at the same time
- Survival time is measured from diagnosis → death; earlier diagnosis inflates this without any true benefit
- Corrective measure: Use disease-specific mortality rates (deaths per 100,000 per year) as the outcome, NOT 5-year survival rates
Example: If screening detects cancer 2 years earlier but treatment does not change the death date, 5-year survival improves from 0% to 100% purely due to lead time — with no actual benefit.
2. Length-Biased Sampling (Length Time Bias)
Slow-growing tumour: ─────────────────────────────► (long window, screen catches it)
Fast-growing tumour: ──────► (short window, screen misses it → symptomatic)
- Screened populations therefore contain a disproportionately large number of indolent cancers with inherently good prognosis — inflating apparent screening benefit
- The patients who most need early detection (aggressive cancers) are least likely to be caught
3. Overdiagnosis and Overtreatment
- An extreme form of length-biased sampling
- The reservoir of slow-growing, clinically insignificant tumours is large
- Problem compounded by competing causes of death in elderly patients
- Consequences: Unnecessary surgery, radiation, chemotherapy, psychological harm, financial cost
| Cancer | Magnitude |
|---|---|
| Prostate cancer (PSA) | Estimated 25–50% of screen-detected cases are overdiagnosed |
| Thyroid cancer | Epidemic of small papillary thyroid cancers detected on USS — most would never cause symptoms |
| Breast cancer (DCIS) | Ductal carcinoma in situ: not all progress to invasive cancer |
| Lung cancer (LDCT) | ~18% overdiagnosis estimated in NLST trial |
| Melanoma | Increasing incidence without proportional increase in mortality |
4. Selection Bias (Healthy Screener Effect / Volunteer Bias)
- Screened populations have lower all-cause mortality than unscreened populations even for unrelated diseases
- Makes screening appear more effective than it truly is
- Corrective measure: Randomised controlled trials of screening (randomise to screened vs. unscreened), not observational comparisons
5. Will Rogers Phenomenon (Stage Migration Bias)
Named after the quote: "When the Okies left Oklahoma and moved to California, they raised the average intelligence in both states."
- Example: CT staging detects micrometastases previously missed → patients previously stage II become stage III → stage II survival improves (sicker patients removed) AND stage III survival improves (less sick patients added)
- Net effect: Survival in every stage improves with no actual benefit to patients
6. False Positives — Harms of Screening
- Anxiety and psychological distress (even after negative confirmatory test)
- Unnecessary investigations: Invasive, expensive, risky (e.g., lung nodule follow-up CT scans, colposcopy, breast biopsy)
- Cascading investigations: One false positive leading to multiple downstream tests
- Overtreatment: Treatment of conditions that would never have caused harm
Example: Low-dose CT lung screening — for every 1,000 scans, ~200 abnormalities detected; vast majority are benign, leading to repeated imaging and occasional invasive procedures.
7. False Negatives — Harms of Screening
- False reassurance → patient ignores subsequent symptoms
- Missed cancers between screening intervals = interval cancers (often more aggressive)
- Reduces the positive predictive value of subsequent symptoms
8. Medicalisation and Psychological Harm
- Labelling effect: Being told one has a "borderline" or "pre-disease" state (pre-diabetes, pre-hypertension, DCIS) causes anxiety, reduces quality of life, and may lead to unnecessary treatment
- Surveillance burden: Serial investigations, appointments, and follow-up cause long-term psychological stress
- Healthy individuals converted into patients
Evaluating a Screening Programme — What Outcomes Matter?
| Outcome | Validity | Comment |
|---|---|---|
| Disease-specific mortality | High | Most important — does screening reduce deaths from the disease? |
| All-cause mortality | Highest | Does screening reduce total deaths? (Avoids misclassification of cause of death) |
| 5-year survival rate | Low — misleading | Profoundly affected by lead time bias and length bias; DO NOT USE to evaluate screening |
| Incidence (stage shift) | Moderate | More early-stage diagnoses is proxy for benefit but must accompany mortality reduction |
| Quality of life (QoL) | High | Overdiagnosis and overtreatment reduce QoL even if mortality unchanged |
The most important principle: A screening test must be evaluated by randomised controlled trial measuring disease-specific or all-cause mortality — not by case series or cohort studies showing improved survival.
Balancing Benefits and Harms — The Core Ethical Tension
| Dimension | Consideration |
|---|---|
| Benefit | Reduction in disease-specific mortality; early, less morbid treatment |
| Harm | False positives, overdiagnosis, overtreatment, anxiety, invasive follow-up |
| Autonomy | Informed consent; patients must understand limitations |
| Equity | Screening must reach high-risk and disadvantaged populations equally |
| Cost-effectiveness | Cost per QALY gained; opportunity cost vs. other health interventions |
- What the test is designed to detect
- The possibility of false-positive and false-negative results
- What further investigations a positive result would entail
- The risk of overdiagnosis and overtreatment
- The potential benefits in terms of reduced mortality
Examples of Current Evidence-Based Screening Programmes
| Condition | Test | Target Population | Evidence |
|---|---|---|---|
| Cervical cancer | HPV test / Pap smear | Women 25–65 every 3–5 years | Strong — mortality ↓ |
| Breast cancer | Mammography | Women 40–74 every 1–2 years | Moderate — 20% mortality ↓; overdiagnosis significant |
| Colorectal cancer | FIT / colonoscopy / sigmoidoscopy | Age 45–75 | Strong — mortality ↓ |
| Lung cancer | Low-dose CT (LDCT) | Smokers 50–80, ≥20 pack-years | Moderate (NLST/NELSON) — 20–26% lung cancer mortality ↓ |
| AAA | Abdominal USS | Male smokers aged 65 | Strong — mortality ↓ |
| Hypertension | BP measurement | All adults every 1–2 years | Strong — stroke/CVD ↓ |
| Diabetes | Fasting glucose / HbA1c | Overweight/obese adults | Moderate |
| Osteoporosis | DEXA scan | Women ≥65, high-risk younger | Moderate — fracture ↓ |
| Prostate cancer (PSA) | PSA | Men 50–70 (controversial) | Weak — significant overdiagnosis; shared decision-making essential |
| Newborn metabolic | Heel prick (PKU, hypothyroid etc.) | All neonates | Strong |
Summary Table — Uses vs. Abuses
| Uses of Screening | Abuses / Limitations |
|---|---|
| Detects disease in pre-symptomatic stage | Lead time bias falsely inflates survival |
| Enables earlier, less morbid treatment | Length bias preferentially detects indolent disease |
| Reduces disease-specific mortality (when evidence-based) | Overdiagnosis — treating pseudo-disease |
| Identifies high-risk individuals for targeted prevention | False positives → anxiety, unnecessary investigations |
| Population-level health improvement | False negatives → false reassurance |
| Cost-effective when properly designed | Volunteer/healthy screener bias in observational data |
| Guides resource allocation | Stage migration (Will Rogers) distorts statistics |
| Satisfies patient autonomy when properly consented | Medicalisation of healthy individuals |
| Overtreatment → net harm in some programmes | |
| Inequitable access may widen health disparities |
Key Teaching Points (Harrison's Ch. 6)
- Screening must satisfy Wilson-Jungner criteria — most importantly, treatment must be available and early detection must confer genuine benefit
- 5-year survival is a useless metric for evaluating screening — always use disease-specific mortality rates from RCTs
- Lead time bias and length bias are the two most important reasons why screening trials must be randomised
- Overdiagnosis is the most underappreciated harm of modern screening — most prominent in prostate, thyroid, breast, and lung cancer screening
- In low-prevalence populations, even highly specific tests generate predominantly false positives — PPV collapses as prevalence falls
- PSA screening remains the textbook example of a controversial screening test: reduces metastatic prostate cancer but with substantial overdiagnosis and overtreatment
- Screening is not risk-free — it is an intervention offered to healthy people, requiring a higher ethical standard and genuine informed consent
- The most valuable screening programmes combine high sensitivity (to not miss disease) at the first-line test with high specificity at the confirmatory diagnostic test
Bayes rule in diagnostic probability. Discuss tools for assessment of quality of healthcare
Bayes theorem diagnostic probability pretest posttest probability likelihood ratio clinical medicine Harrison's
quality of healthcare assessment tools measures indicators patient safety outcome process structure Donabedian
Bayes rule pretest probability sensitivity specificity positive negative predictive value Fagan nomogram clinical decision
healthcare quality improvement tools patient safety indicators benchmarking accreditation error reporting clinical audit
Part I — Bayes' Rule in Diagnostic Probability
Harrison's Principles of Internal Medicine, 21st Edition — Chapter 4
The Core Concept
The Fagan nomogram version of Bayes' rule "helps us understand at a conceptual level how it estimates the posttest probability of disease... the impact of the diagnostic test result is summarized by the likelihood ratio, defined as the ratio of the probability of a given test result in a patient with disease to the probability of that result in a patient without disease." — Harrison's, p. 261
Foundational Definitions
| Term | Definition |
|---|---|
| Pre-test probability | Probability of disease before the test is applied; derived from prevalence, clinical history, examination, and risk factors |
| Post-test probability | Revised probability of disease after incorporating the test result |
| Sensitivity (Sn) | TP / (TP + FN) — probability of positive test given disease present |
| Specificity (Sp) | TN / (TN + FP) — probability of negative test given disease absent |
| Likelihood Ratio (LR) | How much a test result changes the pre-test probability |
Bayes' Theorem — The Formula
Classic Form
- P(D) = pre-test probability (prevalence)
- P(T+|D) = sensitivity
- P(T+|D̄) = 1 − specificity (false positive rate)
- P(D|T+) = post-test probability (PPV in population terms)
Simplified Practical Form Using Odds
The Bedside Bayes Formula (Using LR)
Likelihood Ratios — The Key Tool
Definition
Interpretation of LR Values
| LR+ Value | Interpretation | Change in Probability |
|---|---|---|
| >10 | Large, often conclusive increase | +45% approx |
| 5–10 | Moderate increase | +30% approx |
| 2–5 | Small increase | +15% approx |
| 1–2 | Minimal/negligible | +0–5% |
| 1 | No diagnostic value | 0% |
| LR− Value | Interpretation | Change in Probability |
|---|---|---|
| <0.1 | Large, often conclusive decrease | −45% approx |
| 0.1–0.2 | Moderate decrease | −30% approx |
| 0.2–0.5 | Small decrease | −15% approx |
| 0.5–1 | Minimal/negligible | 0–5% |
Key insight: LRs are independent of prevalence — unlike PPV and NPV, they are properties of the test alone and can be applied to any pre-test probability using Bayesian reasoning.
Worked Clinical Example
- Sensitivity = 68%, Specificity = 77%
- LR+ = 0.68 / (1 − 0.77) = 2.96
The Fagan Nomogram
Pre-test Likelihood Post-test
Probability Ratio Probability
99% ──────────── 1000 ─────────────── 99%
500
95% ──────────── 200 ──────────────── 95%
100
90% ──────────── 50 ──────────────── 90%
20
75% ──────────── 10 ──────────────── 75%
50% ──────────── 5 ──────────────── 50%
2
25% ──────────── 1 ──────────────── 25%
10% ──────────── 0.5 ──────────────── 10%
5% ──────────── 0.2 ──────────────── 5%
0.1
1% ──────────── 0.05 ─────────────── 1%
The Threshold Model of Clinical Decision-Making
0%─────────────[Test threshold]────────[Treatment threshold]──────100%
│ │ │
Disease Test to Treat without
so unlikely further clarify testing
no test needed probability
| Zone | Action |
|---|---|
| Below test threshold | Disease unlikely enough — no testing needed |
| Between thresholds | Uncertainty zone — testing will change management |
| Above treatment threshold | Disease likely enough — treat empirically without waiting for test |
Testing is only worthwhile when the pre-test probability lies between the test and treatment thresholds — and when the test result will change clinical management.
Pre-Test Probability — How to Estimate It
| Method | Description |
|---|---|
| Disease prevalence | Population base rate; from epidemiological data |
| Clinical prediction rules | Wells score (DVT/PE), HEART score (ACS), Centor (strep pharyngitis) |
| History and examination | Most powerful tool; symptom typicality, risk factors, exam findings |
| Clinician gestalt | Experienced clinician's integrated impression (validated in some studies) |
| Published probability tables | Pre-test probabilities for specific symptom/sign combinations |
Key Limitations of Bayesian Reasoning in Practice
| Limitation | Explanation |
|---|---|
| Pre-test probability is subjective | Estimation varies between clinicians; anchoring bias |
| LRs assume test independence | Multiple sequential tests cannot simply be chained (results often correlated) |
| Spectrum bias | LRs derived from populations with different disease spectrum may not apply |
| Threshold uncertainty | Test and treatment thresholds are not always clearly defined |
| Patient values ignored | Pure Bayesian reasoning does not incorporate patient preferences for certainty |
| Continuous test results ignored | Binary positive/negative LRs lose information from continuous variables (e.g., troponin levels) |
Part II — Tools for Assessment of Quality of Healthcare
Harrison's Principles of Internal Medicine, 21st Edition
Donabedian's Triad — The Foundational Framework
"Donabedian has suggested that quality of care can be categorised by type of measurement into structure, process, and outcome."
1. Structure
- Physical resources: Hospital beds, equipment, catheterisation laboratory, ICU
- Human resources: Staffing ratios, nurse-to-patient ratio, specialist availability
- Organisational features: Electronic health records (EHR), protocols, accreditation status
- Example: Does the hospital have a primary PCI-capable catheterisation laboratory?
2. Process
- Whether aspirin was given to a patient with suspected MI (Harrison's, p. 356)
- Whether a Pap smear was performed at the recommended interval (Harrison's, p. 356)
- Whether hand hygiene was performed before invasive procedures
- Whether a DVT prophylaxis protocol was followed
- Example: Door-to-balloon time <90 minutes in STEMI
3. Outcome
- Mortality rates (30-day, 1-year)
- Complication rates (surgical site infection, readmission, hospital-acquired infection)
- Patient-reported outcomes (pain, function, quality of life)
- Example: 30-day mortality after MI, hospital-acquired pressure ulcer rate
"It is important to note that good structure and process do not always result in a good outcome. A patient may present with suspected MI to an institution with a catheterisation laboratory and receive recommended care including aspirin, but still die because of the infarction." — Harrison's, p. 356
| Domain | Advantages | Limitations |
|---|---|---|
| Structure | Easy to measure; reproducible | Poor direct link to outcomes |
| Process | Reflects evidence-based care delivery; actionable | May not always correlate with outcomes |
| Outcome | Directly patient-relevant | Confounded by case mix; needs risk adjustment; delayed measurement |
Tools for Quality Measurement and Improvement
1. Clinical Audit
- Systematic review of clinical care against explicit standards
- Audit cycle: Set standard → Measure practice → Compare to standard → Implement change → Re-audit (close the loop)
- Example: Audit of antibiotic prescription within 1 hour for sepsis against NICE guidelines
- Limitation: Descriptive — identifies gaps but does not establish causation
2. Key Performance Indicators (KPIs) and Quality Indicators
| Type | Examples |
|---|---|
| Clinical effectiveness | HbA1c <53 mmol/mol in diabetics, BP <140/90, statin prescription post-MI |
| Patient safety | Medication error rate, wrong-site surgery rate, falls rate per 1000 bed days |
| Patient experience | Friends and Family Test, CAHPS survey, complaints rate |
| Access/timeliness | Door-to-balloon <90 min, A&E 4-hour target, cancer 2-week wait rule |
| Efficiency | Average length of stay, readmission within 30 days, bed occupancy rate |
3. Balanced Scorecard
| Perspective | Healthcare Application |
|---|---|
| Financial | Cost per episode, budget variance, revenue cycle |
| Customer (Patient) | Patient satisfaction scores, complaints, PROMS |
| Internal processes | Waiting times, adherence to protocols, infection rates |
| Learning and growth | Staff training, turnover, innovation adoption |
4. Plan-Do-Study-Act (PDSA) Cycle
PLAN
↗ ↘
ACT DO
↖ ↙
STUDY
- Plan: Identify problem, set objective, predict outcome
- Do: Implement change on small scale (pilot)
- Study: Analyse results; compare to prediction
- Act: Standardise if successful; modify and repeat if not
5. Root Cause Analysis (RCA)
- Structured retrospective review of adverse events or near-misses
- Goal: Identify systemic (not individual) causes of failure
- Tools within RCA:
- Fishbone diagram (Ishikawa): Categorises causes into Man, Machine, Method, Material, Measurement, Environment (6Ms)
- 5 Whys: Ask "why?" repeatedly until root cause reached
- Fault Tree Analysis: Logical diagramming of failure pathways
- Outcome: Systemic recommendations, not blame allocation
6. Failure Mode and Effects Analysis (FMEA)
- Prospective (proactive) risk assessment tool — used before an adverse event
- Identify potential failure modes in a process → assess their likelihood, severity, and detectability
- Calculate Risk Priority Number (RPN) = Severity × Occurrence × Detectability
- Prioritise interventions for highest RPN failures
- Widely used in pharmacy, surgery, and radiology workflows
7. Statistical Process Control (SPC) Charts
- Monitor quality indicators over time using statistical rules
- Distinguish common cause variation (inherent process variability — expected) from special cause variation (unexpected signals requiring investigation)
- Control limits = ±3 standard deviations from mean
- Types: P-charts (proportions), U-charts (rates), XmR charts (individual measurements)
- Advantage over simple audit: Detects trends and shifts in performance before they become crises
UCL ─ ─ ─ ─ ─ ─ ─ ─ ─ ─ ─ ─ ─ ─ ─ ─
● ● ●
Mean ────────────────●────────●────●────────────
● ● ●
LCL ─ ─ ─ ─ ─ ─ ─ ─ ─ ─ ─ ─ ─ ─ ─ ─
8. Benchmarking
- Comparing an institution's performance against:
- Internal benchmark: Own historical performance
- External benchmark: Peer institutions or national standards
- Best practice benchmark: Against the highest performers
- Requires risk adjustment for fair comparison (case-mix, comorbidities, deprivation indices)
- Tools: NHS Model Hospital, CMS Hospital Compare, Dr Foster Intelligence, OECD Health Statistics
9. Patient-Reported Outcome Measures (PROMs) and Experience Measures (PREMs)
| Tool | What it Measures |
|---|---|
| PROMs | Health outcomes from patient's perspective (pain, function, QoL) — e.g., EQ-5D, Oxford Hip Score |
| PREMs | Patient's experience of care process — e.g., communication, dignity, responsiveness |
| CAHPS | Consumer Assessment of Healthcare Providers and Systems (USA) |
| Friends and Family Test | NHS UK: "Would you recommend this service?" |
| NPS (Net Promoter Score) | Promoters minus detractors as overall satisfaction metric |
10. Accreditation and External Review
- Joint Commission (USA) / CQC (UK) / JCI (International): External bodies that assess healthcare organisations against defined standards
- Surveys, inspections, and continuous monitoring
- Focuses on structure + process standards
- Magnet Status (nursing excellence), ISO 9001 (quality management systems)
11. Mortality and Morbidity (M&M) Conferences
- Regular multidisciplinary review of adverse outcomes and near-misses
- Non-punitive, educational environment
- Identifies system failures, near-misses, and learning opportunities
- Basis for departmental quality improvement initiatives
12. Incident Reporting Systems
- Voluntary reporting of adverse events, near-misses, and unsafe conditions
- Examples: NHS National Reporting and Learning System (NRLS), FDA MedWatch, WHO Global Patient Safety Network
- Chronic underreporting (estimated 10–30% of incidents reported)
- Heinrich's Triangle: For every serious injury, there are ~29 minor injuries and 300 near-misses
13. Patient Safety Indicators (PSIs)
- Hospital-acquired infections (HAI): MRSA, CDiff, CAUTI, CLABSI, VAP
- Surgical complications: Wrong-site surgery, retained foreign body, anastomotic leak
- Medication errors: Wrong drug, wrong dose, wrong patient
- Falls with injury
- Pressure ulcers (hospital-acquired)
- Venous thromboembolism in surgical patients
14. Six Sigma
- Data-driven methodology for eliminating defects: Target = 3.4 defects per million opportunities
- DMAIC framework: Define → Measure → Analyse → Improve → Control
- Originally industrial (Motorola/GE); increasingly applied in healthcare (reducing medication errors, surgical complications)
15. Lean Methodology
- Derived from Toyota Production System
- Core principle: Eliminate waste (Muda) in processes — 8 types of waste:
- DOWNTIME: Defects, Overproduction, Waiting, Non-utilised talent, Transportation, Inventory, Motion, Extra-processing
- Tools: Value stream mapping, 5S (Sort, Set, Shine, Standardise, Sustain), Kaizen (continuous improvement)
- Applied in: ED flow, surgical throughput, pharmacy dispensing, outpatient scheduling
Summary Table — Quality Tools at a Glance
| Tool | Type | Primary Use |
|---|---|---|
| Donabedian Triad | Framework | Categorising quality measures |
| Clinical Audit | Measurement | Gap analysis against standards |
| KPIs / Quality Indicators | Measurement | Monitoring ongoing performance |
| Balanced Scorecard | Strategic | Organisation-wide performance management |
| PDSA Cycle | Improvement | Iterative small-scale change testing |
| Root Cause Analysis | Safety | Reactive adverse event investigation |
| FMEA | Safety | Proactive risk identification |
| SPC Charts | Measurement | Trend monitoring over time |
| Benchmarking | Measurement | Comparative performance assessment |
| PROMs / PREMs | Patient-centred | Patient perspective on outcomes and experience |
| Accreditation | External review | Institutional standards compliance |
| M&M Conferences | Safety/Learning | Peer case review and learning |
| Incident Reporting | Safety | Voluntary adverse event capture |
| Six Sigma | Improvement | Defect reduction to near-zero |
| Lean | Improvement | Waste elimination and process efficiency |
Synthesis — Connecting Bayes and Quality
| Bayesian Reasoning | Quality Improvement |
|---|---|
| Uses prior probability + new data → updated probability | Uses baseline performance + intervention → improved outcome |
| Iterative updating with each new test | Iterative PDSA cycles |
| Quantifies uncertainty explicitly | SPC charts quantify variation explicitly |
| Pre-test probability = baseline prevalence | Baseline KPI = starting performance |
| LR = the power of new information | Effect size = the power of an intervention |
| Post-test probability = revised clinical estimate | Post-intervention KPI = new performance level |
Pcos
Polycystic Ovary Syndrome (PCOS)
Definition
- Hyperandrogenism (HA) — clinical or biochemical
- Ovulatory dysfunction — oligo/anovulation
- Polycystic ovarian morphology on ultrasound
Pathophysiology
1. GnRH Pulse Abnormality
- Abnormalities in GnRH pulsatility → elevated LH pulse frequency and amplitude
- ↑ LH → stimulates ovarian theca cells → excess androgen (testosterone, androstenedione) production
- Relatively low or normal FSH → impaired follicular maturation and anovulation
2. Ovarian Androgen Excess
- Theca cells in PCOS over-respond to LH stimulation
- Elevated androgens → peripheral conversion to oestrone → unopposed oestrogen → positive feedback on LH → further LH excess (vicious cycle)
- 11-oxygenated androgens (e.g., 11-ketotestosterone) may also be elevated — an alternate androgen source
3. Insulin Resistance and Hyperinsulinaemia
- Insulin resistance — predominantly in skeletal muscle and adipose tissue — is present in 50–80% of women with PCOS
- Compensatory hyperinsulinaemia → directly stimulates ovarian androgen production (insulin receptors on theca cells are preserved even when peripheral resistance exists)
- Insulin also ↓ hepatic SHBG production → more free (unbound) testosterone circulates
- Obesity worsens insulin resistance and the PCOS phenotype significantly
4. Follicular Arrest
- Excess androgens and insulin → accumulation of small antral follicles arrested at 2–9 mm
- None reaches dominance → anovulation persists
- Gives the characteristic "string of pearls" appearance on USS
5. Genetic Basis
- Genome-wide association studies (GWAS) have identified ~19 loci associated with PCOS across diverse populations (Harrison's 22E)
- Cluster analyses reveal reproductive and metabolic subtypes
- Likely polygenic and multifactorial inheritance
- Familial concordance: sisters and mothers of PCOS patients have higher rates of PCOS
Diagnostic Criteria
Rotterdam Criteria (2003) — Most Widely Used
| Criterion | Definition |
|---|---|
| 1. Oligoovulation or anovulation | Irregular cycles: <8 periods/year, or cycle length >35 days |
| 2. Clinical or biochemical hyperandrogenism | Hirsutism (mFG score ≥4–6, ethnicity-dependent), acne, alopecia; OR elevated total/free testosterone |
| 3. Polycystic ovarian morphology (PCOM) | ≥20 antral follicles in at least one ovary, OR ovarian volume ≥10 cm³; OR elevated AMH (updated 2023 criteria, Harrison's 22E) |
Diagnostic Phenotypes (4 Rotterdam Phenotypes)
| Phenotype | HA | Ovulatory Dysfunction | PCOM |
|---|---|---|---|
| A (Classic) | ✓ | ✓ | ✓ |
| B | ✓ | ✓ | ✗ |
| C (Ovulatory PCOS) | ✓ | ✗ | ✓ |
| D (Non-androgenic) | ✗ | ✓ | ✓ |
Phenotype A is most severe metabolically; Phenotype D is mildest.
NIH 1990 Criteria (Stricter — Both Required)
- Chronic anovulation
- Clinical and/or biochemical hyperandrogenism + exclusion of other causes
Special Populations
- Adolescents: Diagnosis requires both irregular menses AND hyperandrogenism; ultrasound and AMH criteria are not used (multi-follicular ovaries and elevated AMH are normal in adolescence); wait at least 3 years post-menarche before confirming (Harrison's 22E)
- Lean PCOS: High LH with normal-low FSH and oestradiol; insulin resistance still present in ~30%
Exclusion Criteria — Diagnoses to Rule Out
| Condition | Key Distinguishing Feature |
|---|---|
| Hypothyroidism | ↑ TSH; treat before diagnosing PCOS |
| Hyperprolactinaemia | ↑ Prolactin; pituitary adenoma |
| Non-classic CAH (21-hydroxylase deficiency) | ↑ 17-OH progesterone (>2 ng/mL); rapid-onset virilisation |
| Cushing's syndrome | ↑ 24h urinary cortisol, midnight salivary cortisol; central obesity, striae, bruising |
| Androgen-secreting tumour | Rapid onset hirsutism + virilisation; very high testosterone (>5 nmol/L or DHEAS markedly elevated) |
| Hypogonadotrophic hypogonadism | ↓ LH, ↓ FSH, ↓ oestrogen; hypothalamic dysfunction |
| Primary ovarian insufficiency | ↑ FSH, ↓ AMH, age <40 |
Clinical Features
Menstrual Disturbance
- Oligomenorrhoea (most common) — cycles >35 days
- Amenorrhoea — primary or secondary
- Irregular uterine bleeding
- Rarely, normal cycles with biochemical hyperandrogenism
Hyperandrogenism
- Hirsutism: Coarse terminal hair in androgen-sensitive areas (upper lip, chin, chest, abdomen, inner thighs) — assessed by modified Ferriman-Gallwey (mFG) score (≥4–6 abnormal, ethnicity-dependent)
- Acne: Persistent, adult-onset
- Androgenic alopecia: Temporal recession, central thinning
- Virilisation (clitoromegaly, voice deepening) is RARE and suggests tumour
Metabolic Features
- Obesity: Present in 40–80% of PCOS patients in Western populations; central (android) distribution
- Insulin resistance: Present in ~50–80%; leads to acanthosis nigricans (velvety hyperpigmentation at neck, axillae)
- Metabolic syndrome: ↑ waist circumference, ↑ triglycerides, ↓ HDL, hypertension, impaired fasting glucose
- Type 2 diabetes: 5–10× higher risk; impaired glucose tolerance in 30–35%
- Dyslipidaemia: ↑ LDL, ↑ TG, ↓ HDL
Reproductive Features
- Infertility: Most common cause of anovulatory infertility
- Subfertility: Infrequent ovulation
- Pregnancy complications: ↑ risk of miscarriage, gestational diabetes, gestational hypertension, pre-eclampsia, preterm birth (Harrison's 22E)
Long-Term Health Risks
- Endometrial cancer: 2–6× increased risk from unopposed oestrogen due to chronic anovulation (Harrison's 22E)
- Cardiovascular disease: ↑ risk from metabolic syndrome, dyslipidaemia, hypertension; however, direct evidence of increased CV mortality remains debated
- Obstructive sleep apnoea (OSA): Independent of BMI (Harrison's 22E)
- Metabolic dysfunction-associated steatotic liver disease (MASLD/MAFLD): Independent of BMI (Harrison's 22E)
- Depression and anxiety: High prevalence; body image distress and disordered eating (Harrison's 22E)
Investigations
Baseline (All patients)
| Test | Rationale |
|---|---|
| Total/free testosterone | Biochemical hyperandrogenism; if >5 nmol/L → exclude tumour |
| DHEAS | Adrenal androgen excess; elevated in adrenal tumour/CAH |
| LH / FSH | LH:FSH ratio ≥2–3 (elevated in ~60–70% of PCOS, but not a diagnostic criterion) |
| Oestradiol | Baseline oestrogenic status |
| Prolactin | Exclude hyperprolactinaemia |
| TSH | Exclude thyroid dysfunction |
| 17-OH Progesterone | Exclude non-classic CAH (drawn in follicular phase) |
| AMH | Elevated in PCOS; now incorporated in 2023 diagnostic criteria |
| Fasting glucose + HbA1c | Screen for diabetes/IGT |
| Oral glucose tolerance test (OGTT) | More sensitive for IGT; recommended in high-risk/obese PCOS |
| Fasting lipid profile | All overweight/obese women at diagnosis (Harrison's 22E) |
Imaging
- Pelvic ultrasound (transvaginal preferred):
- ≥20 antral follicles per ovary (2023 updated threshold)
- OR ovarian volume ≥10 cm³
- "String of pearls" sign: multiple peripheral small follicles 2–9 mm
- Note: USS criteria not applied in adolescents or women on OCP
Management
1. Lifestyle Modification (All patients)
- First-line for all women with PCOS (Harrison's 22E)
- 5–10% weight loss in overweight/obese women:
- Restores ovulation in up to 80%
- ↓ androgens, ↓ insulin resistance, ↓ LH, ↑ SHBG
- Improves metabolic parameters
- Low glycaemic index diet, aerobic + resistance exercise
- Pre-pregnancy counselling and lifestyle optimisation recommended before attempting conception (Harrison's 22E)
2. Menstrual Regulation and Endometrial Protection
Combined Hormonal Contraceptives (CHC) — First-line (not seeking pregnancy)
- Regulate cycles; ↑ SHBG → ↓ free testosterone → treat hirsutism/acne
- Androgen effects improve by 2–3 months; hirsutism improvement takes longer (6–12 months)
- Use lowest effective oestrogen dose, cyclic or continuous
- Progestins alone if CHC contraindicated:
- Medroxyprogesterone acetate 10 mg daily × 10–14 days every 1–3 months
- Micronised progesterone 200 mg daily × 10–14 days every 3 months
- Levonorgestrel IUD (Mirena)
3. Hyperandrogenism (Hirsutism/Acne)
| Drug | Mechanism | Notes |
|---|---|---|
| CHC | ↑ SHBG, ↓ LH → ↓ ovarian androgens | First-line |
| Spironolactone (50–200 mg/day) | Androgen receptor blocker + weak androgen synthesis inhibitor | Add after 6 months inadequate CHC response; teratogenic — use with contraception (Harrison's 22E) |
| Flutamide | Pure androgen receptor antagonist | Hepatotoxicity risk; less commonly used |
| Finasteride | 5α-reductase inhibitor → ↓ DHT | Useful for alopecia; teratogenic |
| Topical eflornithine | Inhibits ornithine decarboxylase → slows hair growth | Facial hirsutism |
| Physical hair removal | Laser, electrolysis | Adjunct to pharmacotherapy |
Metformin is NOT recommended for treating hyperandrogenic symptoms alone (Harrison's 22E)
4. Metabolic Risk Management
| Intervention | Indication | Notes |
|---|---|---|
| Metformin | Overweight/obese PCOS; IGT/T2DM; ↑ cardiometabolic risk | ↓ insulin resistance, ↓ androgens, restores ovulation; not for endometrial protection or hirsutism alone (Harrison's 22E) |
| Statins | Dyslipidaemia | Teratogenic — stop before conception |
| GLP-1 agonists (e.g., semaglutide) | Obesity + PCOS; metabolic syndrome | Emerging role; significant weight loss and insulin sensitisation |
| SGLT2 inhibitors | T2DM + PCOS | Emerging data |
| Antihypertensives | Hypertension | Avoid ACE inhibitors/ARBs if pregnant |
5. Fertility / Ovulation Induction
| Treatment | Notes |
|---|---|
| Letrozole (aromatase inhibitor) | First-line ovulation induction; higher live birth rates than clomiphene; 2.5–7.5 mg on days 3–7 |
| Clomiphene citrate (SERM) | Second-line; 50–150 mg on days 3–7; risk of multiple pregnancy |
| Metformin + clomiphene | Adjunct in obese/insulin-resistant women |
| Gonadotropins (FSH injections) | Step-up low-dose protocol; high risk of OHSS in PCOS — use judiciously (Harrison's 22E) |
| IVF | After failed ovulation induction; freeze-all cycle preferred (↓ OHSS risk) |
| Laparoscopic ovarian drilling (LOD) | Second-line surgical option; thermal/laser puncture of ovarian stroma; restores ovulation in ~50% |
Ovarian hyperstimulation syndrome (OHSS): Major risk in PCOS — prevent with low-dose gonadotropin protocols, GnRH agonist trigger, and freeze-all strategies
6. Screening and Monitoring
- Obesity (BMI, waist circumference)
- Hypertension
- Glycaemic control (fasting glucose/HbA1c ± OGTT)
- Lipid profile (overweight/obese women)
- Depression and anxiety
- Endometrial protection (ensure regular withdrawal bleeds)
Summary — PCOS at a Glance
| Domain | Key Points |
|---|---|
| Prevalence | 6–10% of reproductive-age women; most common endocrine disorder in this group |
| Core triad | Hyperandrogenism + Anovulation + Polycystic ovarian morphology |
| Diagnosis | Rotterdam criteria: 2/3 features after exclusion of other causes; updated 2023 criteria include AMH |
| Pathophysiology | ↑ LH pulsatility → ↑ ovarian androgens; insulin resistance → ↑ free testosterone; follicular arrest |
| Metabolic risk | T2DM, metabolic syndrome, dyslipidaemia, CVD, MASLD, OSA |
| Reproductive risk | Anovulatory infertility, miscarriage, gestational diabetes, pre-eclampsia |
| Long-term cancer risk | Endometrial cancer (2–6×); ovarian cancer risk debated |
| Menstrual Rx | CHC first-line; progestins if CHC contraindicated |
| Hyperandrogen Rx | CHC → add spironolactone after 6 months if insufficient |
| Fertility Rx | Letrozole first-line → clomiphene → gonadotropins → IVF |
| Metabolic Rx | Lifestyle (cornerstone); metformin in overweight/obese; GLP-1 agonists emerging |
| Adolescents | Diagnose on anovulation + hyperandrogenism only; wait 3 years post-menarche |
Home ir testing for insulin resistance
What Is Insulin Resistance?
"A decreased biological response to normal concentrations of circulating insulin." — Tietz Textbook of Laboratory Medicine, 7th Ed.
Gold Standard — Euglycaemic-Hyperinsulinaemic Clamp
- A constant IV insulin infusion is given in one arm
- A variable IV glucose infusion in the other arm maintains blood glucose at normal fasting levels
- The glucose infusion rate (GIR) required to maintain euglycaemia = measure of insulin sensitivity
- Higher GIR = more sensitive; Lower GIR = more resistant
- Performed in hospital under close medical supervision — not remotely approximable at home
- Complex, expensive, and impractical for routine or population use
Clinical Surrogate Measures (Requiring a Lab)
1. HOMA-IR (Homeostatic Model Assessment of Insulin Resistance)
"A simpler but indirect approach — a calculation derived from fasting glucose and insulin concentrations." — Tietz Textbook of Laboratory Medicine, 7th Ed.
| HOMA-IR Value | Interpretation |
|---|---|
| <1.0 | Optimal insulin sensitivity |
| 1.0–1.9 | Early/mild insulin resistance |
| 2.0–2.9 | Moderate insulin resistance |
| ≥3.0 | Significant insulin resistance |
| >2.3 | Clinically indicative of IR (used in PCOS literature — Kaplan & Sadock's) |
- Poor precision
- Insulin assays vary significantly between laboratories (no universal standardisation)
- Does not account for hepatic vs. peripheral IR separately
- Affected by beta-cell dysfunction (low insulin + high glucose can give misleading low HOMA-IR)
2. Fasting Insulin Alone
- Normal fasting insulin: 2–25 μIU/mL (varies by assay; Tietz)
- More specific assays: <10 μIU/mL as upper normal
- Elevated fasting insulin in the presence of normal glucose = hyperinsulinaemia compensating for IR
- Requires a lab — not measurable at home
3. OGTT-Derived Indices
"OGTT-derived insulin sensitivity indices may be preferred to fasting sample-derived indices." — Brenner & Rector's The Kidney
- Matsuda Index (ISI-composite): Calculated from glucose and insulin values during a 75 g OGTT at 0, 30, 60, 90, 120 minutes
- More accurate than HOMA-IR as it reflects both fasting and post-load insulin dynamics
- Requires laboratory measurement at multiple time points — clinic-based only
4. TyG Index (Triglyceride-Glucose Index)
- Validated surrogate for IR — correlates well with clamp studies
- Requires fasting lipid panel + fasting glucose from a lab
- Cutoff: TyG ≥8.5 suggests insulin resistance
- Advantage: Uses routine labs already ordered; no insulin assay needed
5. Metabolic Syndrome Criteria as a Clinical Proxy
| Criterion | Threshold |
|---|---|
| Waist circumference | >88 cm (women), >102 cm (men) |
| Fasting triglycerides | >150 mg/dL (>1.7 mmol/L) |
| HDL cholesterol | <50 mg/dL (women), <40 mg/dL (men) |
| Blood pressure | ≥130/85 mmHg |
| Fasting plasma glucose | ≥100 mg/dL (≥5.6 mmol/L) |
What Can Actually Be Done At Home?
| Self-Assessment | What It Signals |
|---|---|
| Waist circumference (tape measure) | Central adiposity — the strongest clinical correlate of IR |
| BMI calculation | Overall adiposity burden |
| Acanthosis nigricans (visual skin check) | Velvety hyperpigmented skin at neck/axillae — a visible sign of hyperinsulinaemia |
| Blood pressure monitor | Hypertension is a component of metabolic syndrome |
| Home glucose meter (fasting capillary glucose) | Impaired fasting glucose (IFG: 100–125 mg/dL) suggests IR; not a direct IR measure |
| Symptom pattern | Fatigue after carbohydrate meals, abdominal weight gain, cravings, irregular periods (in women) |
A home glucose meter gives capillary blood glucose only — it does not measure insulin and cannot calculate HOMA-IR.
"Home IR Test Kits" — Commercial Products
- A finger-prick blood sample sent by post to a laboratory
- Results returned online
- Often measure: fasting glucose, HbA1c, fasting insulin, and calculate HOMA-IR
- These are mail-order laboratory tests, not truly "home tests" — the measurement still happens in a certified laboratory
- Validity depends entirely on: whether the user was truly fasting, blood sample handling quality, and lab insulin assay standardisation
- HOMA-IR calculated from a mail-order kit is a reasonable surrogate if properly performed, but results should be interpreted by a clinician in clinical context
- Not endorsed by any major clinical guideline as a standalone diagnostic tool
Summary
| Method | Setting | Accuracy | Practical? |
|---|---|---|---|
| Euglycaemic clamp | Hospital (research) | Gold standard | No |
| HOMA-IR | Lab (fasting blood draw) | Good surrogate | Clinic/lab |
| Fasting insulin | Lab | Indirect | Clinic/lab |
| TyG index | Lab (routine labs) | Good surrogate | Clinic/lab |
| OGTT indices | Clinic | Better than HOMA | Clinic only |
| Mail-order IR kit | Home sample → lab | Reasonable if done correctly | Partial |
| Fasting home glucose | Home glucometer | Glucose only — not IR | Limited proxy |
| Waist circumference + symptoms | Home | Clinical proxy only | Screening only |
Homa ir formula
Interpretation
| HOMA-IR | Meaning |
|---|---|
| <1.0 | Optimal insulin sensitivity |
| 1.0–1.9 | Mild insulin resistance |
| 2.0–2.9 | Moderate insulin resistance |
| ≥3.0 | Significant insulin resistance |
| >2.3 | Commonly used clinical cutoff for IR (especially in PCOS) |
Example Calculation
- Fasting insulin = 12 μIU/mL
- Fasting glucose = 5.5 mmol/L
- HOMA-IR = (12 × 5.5) / 22.5 = 2.93 → moderate insulin resistance
Requirements
- Both values must be drawn after 8–12 hours of overnight fasting
- Venous blood sample only — home glucometer readings are not accurate enough for this calculation
In mg/dl example
Example
- Fasting insulin = 12 μIU/mL
- Fasting glucose = 99 mg/dL
Quick Reference — Common Glucose Values
| Fasting Glucose (mg/dL) | Fasting Insulin (μIU/mL) | HOMA-IR | Interpretation |
|---|---|---|---|
| 85 | 5 | 1.05 | Normal |
| 90 | 10 | 2.22 | Borderline |
| 99 | 12 | 2.93 | Moderate IR |
| 105 | 15 | 3.89 | Significant IR |
| 110 | 18 | 4.89 | Significant IR |
| 126 | 20 | 6.22 | Severe IR / T2DM range |
Difference between type 1 and type 2 criggler najar
Crigler-Najjar Syndrome: Type I vs Type II
Side-by-Side Comparison
| Feature | Type I | Type II (Arias Syndrome) |
|---|---|---|
| Enzyme activity | Absent (0%) — complete deficiency | Markedly reduced but detectable (<10% of normal) |
| UGT1A1 mutations | 59+ mutations; all encode proteins with no functional activity; common exons 2–5 (Type 1A) or bilirubin-specific exon A1 (Type 1B) | 48+ mutations; all encode proteins with residual activity |
| Serum bilirubin | Extremely high — typically 20–45 mg/dL | Moderately elevated — typically 6–25 mg/dL |
| Onset | Neonatal — striking jaundice from birth | Neonatal or early childhood; often less dramatic |
| Bilirubin in bile | Absent conjugated bilirubin in bile | Small amounts of conjugated bilirubin present |
| Kernicterus risk | Very high — major cause of death without treatment | Lower but real — can occur with fasting, illness, or stress that raises bilirubin acutely |
| Response to phenobarbital | None — unresponsive | Yes — bilirubin falls to 3–5 mg/dL; single bedtime dose often sufficient |
| Prognosis without treatment | Death from bilirubin encephalopathy in infancy or early childhood | Generally survive; chronic low-grade risk of neurological damage |
| Treatment | Phototherapy 12h/day + early liver transplantation (curative); plasmapheresis for acute crises; oral calcium phosphate to interrupt enterohepatic circulation | Phenobarbital (induces residual UGT1A1 expression via CAR receptor); phototherapy if needed |
| Definitive cure | Liver transplantation (before brain damage occurs) | Usually not needed; phenobarbital sufficient |
Pathophysiology Summary
UGT1A1 mutation
↓
Type I: Zero enzyme → bilirubin accumulates → crosses BBB → kernicterus
Type II: <10% enzyme → bilirubin elevated but lower → kernicterus only under stress
Why Phenobarbital Works in Type II but Not Type I
- Phenobarbital is an inducer of the constitutive androstane receptor (CAR) → upregulates UGT1A1 gene expression
- In Type II: residual enzyme exists → phenobarbital amplifies it → bilirubin falls to safe levels (2–5 mg/dL)
- In Type I: no functional enzyme present at all → nothing to induce → no response
Spectrum of UGT1A1 Disorders
| Condition | UGT1A1 Activity | Bilirubin (mg/dL) | Kernicterus Risk |
|---|---|---|---|
| Crigler-Najjar Type I | 0% | 20–45 | Very high |
| Crigler-Najjar Type II | <10% | 6–25 | Low (stress-related) |
| Gilbert Syndrome | 10–33% | <4 (usually <3) | None |
Gilbert syndrome = same enzyme, same pathway, but only a promoter mutation (UGT1A1*28) causing reduced transcription — clinically benign.
Key Mnemonics
- Type I = Incompatible with life without treatment; Inducer (phenobarbital) doesn't work; needs Immediate liver transplant
- Type II = Treatable with Tablet (phenobarbital); Tolerable bilirubin levels
Asymptomatic hyperbilirubinemia
Asymptomatic Hyperbilirubinaemia
Definition
"Differentiating between these syndromes is possible but clinically unnecessary due to their benign nature." — Harrison's 22E, p. (Ch. 52)
Classification by Bilirubin Type
| Type | Also Called | Mechanism | Key Causes |
|---|---|---|---|
| Unconjugated (indirect) | Indirect | Defect in uptake or conjugation | Gilbert's, Crigler-Najjar, haemolysis, drugs |
| Conjugated (direct) | Direct | Defect in canalicular transport or reuptake | Dubin-Johnson, Rotor syndrome |
| Mixed | Both fractions elevated | Combined defect | Rotor syndrome, early liver disease |
Causes of Asymptomatic Unconjugated Hyperbilirubinaemia
1. Gilbert's Syndrome ⭐ Most Common
- Prevalence: 3–12% of the population; M:F ratio 1.5–7:1
- Defect: UGT1A1*28 promoter polymorphism → ↓ transcription of UGT1A1 → reduced bilirubin conjugation to 10–33% of normal
- Asian populations: coding region mutations more common than *28 allele
- Bilirubin: Typically <3 mg/dL (always <6 mg/dL); almost entirely unconjugated
- Triggers that raise bilirubin (2–3× baseline):
- Fasting / dehydration
- Intercurrent illness, stress
- Physical exertion
- Alcohol
- Sleep deprivation, menstruation
- Diagnosis: Clinical — young patient, mild isolated unconjugated hyperbilirubinaemia, normal LFTs, no haemolysis
- Liver biopsy: Not required
- Prognosis: Entirely benign — no treatment needed; reassure the patient
⚠️ Critical Drug Interaction in Gilbert's
| Drug | Risk |
|---|---|
| Irinotecan (CPT-11) | Active metabolite SN-38 glucuronidated by UGT1A1 → impaired clearance → severe diarrhoea, myelosuppression |
| Raloxifene | 2× higher drug exposure due to impaired glucuronidation |
| Atazanavir / Indinavir (HIV protease inhibitors) | Competitively inhibit UGT1A1 → worsen hyperbilirubinaemia; higher risk in Gilbert's |
2. Crigler-Najjar Syndrome Type II (Arias Syndrome)
- UGT1A1 activity: <10% of normal
- Bilirubin: 6–25 mg/dL — unconjugated; may be mildly symptomatic (chronic jaundice)
- Not truly asymptomatic — discussed for completeness
- Responds to phenobarbital (reduces bilirubin to 3–5 mg/dL)
- Kernicterus risk under stress
3. Drug-Induced Unconjugated Hyperbilirubinaemia
| Drug | Mechanism |
|---|---|
| Rifampin | Inhibits hepatic bilirubin uptake (competes with bilirubin at sinusoidal membrane) |
| Probenecid | Inhibits hepatic bilirubin uptake |
| HIV protease inhibitors (atazanavir, indinavir) | Inhibit UGT1A1 conjugation → unconjugated hyperbilirubinaemia in >25% of patients |
4. Haemolysis (Subclinical)
- Mild haemolysis → ↑ bilirubin production overwhelms conjugation capacity
- Always exclude before diagnosing Gilbert's:
- Full blood count (anaemia?)
- Reticulocyte count (↑ in haemolysis)
- LDH (↑), haptoglobin (↓)
- Blood film (spherocytes, elliptocytes, etc.)
- Note: >50% of Gilbert's patients have mild haemolysis as a co-contributor (Goldman-Cecil)
Causes of Asymptomatic Conjugated Hyperbilirubinaemia
5. Dubin-Johnson Syndrome
- Defect: Mutations in ABCC2 gene → absent/defective MRP2 (Multidrug Resistance Protein 2) on canalicular membrane → impaired secretion of conjugated bilirubin into bile
- Bilirubin: 2–5 mg/dL; ~60% conjugated (direct reacting); occasionally up to 20 mg/dL
- All other LFTs: Normal
- Inheritance: Autosomal recessive
- Clinical: Asymptomatic jaundice; may worsen with pregnancy, OCP use, or intercurrent illness
- Liver biopsy: Black/dark brown pigment in hepatocytes (lipofuscin-like melanin pigment — grossly black liver)
- Urine coproporphyrin pattern: Total coproporphyrin normal; but coproporphyrin I = 80% of total (normally coproporphyrin III = 75%)
- Prognosis: Benign — no treatment, no progression
6. Rotor Syndrome
- Defect: Mutations in SLCO1B1 and SLCO1B3 → loss of OATP1B1 and OATP1B3 (hepatic sinusoidal reuptake transporters) → bilirubin conjugates cannot be reabsorbed from sinusoidal blood → spill into systemic circulation
- Bilirubin: 3–7 mg/dL; ~60% conjugated; occasionally higher
- All other LFTs: Normal
- Inheritance: Autosomal recessive
- Liver biopsy: Normal (no pigment — contrast to Dubin-Johnson)
- Urine coproporphyrin pattern: Total coproporphyrin elevated 2–5×; normal I:III ratio
- Prognosis: Benign — no treatment required
Comparison Table — All Hereditary Asymptomatic Hyperbilirubinaemias
| Feature | Gilbert's | Crigler-Najjar II | Dubin-Johnson | Rotor |
|---|---|---|---|---|
| Bilirubin type | Unconjugated | Unconjugated | Conjugated/mixed | Conjugated/mixed |
| Serum bilirubin | <4 mg/dL | 6–25 mg/dL | 2–5 mg/dL | 3–7 mg/dL |
| UGT1A1 activity | 10–33% | <10% | Normal | Normal |
| Defective gene | UGT1A1 (promoter) | UGT1A1 (coding) | ABCC2 (MRP2) | SLCO1B1 + SLCO1B3 |
| Mechanism | ↓ Conjugation | ↓ Conjugation | ↓ Canalicular secretion | ↓ Hepatic reuptake of conjugates |
| Other LFTs | Normal | Normal | Normal | Normal |
| Liver biopsy | Normal | Normal | Black pigment | Normal |
| Urine coproporphyrin | Normal | Normal | Normal total; ↑ Copro I (80%) | ↑ Total (2–5×) |
| Response to phenobarbital | Normalises bilirubin | ↓ Bilirubin | No effect | No effect |
| Triggers | Fasting, illness, alcohol | Illness, surgery | OCP, pregnancy | — |
| Kernicterus risk | None | Low (under stress) | None | None |
| Prevalence | 3–12% of population | Rare | Rare | Rare |
| Prognosis | Benign | Generally benign | Benign | Benign |
| Treatment | None — reassure | Phenobarbital | None | None |
Diagnostic Approach to Isolated Hyperbilirubinaemia
Isolated elevated bilirubin (normal ALT, AST, ALP, GGT)
↓
Fractionate bilirubin
↙ ↘
Unconjugated Conjugated/Mixed
↓ ↓
Check reticulocytes, → Dubin-Johnson
LDH, haptoglobin, or Rotor syndrome
blood film (urine coproporphyrin
↓ pattern differentiates)
Haemolysis excluded?
↓
Young patient, mild
bilirubin <4 mg/dL
↓
→ Gilbert's Syndrome
(no further workup
unless drug concern)
Key Teaching Points
- Gilbert's syndrome is the most common cause — affects up to 12% of the population; entirely benign but important for drug dosing (irinotecan toxicity)
- All four hereditary asymptomatic syndromes have normal aminotransferases and ALP — any elevation shifts the diagnosis toward liver disease
- Dubin-Johnson vs Rotor: Distinguished by liver biopsy (pigment vs. normal) and urine coproporphyrin pattern — but clinically unnecessary as both are benign (Harrison's 22E)
- Rifampin/probenecid can mimic Gilbert's by blocking hepatic bilirubin uptake — always take a drug history
- Haemolysis must always be excluded before attributing unconjugated hyperbilirubinaemia to Gilbert's
Case of aortic stenosis full viva based starting from history, hopi, present history past history, general examination cvs examination, provisional diagnosis in Indian medical College viva style
Aortic Stenosis — Complete Indian Medical College Viva
History → Examination → Provisional Diagnosis
🎓 VIVA OPENING — Examiner Sets the Scene
"You are posted in Medicine/Cardiology ward. A 55-year-old male farmer from rural Maharashtra has been admitted with complaints of breathlessness and chest pain on exertion for the past 6 months. Take a complete history and examine this patient."
PART I — HISTORY TAKING
1. Biodata
| Name | Mr. Ramesh S. |
| Age | 55 years |
| Sex | Male |
| Occupation | Farmer |
| Residence | Rural Maharashtra |
| Religion | Hindu |
| Marital status | Married |
| Date of admission | (today's date) |
| Informant | Patient himself (reliable) |
2. Chief Complaints (CC)
- Breathlessness on exertion — 6 months
- Chest pain/discomfort on exertion — 4 months
- Two episodes of blackouts (syncope) — 2 months
- Swelling of feet — 3 weeks
Examiner Q: Why do you list them in this order? Answer: Symptoms are listed in chronological order of onset. This reveals the natural progression of AS: dyspnoea → angina → syncope, followed by features of decompensation (oedema).
3. History of Present Illness (HOPI)
Breathlessness
- Onset: Insidious, 6 months ago
- Initially on heavy exertion (ploughing fields) — NYHA Class II
- Progression: Now on mild exertion (walking 50–100 metres on flat ground) — NYHA Class III
- Orthopnoea: Patient now sleeps with 2 pillows (developed 2 months ago)
- PND: Present — patient wakes from sleep 1–2 hours after lying down, sits up or stands by window for relief
- No wheeze (distinguishes from asthma)
- Aggravating factors: Exertion, lying flat
- Relieving factors: Rest, sitting upright
Chest Pain
- Onset: 4 months ago
- Character: Tight, constricting, substernal
- Radiation: To the left shoulder and jaw
- Duration: 5–10 minutes per episode
- Precipitating factor: Exertion only (climbs stairs, walks fast)
- Relieving factor: Rest within minutes
- No rest pain, no nocturnal pain
- No palpitations preceding chest pain
- NYHA/CCS Class II angina
Examiner Q: What is the triad of symptoms in aortic stenosis? Answer: SAD — Syncope, Angina, Dyspnoea. The onset of any one of these symptoms dramatically worsens prognosis:
- Angina → mean survival ~5 years
- Syncope → mean survival ~3 years
- Heart failure (dyspnoea) → mean survival ~1–2 years
Syncope
- 2 episodes in last 2 months
- Both precipitated by exertion (getting up from squat after work)
- Sudden loss of consciousness — no preceding aura, no tongue bite, no urinary incontinence, no post-ictal confusion
- Duration: 30–60 seconds each time
- Spontaneous recovery — no residual neurological deficit
- Witnessed by family — described as "gone white, fell gently, came back quickly"
- No palpitations preceding — not arrhythmic syncope
- No head injury
Examiner Q: Why does syncope occur in aortic stenosis? Answer: During exertion, cardiac output cannot increase due to the fixed obstruction. Peripheral vasodilation in exercising muscles occurs normally, but the heart cannot compensate → ↓ cerebral perfusion → syncope. Also, effort may trigger baroreceptor-mediated reflex vasodilation (vasovagal mechanism). Rarely, exertion-induced arrhythmia may contribute.
Pedal Oedema
- Onset: 3 weeks ago — bilateral, pitting
- Started at ankles, now up to mid-shin
- Worse in the evenings, better in the mornings
- Associated with decreased urine output over same period
- No ascites, no facial puffiness
4. Past History
| System | Details |
|---|---|
| Rheumatic fever | History of recurrent sore throats and joint pains in childhood (age 10–14 years) — treated with penicillin injections for 2–3 years — stopped at age 18 |
| Cardiac history | Told "heart murmur present" at age 25 during army medical examination — not investigated further |
| Hypertension | Not known hypertensive |
| Diabetes mellitus | Not a known diabetic |
| Tuberculosis | No history of TB, no anti-TB treatment |
| Surgery | No previous surgeries |
| Hospitalisation | No prior admissions |
| Asthma/COPD | No history of wheeze or chronic cough |
Examiner Q: Why is the childhood history relevant here? Answer: Rheumatic fever is the most common cause of aortic stenosis in India (unlike the West where calcific/degenerative AS predominates in elderly). The childhood history of recurrent streptococcal pharyngitis, joint pains, and penicillin prophylaxis strongly suggests rheumatic aortic stenosis. The murmur detected at age 25 is consistent with the known long latency (20–30 years) of rheumatic valvular disease before symptoms develop.
5. Family History
- No family history of heart disease, sudden cardiac death, or valve disease
- No family history of diabetes, hypertension, dyslipidaemia
6. Personal History
| Diet | Non-vegetarian, adequate |
| Appetite | Reduced over past 3 months |
| Bowel habits | Regular |
| Micturition | Decreased frequency — nocturia once |
| Sleep | Disturbed — orthopnoea and PND |
| Addiction | Bidi smoking — 20 pack-years; occasional alcohol (no dependence) |
| Allergies | None known |
| Occupation | Farmer — heavy manual labour, now significantly limited |
7. Socioeconomic History
- Lives in kutcha house with 6 family members
- Income from farming — lower socioeconomic class
- No insurance coverage
- Travelled 120 km to reach tertiary hospital
PART II — GENERAL EXAMINATION
"Sir, on general examination, the patient is:"
Build and Appearance
- Middle-aged male, moderately built, moderately nourished
- Conscious, cooperative, oriented to time, place, and person
- Not in acute distress at rest; becomes breathless on minimal exertion
Vital Signs
| Parameter | Finding | Significance |
|---|---|---|
| Pulse | 76 bpm, regular, low volume, slow rising, anacrotic character, all peripheral pulses felt | Pulsus parvus et tardus — pathognomonic of severe AS |
| Blood pressure | 100/80 mmHg — narrow pulse pressure (20 mmHg) | ↓ stroke volume; normal pulse pressure 40–60 mmHg |
| Respiratory rate | 22/min | Tachypnoea — early pulmonary congestion |
| Temperature | 98.6°F — afebrile | |
| SpO₂ | 94% on room air | Mild hypoxaemia |
Examiner Q: What is pulsus parvus et tardus? Why does it occur? Answer:
- Parvus = small/low volume pulse
- Tardus = slow-rising, delayed upstroke
- Occurs because the stenotic aortic valve causes fixed obstruction to LV outflow → ↓ stroke volume → small pulse volume; the valve opening is slow and incomplete → delayed peak → anacrotic shoulder on upstroke
- Best felt at the carotid artery (Goldman-Cecil, p. 698)
Pallor, Icterus, Cyanosis, Clubbing, Oedema, Lymphadenopathy (PICCLE)
| Sign | Finding |
|---|---|
| Pallor | Mild — mucous membranes slightly pale (mild anaemia from chronic disease) |
| Icterus | Absent |
| Cyanosis | Absent peripherally and centrally at rest |
| Clubbing | Absent (clubbing not a feature of AS) |
| Lymphadenopathy | Absent |
| Oedema | Pitting pedal oedema — bilateral, 2+ up to mid-shin; pits easily, does not transilluminate |
Jugular Venous Pressure (JVP)
- Elevated — 5 cm above sternal angle (normal <4 cm at 45°)
- Waveform: Prominent a wave (↑ right heart filling pressure from right heart involvement and pulmonary hypertension; also vigorous atrial contraction against stiff RV)
- No Kussmaul's sign
Examiner Q: Is JVP typically elevated in pure aortic stenosis? Answer: In early/compensated AS, JVP is normal — AS is primarily a left heart disease. Elevated JVP indicates decompensation with pulmonary hypertension → RV pressure overload → RV failure. This patient has elevated JVP because he has advanced disease with cardiac decompensation.
PART III — CARDIOVASCULAR SYSTEM EXAMINATION
Inspection
| Area | Finding |
|---|---|
| Precordium | No visible pulsations; no deformity, no scars |
| Apex beat | Visible in 5th intercostal space, medial to midclavicular line (not displaced laterally — important in AS) |
| Carotid pulsations | Visible but diminished in amplitude |
| Neck veins | Distended as noted |
Palpation
| Finding | Description | Significance |
|---|---|---|
| Apex beat | 5th ICS, medial to MCL — not displaced | LV hypertrophy without dilatation (pressure overload → concentric hypertrophy) |
| Character of apex | Heaving (sustained, forceful) — "tapping" quality; palpable S4 | Sustained apex = pressure overload hypertrophy |
| Systolic thrill | Palpable thrill at aortic area (right 2nd ICS) AND at the suprasternal notch and carotids | Thrill = grade 4+ murmur; indicates severe AS |
| Parasternal heave | Present (if pulmonary hypertension → RV enlargement) | Suggests RV involvement from elevated PCWP |
| No tapping apex | — | Distinguishes from mitral stenosis |
Examiner Q: What does "heaving apex" tell you? Answer: A heaving (sustained, thrusting) apex beat indicates pressure overload of the left ventricle — the hallmark of AS. The LV works against the obstruction, develops concentric hypertrophy, and therefore the apex does not displace outward (unlike volume overload in AR/MR where the apex is displaced and diffuse).
Examiner Q: The simultaneous finding of what two signs at the bedside strongly suggests severe AS? Answer: (Goldman-Cecil, p. 698): Forceful LV apex beat + delayed and weakened carotid pulse felt simultaneously = highly persuasive of severe AS.
Percussion
- Cardiac dullness: Within normal limits in transverse diameter (no significant cardiomegaly — concentric hypertrophy without dilatation in compensated phase)
- If decompensated: Slight increase in transverse cardiac dullness
Auscultation ⭐ Most Important Section
| Area | Heart Sounds | Significance |
|---|---|---|
| S1 | Normal or slightly soft | |
| Systolic ejection click | Present only if valve is still mobile (non-calcified — congenital bicuspid AS in young) | Absent in calcified rheumatic/degenerative AS |
| S2 | Single — aortic component (A2) absent or very soft | Calcified valve cannot close briskly → ↓ A2; P2 may be prominent if pulmonary hypertension |
| Paradoxical splitting of S2 | P2 before A2 (split widens on expiration) | Delayed LV emptying → delayed A2 → A2 occurs after P2 |
| S4 (atrial gallop) | Present at apex | Stiff, hypertrophied LV requires forceful atrial contraction; in SR — if AF develops, S4 disappears |
| S3 | May appear in decompensated/dilated phase | Indicates ↓ EF, advanced disease |
The Murmur — Detailed Description
"Sir, I auscultate a murmur with the following characteristics:"
| Feature | Finding |
|---|---|
| Timing | Systolic |
| Type | Ejection (crescendo-decrescendo) — begins after S1, ends before S2 |
| Grade | Grade 4/6 (with thrill) |
| Quality | Harsh, rough, rasping ("machinery-like") |
| Pitch | Medium-high |
| Site of maximum intensity | Aortic area — right 2nd intercostal space, right sternal border |
| Radiation | To bilateral carotids (by direct transmission of blood jet); to suprasternal notch |
| Shape | Late peaking (peak in midsystole to late systole in severe AS) |
| Effect of respiration | Does not increase with inspiration (left-sided murmur) |
| Effect of Valsalva | Decreases (↓ venous return → ↓ gradient) — distinguishes from HOCM (HOCM murmur increases with Valsalva) |
| Effect of squatting | Increases (↑ venous return) |
| Gallavardin phenomenon | Musical high-pitched component heard at the apex that may mimic mitral regurgitation — actually the high-frequency component of AS murmur transmitted to apex |
Examiner Q: How do you differentiate the murmur of AS from the murmur of HOCM (HCM)?
| Feature | Aortic Stenosis | HOCM |
|---|---|---|
| Site max | Right 2nd ICS | 3rd–4th ICS left sternal border |
| Carotid radiation | Yes | No |
| Carotid pulse | Parvus et tardus | Brisk, bisferious |
| Valsalva | Murmur ↓ | Murmur ↑ |
| Squatting | Murmur ↑ | Murmur ↓ |
| Thrill | Aortic area | Left sternal border |
Additional Auscultatory Areas
- Mitral area: Check for mitral regurgitation (frequently coexists in rheumatic disease); also assess for Gallavardin phenomenon
- Pulmonary area: Loud P2 if pulmonary hypertension present
- Tricuspid area: Pansystolic murmur if functional TR from RV dilatation
- Lung bases: Bilateral fine crepitations — pulmonary congestion
Peripheral Vascular Examination
- Carotid pulse: Low volume, slow-rising, anacrotic character bilaterally
- Femoral pulse: Present, may be diminished
- All peripheral pulses palpable
- No signs of peripheral embolism
PART IV — OTHER SYSTEM EXAMINATION
Respiratory System
- Bilateral fine basal crepitations (not clearing with cough) — pulmonary venous congestion
- No wheeze (rules out asthma)
- Percussion note: Dull at bases bilaterally (early pleural effusion from elevated PCWP)
Abdomen
- Liver: Palpable 3 cm below right costal margin — tender, smooth, soft — congestive hepatomegaly (from elevated JVP/RHF)
- Spleen: Not palpable
- Ascites: Not present (absent fluid thrill and shifting dullness)
- No ankle-to-groin pitting
Central Nervous System
- No focal neurological deficits
- MMSE: Normal — no embolic events
PART V — PROVISIONAL DIAGNOSIS
"Sir, based on the history and clinical examination, my provisional diagnosis is:"
Primary Diagnosis
Severe Rheumatic Aortic Stenosis with Decompensated Heart Failure (NYHA Class III)
| Symptom/Sign | Clinical Significance |
|---|---|
| Childhood rheumatic fever history | Aetiological basis — rheumatic AS |
| Murmur detected at age 25 | Long latent period before symptoms — consistent with valvular AS |
| Classic SAD triad — dyspnoea, angina, syncope on exertion | Cardinal symptoms of AS |
| Pulsus parvus et tardus | Reduced stroke volume, fixed obstruction |
| Narrow pulse pressure (20 mmHg) | ↓ Stroke volume |
| Heaving (sustained) apex at 5th ICS, not displaced | Concentric LVH — pressure overload |
| Palpable systolic thrill at right 2nd ICS and carotids | Grade ≥4 murmur; severe AS |
| Harsh late-peaking crescendo-decrescendo systolic murmur at right 2nd ICS radiating to carotids | Classic AS murmur |
| Single S2 (absent A2) | Calcified, immobile aortic valve |
| Paradoxical splitting of S2 | Delayed LV emptying |
| S4 gallop | Stiff, hypertrophied LV |
| Bilateral basal crepitations | Pulmonary oedema/venous congestion |
| Elevated JVP with prominent a wave | Decompensation, pulmonary hypertension |
| Pitting pedal oedema | Right heart failure — decompensation |
| Congestive hepatomegaly | Right heart failure |
Differential Diagnoses
| Diagnosis | For | Against |
|---|---|---|
| Hypertrophic obstructive cardiomyopathy (HOCM) | Systolic murmur, LVH, syncope | Murmur decreases with Valsalva (not increases); carotid pulse brisk not parvus; no rheumatic history; murmur at LLSB not aortic area |
| Mitral regurgitation | Systolic murmur | Murmur pansystolic, best at apex, radiates to axilla; normal S2; hyperdynamic displaced apex |
| Aortic sclerosis | Systolic murmur at aortic area, elderly | Soft, early peaking murmur; NO carotid radiation; normal carotid pulse; normal S2; no symptoms |
| Pulmonary stenosis | Systolic ejection murmur | Murmur at left 2nd ICS; increases with inspiration; RV heave; no carotid radiation |
| Ventricular septal defect | Systolic murmur | Pansystolic; left sternal border; thrill at 4th ICS; no radiation to carotids |
Aetiology in This Case
| Cause | Likelihood |
|---|---|
| Rheumatic | Most likely — childhood RF, India, age 55 |
| Calcific degenerative | Possible in elderly (age >65 typically); less likely here |
| Congenital bicuspid | Typically presents earlier (age 40–50); no systolic click here (calcified) |
| Unicuspid | Extremely rare |
Investigations to Order
Bedside / Emergency
- 12-lead ECG: LVH (Sokolow-Lyon criteria), strain pattern (ST depression + T inversion in V4–V6 and I, aVL), LA enlargement (broad notched P in II), LBBB if severe
Imaging
-
CXR PA view:
- Cardiac size — normal to mildly enlarged (concentric hypertrophy — cardiomegaly late)
- Post-stenotic aortic dilatation (dilated ascending aorta)
- Aortic valve calcification (lateral view)
- Pulmonary venous congestion — Kerley B lines, upper lobe diversion, haziness at hila
- Pleural effusion (bilateral)
-
2D Echo + Doppler — Gold Standard:
- Thickened, calcified, restricted aortic valve leaflets
- Assess aortic valve area (AVA):
- Mild AS: AVA >1.5 cm² / mean gradient <20 mmHg
- Moderate AS: AVA 1.0–1.5 cm² / mean gradient 20–40 mmHg
- Severe AS: AVA <1.0 cm² / mean gradient >40 mmHg / peak velocity >4 m/s
- Concentric LVH, ↓ or preserved EF
- Assess co-existing mitral valve disease (rheumatic)
- Pulmonary artery pressure assessment
Laboratory
- FBC (anaemia), RFTs, LFTs (congestive), electrolytes
- Fasting glucose, lipids, TFTs
- BNP/NT-proBNP (elevated — marker of severity and decompensation)
- ESR, CRP, ASO titre (rheumatic activity)
- Blood cultures × 3 if any fever (infective endocarditis risk)
- Urine R/M
Cardiac Catheterisation
- If echo inconclusive, or prior to surgery
- Coronary angiography mandatory before aortic valve replacement (AVR) to assess for concomitant CAD
Management Outline
Immediate (Decompensation)
- Diuretics: Furosemide IV — cautiously (preload-dependent; over-diuresis → ↓ CO)
- Oxygen supplementation
- Fluid restriction: 1.5 L/day
- Salt restriction: <2 g/day
- Vasodilators: Use with extreme caution in severe AS (can cause catastrophic hypotension)
- Digoxin: Only if AF with rapid ventricular rate
- Anticoagulation: Only if AF or mechanical prosthesis
Definitive Treatment — Aortic Valve Replacement (AVR)
"Sir, the definitive treatment is aortic valve replacement. This patient has developed symptoms — he has all three cardinal symptoms of severe AS (SAD triad). AVR is indicated."
| Procedure | When |
|---|---|
| Surgical AVR (SAVR) | Younger patients (<75), low surgical risk — preferred for rheumatic AS |
| TAVR (Transcatheter AVR) | High/prohibitive surgical risk, elderly, or prior chest surgery |
Secondary Prophylaxis
- Benzathine penicillin 1.2 MU IM monthly — lifelong secondary prophylaxis for rheumatic fever (to prevent further valve damage)
Endocarditis Prophylaxis
- Antibiotic prophylaxis before dental/invasive procedures — per current guidelines
Viva Summary — "One-Liner" for Final Answer
"This is a case of a 55-year-old male farmer with a history of childhood rheumatic fever, presenting with the classic triad of aortic stenosis — exertional dyspnoea (NYHA III), exertional angina (CCS II), and exertional syncope — with pulsus parvus et tardus, narrow pulse pressure, heaving non-displaced apex, palpable aortic thrill, harsh late-peaking crescendo-decrescendo systolic murmur at the right second intercostal space radiating to the carotids, single S2, palpable S4, and features of decompensation — elevated JVP, bilateral basal crepitations, congestive hepatomegaly, and pitting pedal oedema — consistent with a diagnosis of severe rheumatic aortic stenosis with decompensated congestive heart failure. Echocardiography is the investigation of choice, and the definitive treatment is aortic valve replacement."
Give Hopi for chief complaint of fatigue and palpitations
HOPI — Chief Complaints: Fatigue and Palpitations
Indian Medical College Viva Style
Chief Complaints
- Fatigue / Easy fatigability — 4 months
- Palpitations — 2 months
HISTORY OF PRESENT ILLNESS
1. FATIGUE / EASY FATIGABILITY
Onset and Duration
- Onset: Insidious, 4 months ago
- Duration: Persistent, progressively worsening
- Prior health: Previously active, no similar complaints
Character and Severity
- Describe as feeling "tired all the time," "weak," "no energy"
- Inability to perform daily routine activities — previously could work full day, now tires after 30 minutes of mild activity
- Functional limitation: Unable to complete household chores / occupational duties
- Not relieved by rest (if so, suspect anaemia, hypothyroidism, cardiac cause)
- OR partially relieved by rest (if so, suspect cardiac/pulmonary cause)
Associated Symptoms — Ask Systematically
With Fatigue — Ask About:
| Question | If Positive | Suggests |
|---|---|---|
| Breathlessness on exertion? | NYHA grading | Cardiac failure, anaemia, ILD |
| Orthopnoea / PND? | Number of pillows | Cardiac failure |
| Chest pain/discomfort? | Character, radiation | ACS, angina |
| Pedal oedema? | Duration, pitting | Cardiac failure, CKD, hypothyroidism |
| Pallor noticed by family? | Yes/No | Anaemia |
| Yellowish discolouration? | Yes/No | Haemolytic anaemia, liver disease |
| Bleeding from any site? | Menorrhagia, haematuria, melaena, haemoptysis | Iron deficiency anaemia, haematological malignancy |
| Weight loss? | Kg over how many months | Malignancy, TB, hyperthyroidism |
| Weight gain? | Recent, with puffiness | Hypothyroidism, nephrotic, cardiac failure |
| Heat / cold intolerance? | Hot = hyperthyroid; Cold = hypothyroid | Thyroid disease |
| Hair loss, dry skin, constipation, hoarse voice? | Yes | Hypothyroidism |
| Excessive sweating, tremors, diarrhoea? | Yes | Hyperthyroidism |
| Fever, night sweats? | Duration, pattern | TB, lymphoma, infective endocarditis |
| Appetite? | Increased (hyperthyroid, diabetes) or decreased (malignancy, hypothyroid) | Various |
| Polyuria, polydipsia, polyphagia? | Yes | Diabetes mellitus |
| Muscle weakness, proximal > distal? | Difficulty rising from squat, combing hair | Myopathy, hyperthyroidism, Cushing's |
| Mood, sleep, concentration, interest in activities? | Low mood, early morning awakening | Depression (most common underdiagnosed cause of fatigue) |
| Menstrual history (in females) | Irregular, heavy, prolonged | Iron deficiency, hypothyroidism, PCOS |
2. PALPITATIONS
Definition Clarify First
"Sir, I first confirmed with the patient what he means by palpitations — an awareness or perception of his own heartbeat, which he finds uncomfortable or abnormal."
Onset and Duration
- Onset: 2 months ago (after fatigue began by 2 months — note temporal relationship)
- Duration: Episodic OR continuous
- Frequency: How many episodes per day/week?
Character — Most Important Part
| Question | Response | Suggests |
|---|---|---|
| Regular or irregular? | Regular | SVT, sinus tachycardia, atrial flutter with fixed block |
| Irregular | AF, frequent ectopics | |
| Regularly irregular | 2nd degree AV block, trigeminy | |
| Irregularly irregular | AF (most common), multifocal atrial tachycardia | |
| Rate? | Fast (>100) | Tachyarrhythmia, sinus tachy |
| Slow (<60) | Bradyarrhythmia, complete heart block | |
| Normal rate | Ectopics ("missed beat" or "extra beat") | |
| Onset | Sudden / instantaneous | Re-entrant SVT, AF |
| Gradual build-up | Sinus tachycardia (anxiety, anaemia, exercise) | |
| Offset | Sudden / instantaneous | Re-entrant SVT |
| Gradual slowing | Sinus tachycardia | |
| "Missed beat" or "flip-flop" | Single thuds | PACs or PVCs (benign ectopics) |
Duration of Each Episode
- Seconds: Ectopics (PAC/PVC) — most common, usually benign
- Minutes: SVT, paroxysmal AF
- Hours: Persistent AF, atrial flutter
- Constant: Persistent AF, sinus tachycardia
Precipitating Factors
| Factor | Suggests |
|---|---|
| Exertion | VT (serious), SVT, sinus tachycardia |
| Caffeine, tea, alcohol | Ectopics, AF |
| Stress, anxiety | Sinus tachycardia, SVT |
| Change in posture | POTS (postural tachycardia syndrome) |
| At rest / nocturnal | Bradyarrhythmia, ectopics, vagally-mediated |
| After meals | Ectopics, vagal |
| No trigger | Paroxysmal AF, re-entrant SVT |
Termination
- Spontaneous? How long to stop?
- Manoeuvres: Valsalva, carotid massage, breath-holding, cold water on face, squatting → if terminates SVT (AV node re-entry), suggests re-entrant mechanism
- Medical cardioversion needed? (suggests sustained AF/flutter/VT)
Associated Symptoms During Palpitation Episode — CRITICAL
| Symptom | Significance |
|---|---|
| Pre-syncope / Lightheadedness | ↓ Cardiac output during arrhythmia; haemodynamically significant |
| Syncope / Loss of consciousness | Red flag — VT, complete heart block, SVT with haemodynamic compromise |
| Chest pain / tightness | Ischaemia triggered by arrhythmia; angina |
| Breathlessness | ↓ Cardiac output; pulmonary oedema (flash) |
| Neck pounding / throbbing | AV dissociation (VT, complete heart block) — atria contracting against closed AV valve |
| Polyuria after episode | Paroxysmal SVT — ANP release from atrial stretch |
| Sweating, tremors, hunger | Hypoglycaemia as precipitant |
| Anxiety, panic | Psychological — must exclude organic first |
Relationship Between Fatigue and Palpitations
"Sir, I specifically asked whether fatigue preceded or followed palpitations:"
| Scenario | Interpretation |
|---|---|
| Fatigue → then palpitations | Underlying cause (anaemia, hypothyroidism, cardiac failure) → compensatory tachycardia / secondary arrhythmia |
| Palpitations → then fatigue | Primary arrhythmia (e.g., fast AF) → reduced cardiac output → fatigue (tachycardia-induced cardiomyopathy if chronic) |
| Both simultaneously | Common underlying aetiology — e.g., anaemia causing both fatigue (↓ O₂ delivery) and sinus tachycardia (perceived as palpitations) |
Red Flags for Dangerous Arrhythmia — Must Ask
| Red Flag | Significance |
|---|---|
| Syncope during palpitations | VT, complete heart block, Brugada |
| Family history of sudden cardiac death | LQTS, Brugada, HCM, ARVC |
| Palpitations during exertion | VT, CPVT (catecholaminergic polymorphic VT) |
| Structural heart disease (known murmur, IHD) | VT in scar tissue |
| Palpitations that require A&E attendance | Suggests haemodynamically significant arrhythmia |
Common Diagnostic Scenarios — Linking Fatigue + Palpitations
| Diagnosis | Fatigue Pattern | Palpitation Character | Key Associated Features |
|---|---|---|---|
| Iron deficiency anaemia | Progressive, exertional | Regular, fast, gradual onset/offset | Pallor, heavy periods, pica, koilonychia, angular stomatitis |
| Hypothyroidism | Profound, constant, cold intolerance | Slow (bradycardia) OR occasional ectopics | Weight gain, constipation, dry skin, hair loss, hoarse voice, delayed reflexes |
| Hyperthyroidism | Heat intolerance, tremor, weight loss | Fast, irregular (AF in 10%) OR regular tachy | Goitre, exophthalmos, lid lag, sweating, diarrhoea, tremor |
| Atrial fibrillation | From ↓ cardiac output | Irregularly irregular, fast | Pulse deficit, no S4, no presystolic accentuation |
| Cardiac failure | Exertional, with orthopnoea/PND | Sinus tachy or AF | Elevated JVP, S3, displaced apex, basal crepitations |
| Anxiety/Panic disorder | Worse with stress | Situational, with hyperventilation | Paraesthesias, dyspnoea, normal cardiac exam |
| Diabetes mellitus | Polyuria, polydipsia | Sinus tachycardia from hypoglycaemia | Polyuria, polydipsia, weight loss |
| Infective endocarditis | Fever, night sweats | AF or ectopics from cardiac involvement | Fever, changing murmur, splinter haemorrhages, Osler's nodes |
| Ectopic beats (PAC/PVC) | Mild, not prominent | Single thuds/"missed beat", low rate | Normal exam, normal echo — reassure |
Summarised HOPI Paragraph
"Sir, the patient was apparently well 4 months ago when he developed insidious onset, progressively worsening fatigue. He describes this as generalised weakness and easy fatigability on mild exertion, not relieved adequately by rest. He notices pallor on his own face in the mirror. He has had heavy menstrual periods for the past 6 months, lasting 7–8 days per cycle with clot passage. Two months after the onset of fatigue, he began experiencing palpitations. These are episodic, lasting 5–10 minutes each, sudden in onset and offset, regular and fast in rhythm. There is no associated syncope, chest pain, or breathlessness during episodes. He has mild exertional breathlessness (NYHA class II) and no orthopnoea or pedal oedema. There is no history of fever, night sweats, weight loss, thyroid symptoms, polyuria, polydipsia, or drug use. He has no prior cardiac history or family history of sudden cardiac death. On direct questioning, fatigue clearly preceded palpitations by 2 months, suggesting the palpitations are secondary — most likely sinus tachycardia from underlying iron deficiency anaemia. My provisional diagnosis is iron deficiency anaemia with compensatory sinus tachycardia, secondary to menorrhagia."
History diagnosis for complaint of breathelssness on exertion 6 months, fatigue 6 months palpitations 1 month
Full History & Provisional Diagnosis
Chief Complaints: Breathlessness on Exertion (6 months) + Fatigue (6 months) + Palpitations (1 month)
BIODATA
| Name | Mrs. Sunita D. |
| Age | 28 years |
| Sex | Female |
| Occupation | Housewife |
| Residence | Rural Rajasthan |
| Marital status | Married, 2 children |
| Informant | Patient herself (reliable) |
CHIEF COMPLAINTS
- Breathlessness on exertion — 6 months
- Easy fatigability — 6 months
- Palpitations — 1 month
HISTORY OF PRESENT ILLNESS
1. BREATHLESSNESS ON EXERTION
Onset and Progression
- Onset: Insidious, 6 months ago
- Initially on heavy exertion — climbing 2 flights of stairs, carrying heavy loads — NYHA Class II
- Progression: Gradually worsening over 6 months
- Now breathless on mild exertion — walking 100–200 metres on flat ground, doing light housework — NYHA Class II–III
- No breathlessness at rest currently
Orthopnoea
- Asks: "Do you need extra pillows to sleep? Do you feel uncomfortable lying flat?"
- Absent (if present → suggests cardiac failure, massive pleural effusion)
- Alternatively: 1 pillow since 2 months (mild orthopnoea → early cardiac decompensation)
Paroxysmal Nocturnal Dyspnoea (PND)
- Absent — patient sleeps through the night
- (If present → cardiac failure or severe mitral stenosis — cardiac asthma)
Character of Breathlessness
- Exertional only at this stage
- No wheeze (rules out asthma/COPD)
- No stridor (rules out upper airway obstruction)
- No positional variation other than described
Aggravating Factors
- Exertion — consistently
- Emotional stress
- Pregnancy — ask specifically (breathlessness may have been precipitated or worsened by pregnancy in a woman with pre-existing cardiac or haematological disease)
Relieving Factors
- Rest — complete relief within minutes of stopping exertion
- Note: Relief with rest suggests cardiac or haematological cause; incomplete relief suggests pulmonary cause
Progression Chart
| Time | Exertion Tolerance | NYHA Class |
|---|---|---|
| 6 months ago | Heavy exertion (2 flights stairs) | II |
| 3 months ago | Moderate exertion (1 flight, brisk walk) | II–III |
| Now | Mild exertion (100 metres flat) | III |
2. FATIGUE / EASY FATIGABILITY
Onset and Duration
- Same onset as breathlessness — 6 months ago, insidious
- Both symptoms appeared simultaneously — important clue (common underlying aetiology)
Character
- Generalised weakness — "body feels heavy," "no energy from morning"
- Unable to complete daily household work — cooking, sweeping, carrying water
- Not relieved adequately by rest — present even after full night's sleep
- Worsening progressively over 6 months
Associated with Fatigue — Systematically Ask:
| Question | Finding | Significance |
|---|---|---|
| Pallor noticed? | Yes — family noticed her face becoming pale over 6 months | Anaemia |
| Yellow discolouration of eyes? | Absent | Excludes haemolytic anaemia, liver disease |
| Bleeding from any site? | Heavy menstrual periods — 7–8 days, with clots, uses 6–8 pads/day × 6 months | Iron deficiency anaemia from menorrhagia |
| Blood in stools? | Absent | |
| Blood in urine? | Absent | |
| Weight loss? | Mild — 3 kg over 6 months | Could be due to poor intake or chronic disease |
| Appetite? | Decreased | Anaemia, cardiac failure, or chronic disease |
| Pica? | Asks specifically — craving for mud/chalk/ice (pagophagia) | Pathognomonic of iron deficiency — if present, strongly supports diagnosis |
| Cold intolerance, dry skin, hair loss, constipation, hoarse voice? | Absent | Excludes hypothyroidism |
| Excessive sweating, heat intolerance, tremors, diarrhoea? | Absent | Excludes hyperthyroidism |
| Fever or night sweats? | Absent | Excludes TB, lymphoma, infective endocarditis |
| Polyuria, polydipsia? | Absent | Excludes diabetes |
| Joint pains, rashes, oral ulcers? | Absent | Excludes SLE, connective tissue disease |
| Swelling of ankles? | Mild bilateral pedal oedema since 3 weeks | Cardiac decompensation, anaemia-induced high-output failure, or hypoalbuminaemia |
3. PALPITATIONS
Onset and Duration
- Onset: 1 month ago — after breathlessness and fatigue by 5 months
- Temporal sequence: Fatigue + breathlessness → then palpitations (palpitations appear later)
- This sequence strongly suggests palpitations are secondary to the underlying cause (compensatory tachycardia)
Character
| Feature | Finding |
|---|---|
| Rhythm | Regular |
| Rate | Fast — patient estimates heartbeat is racing |
| Onset | Gradual — builds up with exertion |
| Offset | Gradual — slows down with rest |
| Continuous or episodic | Episodic — mainly during exertion and occasionally at rest |
Examiner Q: What does gradual onset and offset with regular rhythm suggest? Answer: Sinus tachycardia — gradual onset/offset, regular, triggered by exertion or stress. Abrupt onset/offset suggests re-entrant SVT or AF.
Duration of Each Episode
- Coincides with exertion — lasts as long as she is active
- Settles within 5 minutes of rest
Precipitating Factors
- Exertion — primarily
- Emotional stress — occasionally
- No caffeine excess, no alcohol
Termination
- Spontaneous with rest — no manoeuvres needed, no medical intervention required
Associated Symptoms During Palpitation
| Symptom | Present/Absent | Significance |
|---|---|---|
| Syncope or pre-syncope | Absent | No haemodynamic compromise |
| Chest pain | Absent | No ischaemia |
| Neck throbbing | Absent | No AV dissociation |
| Breathlessness | Present — same episodes | Palpitations occur with exertional breathlessness — same trigger |
| Polyuria after episode | Absent | Not SVT |
Red Flags — Specifically Ask
- No syncope during palpitations
- No family history of sudden cardiac death
- No known cardiac disease
- Palpitations do not occur exclusively at rest or nocturnally
- Palpitations never required hospital attendance
LINKING THE THREE SYMPTOMS — KEY VIVA POINT
"Sir, I would like to draw the examiner's attention to the temporal relationship between the three symptoms:"
6 months ago: Breathlessness on exertion + Fatigue (simultaneous onset)
↓
Both suggest same underlying aetiology
↓
1 month ago: Palpitations develop (secondary, later symptom)
↓
Palpitations gradual onset/offset, regular, exertional
↓
= Sinus tachycardia (compensatory)
Moderate-to-severe Iron Deficiency Anaemia
PAST HISTORY
| System | Finding | Significance |
|---|---|---|
| Menstrual history | Menarche at 13; regular 28-day cycles; menorrhagia for 6–8 months — 7–8 days, clot passage, 6–8 pads/day, dysmenorrhoea present | Primary cause of iron loss |
| Obstetric history | G3P2L2 — last delivery 18 months ago; no significant PPH; breastfed for 12 months; did not receive iron supplements post-delivery | Iron depletion from pregnancy + lactation |
| Dietary history | Predominantly vegetarian — chapati, dal, limited green leafy vegetables; no meat, no organ foods | ↓ Dietary iron intake; non-haem iron poorly absorbed |
| Previous anaemia | Was told she had "low blood" during second pregnancy — took iron tablets for 2–3 months then stopped | Prior iron deficiency — inadequately treated |
| Cardiac disease | No known murmur, no rheumatic fever | Important to exclude cardiac cause |
| TB / chronic disease | No history of TB, no prolonged fever, no anti-TB treatment | Excludes anaemia of chronic disease |
| Worm infestation | Possible — lives in rural area, consumes well water, walks barefoot | Hookworm — important co-cause of iron deficiency in India |
| Surgery | No previous surgery; no gastrectomy | Gastrectomy → ↓ acid → ↓ iron absorption |
| Drug history | No NSAIDs, no antacids, no H2 blockers, no PPIs | Drugs that impair iron absorption or cause GI blood loss |
| Hypertension / DM | Not known | |
| Thyroid disease | No prior diagnosis | |
| Blood transfusion | None | |
| Allergy | None |
FAMILY HISTORY
| Anaemia | Mother also reported as "low blood" — suggests familial pattern (dietary, thalassaemia trait, G6PD) |
| Thalassaemia | No known diagnosis; ask specifically in Indian context |
| Cardiac disease | No family history of heart disease or sudden death |
| Malignancy | Absent |
PERSONAL HISTORY
| Domain | Finding | Significance |
|---|---|---|
| Diet | Predominantly vegetarian, inadequate green leafy vegetables, no meat | ↓ Iron intake |
| Appetite | Decreased for 3–4 months | Chronic disease/anaemia |
| Pica | Yes — craves chalk/mud (geophagia) for past 3 months | Pathognomonic of iron deficiency |
| Bowel habits | Normal — no melaena, no haematochezia | Excludes GI blood loss |
| Micturition | Normal — no haematuria | |
| Sleep | Disturbed — exertional limitations by day; no PND | |
| Menstrual | Detailed above — menorrhagia × 6–8 months | Primary aetiology |
| Addiction | Non-smoker, no alcohol, no tobacco | |
| Socioeconomic status | Lower middle class, inadequate dietary diversity | Nutritional contribution |
| Occupation | Housewife — heavy domestic work now limited | Functional impact |
GENERAL EXAMINATION
| Sign | Finding |
|---|---|
| Built and nourishment | Thin, moderately nourished |
| Pallor | Marked — conjunctival, palmar, mucosal pallor (inner lower eyelid most reliable) |
| Icterus | Absent |
| Cyanosis | Absent |
| Clubbing | Absent (clubbing in IDA only in long-standing severe cases — koilonychia more typical) |
| Koilonychia | Present — spoon-shaped nails (iron deficiency) |
| Angular stomatitis | Present — cracks at corners of mouth |
| Glossitis | Present — smooth, atrophic tongue (loss of papillae) |
| Brittle hair and nails | Present |
| Pedal oedema | Mild bilateral pitting — high-output cardiac state from severe anaemia |
| Lymphadenopathy | Absent |
| Pulse | Tachycardia — 104/min, regular, high volume, bounding (high-output state) |
| BP | 100/70 mmHg — mildly low |
| Respiratory rate | 20/min |
| JVP | Normal or mildly raised if high-output failure |
CVS EXAMINATION FINDINGS (Brief)
| Finding | Significance |
|---|---|
| Apex beat | Hyperdynamic, may be slightly displaced (high-output state dilates LV) |
| Haemic murmur | Soft systolic flow murmur at pulmonary/mitral area — Grade 1–2/6, soft, blowing, no thrill, no radiation — from ↑ flow velocity across normal valves in anaemia |
| S1, S2 | Normal |
| No diastolic murmur | Excludes mitral stenosis |
| No signs of valve disease | Excludes rheumatic/structural cause |
PROVISIONAL DIAGNOSIS
Primary Diagnosis
"Sir, my provisional diagnosis is Moderate to Severe Iron Deficiency Anaemia, most likely secondary to chronic menorrhagia, compounded by inadequate dietary iron intake, recent pregnancy and lactation, and possible hookworm infestation — presenting with high-output cardiac state manifesting as exertional breathlessness, fatigue, and compensatory sinus tachycardia."
Supporting Evidence Summary
| Feature | Supports IDA |
|---|---|
| Young woman, rural, vegetarian | Epidemiology |
| Menorrhagia × 6–8 months | Chronic iron loss |
| Recent pregnancy + lactation without supplementation | Increased demand + depletion |
| Simultaneous breathlessness + fatigue (6 months) | ↓ Hb → ↓ O₂ carrying capacity |
| Compensatory sinus tachycardia later (1 month) | Secondary high-output state |
| Koilonychia, angular stomatitis, glossitis | Classic iron deficiency signs |
| Pica (chalk/mud craving) | Pathognomonic of IDA |
| Pallor | Anaemia |
| Bounding pulse, haemic murmur | High-output circulation |
| Gradual onset/offset palpitations with exertion | Sinus tachycardia, not arrhythmia |
Differential Diagnoses
| Diagnosis | For | Against |
|---|---|---|
| Thalassaemia trait | Similar demographics, anaemia, fatigue | Milder symptoms, splenomegaly, family history; MCV disproportionately low for Hb level; haemoglobin electrophoresis distinguishes |
| Anaemia of chronic disease | Fatigue, pallor | No chronic infection/inflammation/malignancy history; ferritin high in ACD (low in IDA) |
| Hypothyroidism | Fatigue, menorrhagia, weight gain | No cold intolerance, no dry skin, no constipation, no bradycardia; normal thyroid on examination |
| Rheumatic heart disease (Mitral stenosis) | Young Indian woman, breathlessness, palpitations | No childhood RF history; no opening snap; no presystolic murmur; no loud S1; no AF |
| Cardiac failure | Breathlessness, fatigue, pedal oedema | No elevated JVP, no S3, no displaced apex, no basal crepitations, no orthopnoea; young patient, no structural disease |
| Hyperthyroidism | Palpitations, fatigue, weight loss | No heat intolerance, no tremor, no goitre, no exophthalmos, no diarrhoea; pulse regular not irregular |
| Hookworm infestation | Rural, barefoot, well water | Co-cause, not primary diagnosis; eosinophilia on FBC would support |
Investigations to Order
Confirmatory
| Test | Expected Finding in IDA |
|---|---|
| Complete Blood Count (CBC) | ↓ Hb (<8 g/dL severe); microcytic (↓ MCV <80 fL); hypochromic (↓ MCH <27 pg); ↑ RDW (anisocytosis) |
| Peripheral blood smear | Microcytes, hypochromia, elliptocytes, pencil cells, anisocytosis, poikilocytosis |
| Serum ferritin | ↓ <12 ng/mL — most sensitive and specific for iron deficiency |
| Serum iron | ↓ (<60 μg/dL) |
| TIBC (Total Iron Binding Capacity) | ↑ (>400 μg/dL) — inverse to iron stores |
| Transferrin saturation | ↓ (<20%) |
| Reticulocyte count | Normal or mildly ↑ — if on iron treatment, ↑ sharply (reticulocyte crisis at day 7–10) |
To Identify Cause
| Test | Rationale |
|---|---|
| Stool for occult blood | GI blood loss |
| Stool for ova and cysts | Hookworm (Ancylostoma duodenale) — major cause in rural India |
| Urine R/M | Haematuria |
| Gynaecological evaluation | Menorrhagia — pelvic USS, hormonal work-up |
| Thyroid function tests | Hypothyroidism causes menorrhagia |
| Haemoglobin electrophoresis | Exclude thalassaemia trait (↑ HbA2 in beta-thal trait) |
| Serum B12 and folate | Concurrent deficiency (common in India) — may mask macrocytosis |
Cardiac
| Test | Rationale |
|---|---|
| ECG | Sinus tachycardia, non-specific ST-T changes from anaemia |
| Chest X-ray | Cardiomegaly (high-output), pulmonary congestion if decompensated |
| Echocardiogram | If murmur or cardiomegaly to exclude structural disease |
Management Outline
Immediate
- Oral iron: Ferrous sulphate 200 mg TDS (65 mg elemental iron/tablet) — with Vitamin C (orange juice) to enhance absorption; avoid with tea, calcium, antacids
- Dietary counselling: Green leafy vegetables, jaggery, dates, beans, meat (if acceptable); avoid inhibitors (tea, phytates)
- Deworming: Albendazole 400 mg single dose if hookworm suspected
- Treat menorrhagia: Tranexamic acid, mefenamic acid; refer gynaecology for evaluation
Monitoring Response
- Reticulocyte peak at day 7–10 after starting iron
- Hb rise of 1–2 g/dL per week expected
- Continue iron for 3 months after Hb normalises to replenish stores
- Recheck ferritin to confirm store replenishment
Transfusion
- If Hb <7 g/dL with haemodynamic compromise or symptoms of cardiac failure → packed red cell transfusion
Final One-Liner (Viva Summary)
"Sir, this is a case of a 28-year-old housewife from rural Rajasthan, presenting with a 6-month history of progressively worsening exertional breathlessness and generalised fatigue, followed by exertional palpitations for 1 month. The temporal sequence — breathlessness and fatigue appearing simultaneously 6 months prior, with palpitations developing later as a compensatory phenomenon — in a young vegetarian woman with chronic menorrhagia, recent pregnancy and lactation without iron supplementation, and pica, is highly consistent with moderate-to-severe iron deficiency anaemia causing a high-output cardiac state. On examination, she has marked pallor, koilonychia, angular stomatitis, atrophic glossitis, tachycardia with a bounding pulse, and a soft haemic systolic flow murmur with normal heart sounds and no signs of structural cardiac disease, further supporting my provisional diagnosis of iron deficiency anaemia secondary to chronic menorrhagia with possible hookworm co-infestation."