Kartagener syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
Kartagener syndrome primary ciliary dyskinesia
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have everything needed for a complete, well-illustrated answer.
Kartagener Syndrome
Kartagener syndrome is a clinical variant of Primary Ciliary Dyskinesia (PCD), defined by the classic triad:
- Situs inversus (complete mirror-image reversal of thoracic and abdominal organs)
- Chronic sinusitis (and/or rhinosinusitis)
- Bronchiectasis
It is also called the Kartagener triad or immotile cilia syndrome (when the broader ciliary dysfunction is emphasized).
- K J Lee's Essential Otolaryngology, p. 48
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1, p. 1087
Genetics and Epidemiology
-
Inheritance: Autosomal recessive
-
Prevalence: PCD affects approximately 1 in 20,000 individuals at birth; Kartagener syndrome accounts for ~50% of all PCD cases (i.e., those with situs inversus)
-
Gene defects: Mutations in genes encoding dynein arm components (e.g., DNAI1, DNAI2, DNAAF1/KTU, DNAAF2, and >50 other PCD-associated genes). No single gene accounts for all cases.
-
Histology: A Text and Atlas, p. 784
Pathophysiology
The root cause is a structural defect in the axonemal dynein arms of cilia and flagella. Normal cilia have a 9+2 microtubule arrangement with outer and inner dynein arms that generate the ATP-powered sliding force for ciliary beating.
In Kartagener/PCD:
- The dynein arms are absent (outer, inner, or both) from the A-tubules of peripheral microtubule doublets
- Basal bodies are often misoriented (feet point in random directions rather than a uniform orientation)
- Result: absent or severely reduced ciliary beat frequency and coordination → failure of mucociliary transport
Why situs inversus occurs: During embryonic development, nodal cilia in the embryonic node normally beat in a directional manner to establish left-right asymmetry. When these cilia are dysfunctional, laterality is determined randomly, giving a ~50% chance of situs inversus in affected individuals - which is why only half of PCD patients develop Kartagener syndrome.
- Histology: A Text and Atlas, pp. 784-787
- Junqueira's Basic Histology, p. 350
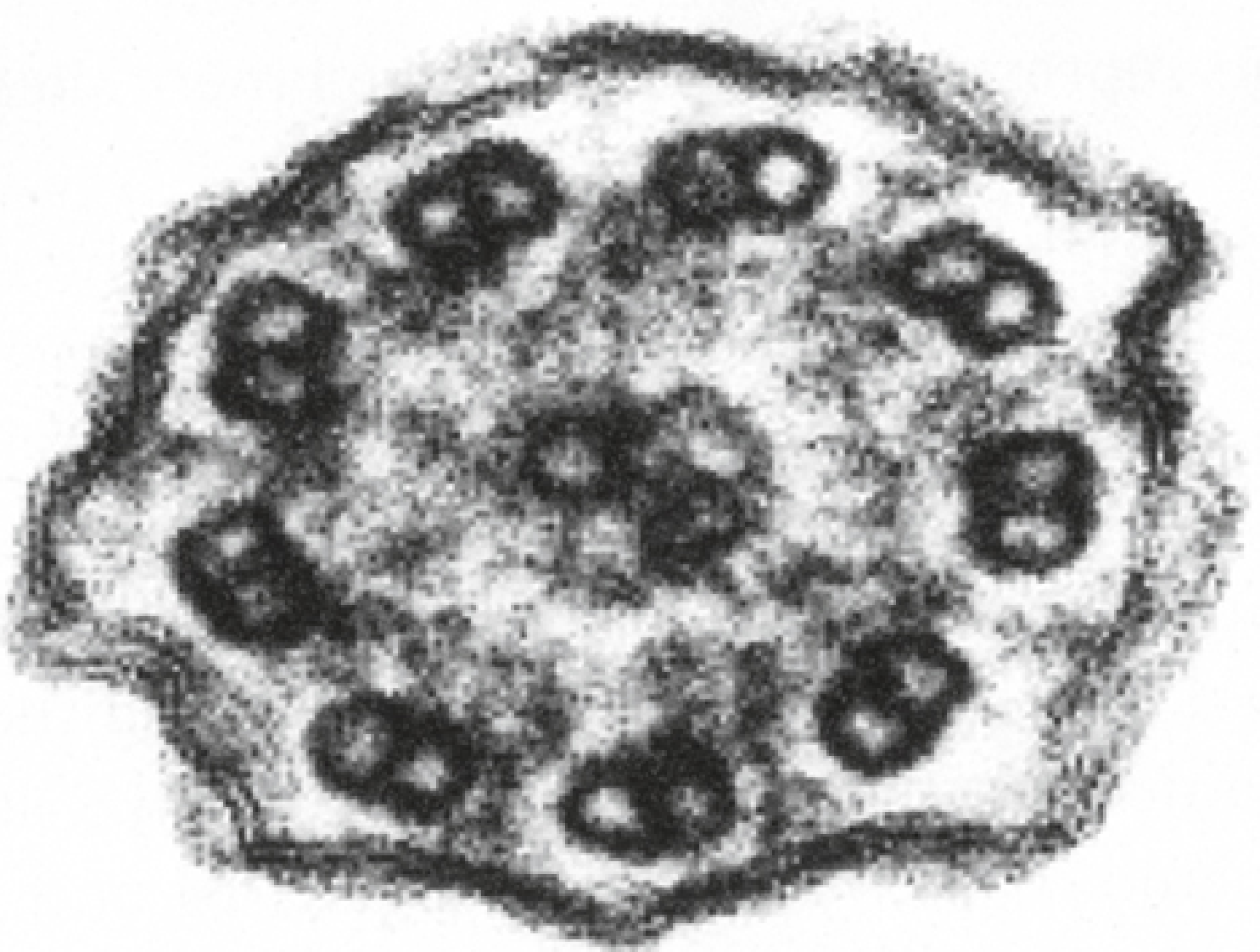
Electron Micrograph - Absent Dynein Arms
This cross-section EM of a cilium from a PCD patient shows the 9+2 doublets with absent dynein arms (compare to normal cilia where arm projections are clearly visible on each doublet):
Clinical Features
The clinical manifestations reflect where motile cilia are distributed:
Respiratory Tract
- Recurrent sinusitis / rhinosinusitis - year-round, beginning in infancy
- Nasal polyps - present in ~27% of Kartagener patients
- Bronchiectasis - progressive airway damage from recurrent infections; basal predominant
- Chronic productive cough - from early childhood (<6 months of age)
- Recurrent otitis media - from Eustachian tube ciliary dysfunction
- Neonatal respiratory distress - a common early clue
Reproductive System
- Male infertility (virtually universal) - sperm flagella share the same 9+2 dynein arm structure; immotile flagella = azoospermia/asthenospermia. Spermatogenesis is normal, but the sperm cannot swim.
- Female subfertility - fallopian tube cilia are also impaired. Females may occasionally be fertile if residual ciliary movement is sufficient, but there is an increased risk of ectopic pregnancy due to impaired ovum transport.
CNS
- Hydrocephalus internus (rare) - ependymal cells lining the CSF spaces possess motile cilia; dysfunction may impair CSF circulation through narrow inter-ventricular spaces.
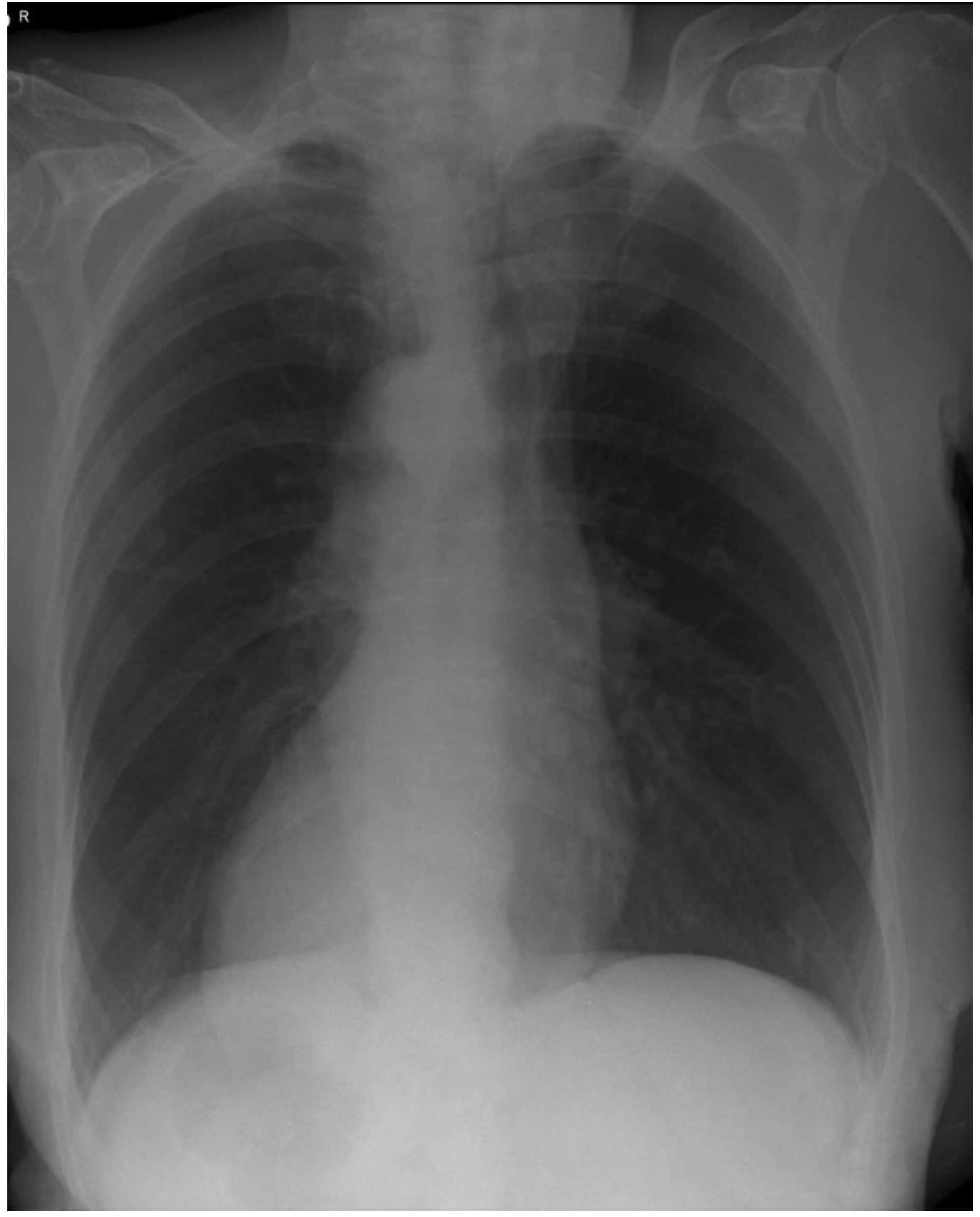
Chest X-Ray and CT Findings
Chest radiograph showing dextrocardia (heart on the right) - one of the hallmarks of situs inversus:
Frontal CXR + Axial CT in Kartagener syndrome: dextrocardia with basal linear opacities (bronchial wall thickening) on CXR (A); severe cystic bronchiectasis on CT, particularly on the left, with the left lung showing a morphologic configuration resembling a right middle lobe (arrow in B):
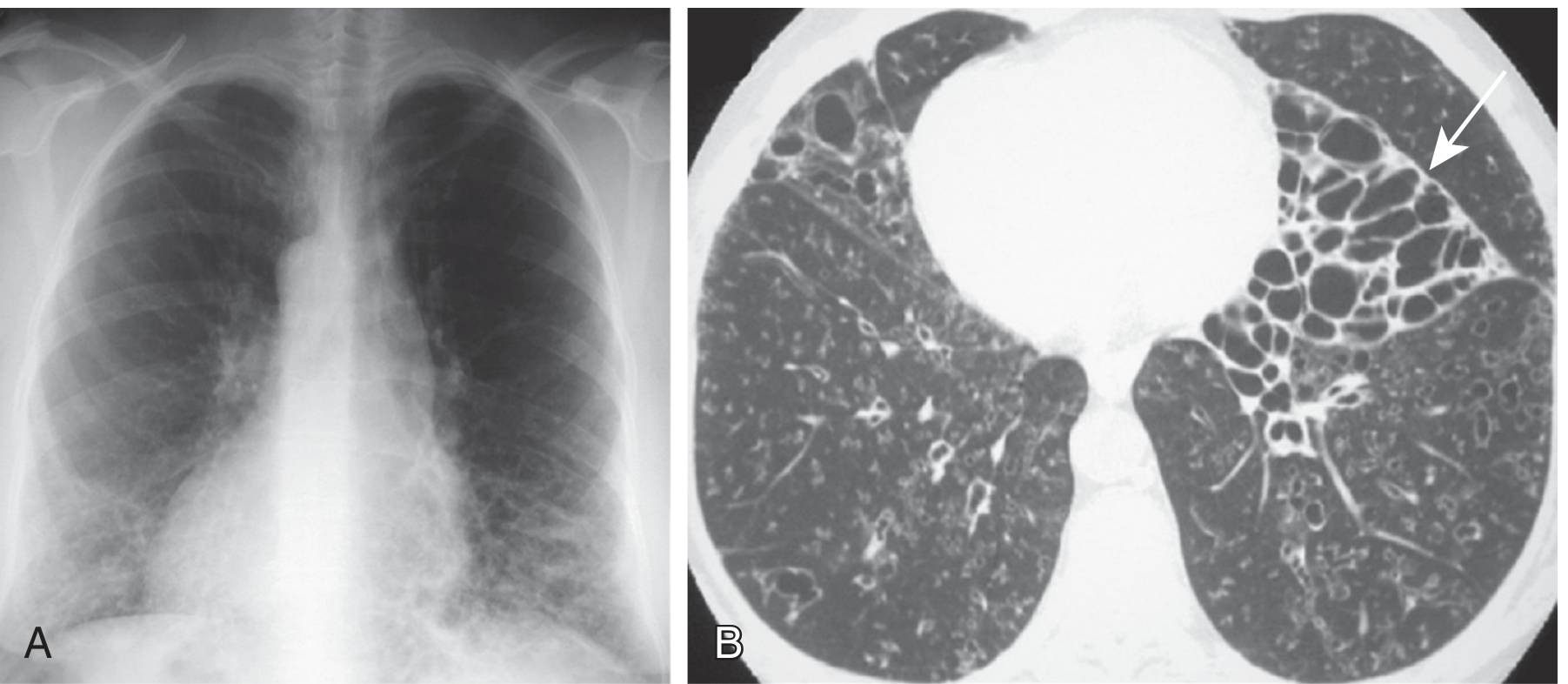
- Murray & Nadel's Textbook of Respiratory Medicine, p. 1596
- Goldman-Cecil Medicine, p. 3739
Diagnosis
Clinical suspicion is triggered by the presence of ≥2 key features (per the ATS PCD guidelines):
- Unexplained neonatal respiratory distress
- Year-round daily cough beginning before 6 months of age
- Year-round daily rhinosinusitis beginning before 6 months
- Abnormal organ laterality (situs inversus/heterotaxy)
Diagnostic Algorithm (ATS 2018)
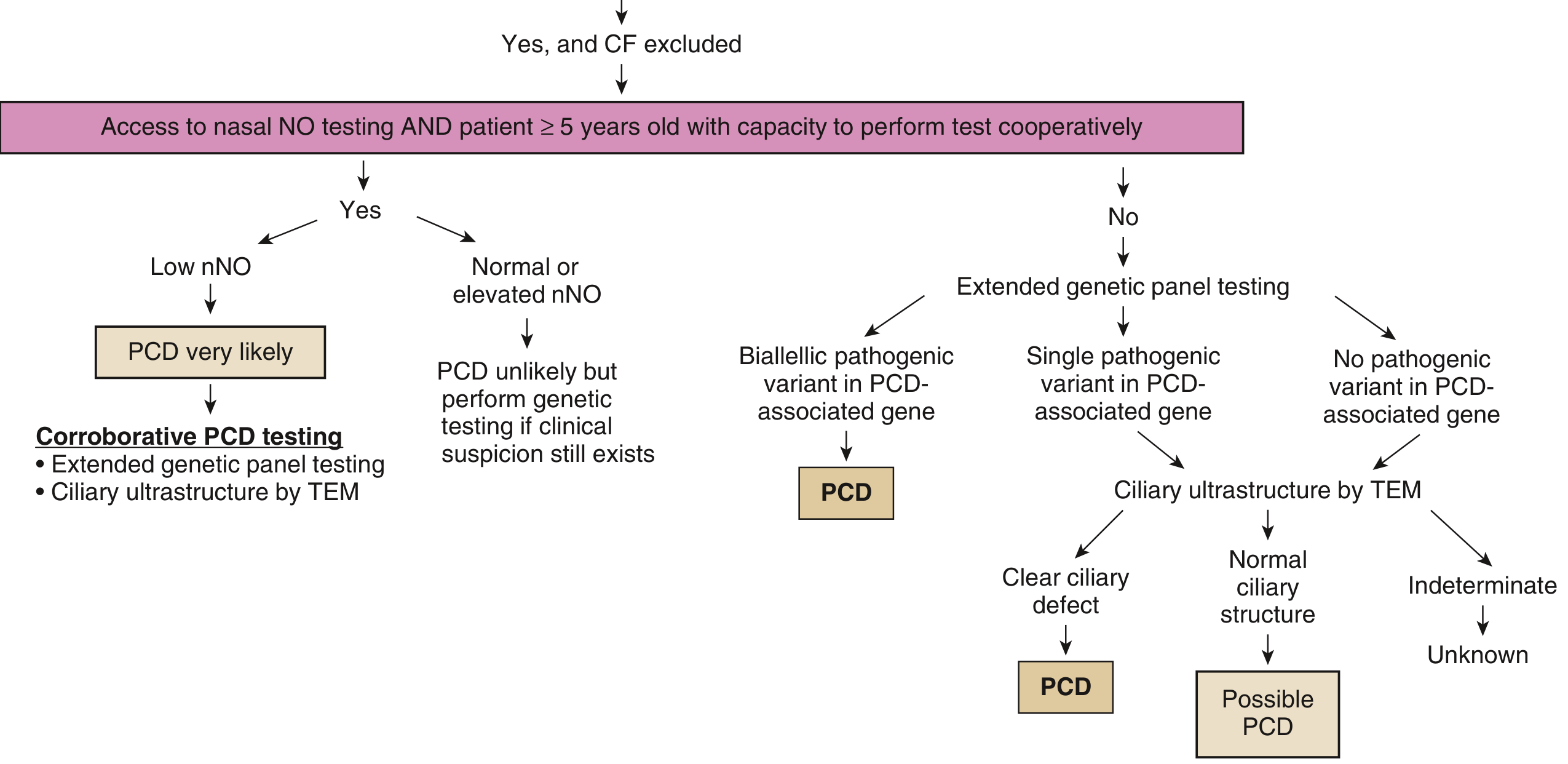
Key tests:
| Test | Details |
|---|---|
| Nasal nitric oxide (nNO) | Markedly low in PCD (nNO is produced by sinuses and is impaired in ciliary dysfunction). Requires patient ≥5 years old. First exclude CF (significant minority of CF patients also have low nNO). |
| Extended genetic panel testing | Biallelic pathogenic variants in a PCD-associated gene = diagnostic. >50 genes known. |
| Transmission electron microscopy (TEM) | Gold standard for showing dynein arm defects, but ~30% of PCD patients have normal or near-normal TEM - poor sensitivity. |
| High-speed video microscopy | Assesses ciliary beat frequency/pattern; suffers from low specificity (chronic infection can secondarily impair cilia). |
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 1596-1597
Management
There is no cure; management is supportive and aimed at minimizing airway damage:
- Airway clearance techniques - chest physiotherapy, positive expiratory pressure devices, mucolytics (hypertonic saline); a 2024 systematic review (PMID 39269762) found airway clearance is a mainstay of therapy but evidence on optimal techniques remains limited.
- Antibiotic therapy - prompt treatment of respiratory exacerbations; long-term low-dose macrolides for their anti-inflammatory effects (used similarly to bronchiectasis management).
- Sinus management - endoscopic sinus surgery for refractory sinusitis and polyposis.
- Fertility counseling - for both male (assisted reproduction via ICSI using morphologically normal sperm) and female patients.
- Surveillance - regular pulmonary function tests, CT chest monitoring, hearing assessments (for otitis media sequelae).
- Lung transplantation in end-stage disease.
Key Summary Table
| Feature | Detail |
|---|---|
| Classic triad | Situs inversus + Chronic sinusitis + Bronchiectasis |
| Inheritance | Autosomal recessive |
| Core defect | Absent dynein arms on ciliary A-tubules |
| % of PCD with situs inversus | ~50% |
| Male fertility | Almost always infertile (immotile sperm) |
| Female fertility | Subfertile; increased ectopic pregnancy risk |
| Nasal polyps | ~27% |
| Screening test | Nasal nitric oxide (low) |
| Gold standard | TEM (but 30% false negative) |
| Confirmatory | Biallelic PCD gene mutations |
This is a shared conversation. Sign in to Orris to start your own chat.