Give me the pathology aspects of sickle cell anemia required to study for neet pg 2026.
sickle cell anemia pathology molecular basis pathophysiology
sickle cell anemia morphology complications organ damage lab findings
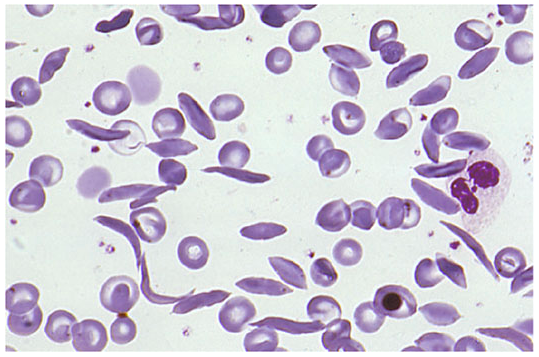
sickle cell anemia blood smear morphology pathology
Sickle Cell Anemia — Pathology (NEET PG 2026)
1. Genetics & Molecular Basis
| Feature | Detail |
|---|---|
| Gene | HBB gene (chromosome 11p15.5) |
| Mutation | Point mutation — GAG → GTG (codon 6 of β-globin gene) |
| Amino acid change | Glutamic acid → Valine at position 6 of β-globin chain |
| Type of mutation | Missense mutation |
| Inheritance | Autosomal recessive |
| Hemoglobin | HbS (α₂β₂ˢ) |
| Trait (carrier) | HbAS — typically asymptomatic; protects against P. falciparum malaria |
| Disease | HbSS — full sickle cell disease |
Key NEET fact: The substitution of hydrophilic glutamic acid by hydrophobic valine creates a sticky hydrophobic patch on the β-globin chain, driving polymerization under deoxygenation.
2. Pathophysiology — The Sickling Process
Step-by-step mechanism:
- Deoxygenation → HbS polymerizes due to hydrophobic valine-valine contacts between β-globin chains
- Polymer formation → Forms long, rigid tactoids (fascicles) that distort the RBC membrane
- RBC shape changes → Classic sickle/crescent shape
- Reversible vs. Irreversible sickling:
- Early: sickling is reversible on reoxygenation
- Repeated episodes → irreversibly sickled cells (ISC) persist even when oxygenated
- Membrane damage → HbS polymer penetrates membrane → vesiculation, microparticle release, increased ion channel activity (Gardos channel, K/Cl cotransport, Psickle)
- Cellular dehydration → Increased mean corpuscular hemoglobin concentration (MCHC) → facilitates further polymerization
Key facilitators of sickling:
- Hypoxia (most important)
- Acidosis (↓ pH) — right shift of oxygen-dissociation curve
- Dehydration
- Infection/fever
- Cold temperature
- High HbS concentration
Key NEET fact: Fetal hemoglobin (HbF) inhibits sickling — it does NOT participate in polymer formation. This is the rationale for hydroxyurea (↑ HbF production).
3. Blood Smear / Morphology
| Finding | Significance |
|---|---|
| Sickle cells (drepanocytes) | Pathognomonic |
| Target cells | Due to asplenia (functional) |
| Howell-Jolly bodies | Due to functional hyposplenism |
| Polychromasia / reticulocytosis | Compensatory hemolysis |
| Nucleated RBCs | Stress erythropoiesis |
| Anisocytosis & poikilocytosis | General RBC membrane damage |
4. Types of Hemoglobin Variants (NEET High Yield)
| Genotype | HbS% | HbA% | HbF% | HbA2% | Severity |
|---|---|---|---|---|---|
| Normal | 0 | 96–98 | <1 | 2–3 | — |
| Sickle trait (HbAS) | 40 | 55–60 | <1 | 2–3 | Asymptomatic |
| Sickle cell anemia (HbSS) | 85–95 | 0 | 5–15 | 2–4 | Severe |
| HbSC disease | 50 (HbS) | 0 | <1 | 0; 50% HbC | Moderate |
| HbS-β⁰ thalassemia | >90 | 0 | ↑ | ↑ | Severe |
| HbS-β⁺ thalassemia | 60–85 | <25 | ↑ | ↑ | Mild-Moderate |
5. Vaso-occlusion — The Central Pathologic Event
- Sickled RBCs are rigid and sticky → adhere to vascular endothelium
- Activation of endothelium → upregulation of adhesion molecules (VCAM-1, ICAM-1, P-selectin, E-selectin)
- Adhesion cascade: sickled RBC → neutrophil bridging → vascular occlusion
- Ischemia → infarction of downstream tissues
6. Organ Pathology (Organ-Specific Changes)
Spleen
- Early childhood: splenomegaly (congestion due to RBC trapping)
- Progressive: repeated infarcts → autosplenectomy (by age 5–8 years in HbSS)
- Result: Functional asplenia → susceptibility to encapsulated organisms:
- Streptococcus pneumoniae (most common)
- Haemophilus influenzae
- Salmonella (osteomyelitis — most common organism in SCA)
- Neisseria meningitidis
NEET Key: Most common cause of death in children with SCA = Pneumococcal sepsis
Bone
- Bone marrow hyperplasia → expansion of medullary cavity
- "Hair-on-end" / crew-cut appearance on skull X-ray
- "Bone-in-bone" / "Lincoln Log" vertebrae (H-shaped/fish-mouth vertebrae on X-ray)
- Avascular necrosis (AVN) of femoral/humeral heads
- Dactylitis ("hand-foot syndrome") — earliest manifestation in infants (6 months–2 years); periostitis of small bones of hands/feet
- Osteomyelitis: Salmonella > Staph. aureus (reverse of normal population)
Kidney
- Hyposthenuria — inability to concentrate urine (medullary hypoxia destroys concentrating mechanism)
- Papillary necrosis — due to ischemia of renal medulla
- Hematuria — even in sickle trait (hypoxic medulla)
- Sickle cell nephropathy → CKD
Lung
- Acute Chest Syndrome (ACS): New infiltrate on CXR + fever + respiratory symptoms
- Most common cause of death in adults with SCA
- Causes: fat embolism (from bone marrow infarcts), infection, in situ thrombosis, pulmonary vaso-occlusion
- Pulmonary hypertension — chronic complication
Brain
- Stroke — most common serious neurological complication
- Children: large-vessel ischemic stroke (due to intimal proliferation)
- Adults: hemorrhagic stroke
Eye
- Proliferative sickle retinopathy — especially HbSC disease
- "Sea fan" neovascularization
Liver/Gallbladder
- Pigment gallstones (bilirubin stones) — due to chronic hemolysis → unconjugated hyperbilirubinemia
- Hepatomegaly — due to RBC trapping and extramedullary hematopoiesis
Skin
- Leg ulcers — due to vascular insufficiency (malleolar region most common)
Penis
- Priapism — sustained painful erection due to veno-occlusion in corpus cavernosum
7. Types of Crises in Sickle Cell Disease
| Crisis | Mechanism | Key Feature |
|---|---|---|
| Vaso-occlusive (painful) crisis | Sickling → vascular occlusion → infarction | Most common crisis |
| Aplastic crisis | Parvovirus B19 infects erythroid precursors → ↓ RBC production | ↓ Hb, ↓ reticulocytes, NO hemolysis |
| Sequestration crisis | Massive pooling of RBCs in spleen/liver | Rapid ↓ Hb, splenomegaly, shock; more in HbSC/infants |
| Hemolytic crisis | Accelerated hemolysis | ↑ LDH, ↑ bilirubin, ↓ Hb |
| Hyperhemolytic crisis | Often post-transfusion | Very low Hb, can be life-threatening |
| Megaloblastic crisis | Folate deficiency from high RBC turnover | Rare |
NEET Key: Aplastic crisis → Parvovirus B19 is the trigger. Sequestration crisis is the most life-threatening acute crisis.
8. Laboratory Diagnosis
| Test | Finding |
|---|---|
| CBC | Hb 6–9 g/dL, ↑ WBC, ↑ platelets (after autosplenectomy) |
| Reticulocyte count | Elevated (5–15%) |
| Peripheral smear | Sickle cells, target cells, Howell-Jolly bodies |
| Sickling test (Metabisulfite test) | Positive in trait AND disease (screening) |
| Sickle solubility test (Sickledex) | Positive (cannot distinguish trait from disease) |
| Hemoglobin electrophoresis | Gold standard for diagnosis and speciation |
| HPLC | Most sensitive/specific — used for newborn screening |
| Bilirubin | ↑ Unconjugated (hemolysis) |
| LDH | Elevated |
| Haptoglobin | ↓ or absent |
| Urinalysis | Hyposthenuria, hematuria, proteinuria |
9. Important Robbins Pathology Points (NEET PG Focus)
- Sickle cell anemia is the prototype of hemolytic anemias due to RBC membrane/structural defects resulting from abnormal hemoglobin
- Pathology is broadly due to:
- Chronic hemolytic anemia — extravascular hemolysis (RES) predominantly
- Vaso-occlusion and ischemic tissue damage
- Erythroid hyperplasia in bone marrow — compensatory; leads to bone changes
- Extramedullary hematopoiesis — spleen, liver
- The spleen in early disease shows congestion and red pulp expansion → later becomes a fibrotic, shrunken nubbin (autosplenectomy)
- Tissues show features of chronic ischemia + repeated infarcts
- Hemosiderosis — due to repeated transfusions and chronic hemolysis
10. High-Yield NEET PG One-Liners
- Mutation: GAG → GTG (Glu → Val, position 6, β-chain)
- Most common crisis: Vaso-occlusive/painful crisis
- Earliest manifestation in infants: Dactylitis
- Most common infection: Pneumococcal sepsis
- Most common organism in osteomyelitis: Salmonella
- Aplastic crisis trigger: Parvovirus B19
- Gold standard diagnosis: Hemoglobin electrophoresis
- Best screening test: HPLC (newborn screening)
- Drug that ↑ HbF: Hydroxyurea (also ↓ neutrophil adhesion, ↓ sickling)
- Renal finding: Hyposthenuria (earliest), then papillary necrosis
- Skull X-ray: Hair-on-end / crew-cut appearance
- Vertebrae: H-shaped / fish-mouth / Lincoln Log vertebrae
- Eye complication worst in: HbSC disease
- Most common cause of death in adults: Acute Chest Syndrome
- Most common cause of death in children: Pneumococcal sepsis
- HbF protects because: it does not participate in HbS polymer formation
- Sickle trait protects against: Plasmodium falciparum malaria
Now, based on the above, I want you to prepare Anki cards for AnkiDroid app. Front portion should be the question, back portion should be the answer. The question should mention the disease it is referring to unless it is a clinical question asking for diagnosis. Because this will help me to identify while revising overall which topic the question is referring to. Include maximum clinical questions which will help me to answer MCQs in NEET-PG. It should also include factual aspects regarding the topic and it should include only pathology topics regarding sickle cell anemia. And it should cover almost everything that can be asked for NEET-PG 2026. Now make sure not to cause repetition of questions like similar question or same answer for different questions. Avoid repetitions.
- Copy everything inside the code block into a
.txtfile (UTF-8), for example:Sickle_Cell_Pathology_NEETPG2026.txt - In AnkiDroid: Import File → choose tab-separated fields.
- Field 1 = Front, Field 2 = Back.
In sickle cell anemia, what is the exact genetic mutation in the β-globin gene? Point mutation in HBB gene at codon 6: GAG → GTG, causing Glutamic acid → Valine substitution (missense mutation).
In sickle cell anemia, what is the amino acid substitution responsible for disease pathogenesis? β6 Glutamic acid is replaced by Valine (Glu6Val).
In sickle cell anemia, what is the inheritance pattern? Autosomal recessive.
In sickle cell anemia, which abnormal hemoglobin is formed? HbS (α2βS2).
In sickle cell anemia, why does deoxygenation trigger sickling? Deoxygenated HbS polymerizes due to hydrophobic interaction of Val at β6, forming rigid polymers that distort RBCs.
In sickle cell anemia, what is the central pathological event causing organ damage? Vaso-occlusion by rigid sickled RBCs causing ischemia and infarction.
In sickle cell anemia, what are the two major mechanisms of pathology? 1) Chronic hemolytic anemia 2) Recurrent vaso-occlusion with tissue infarction.
In sickle cell anemia, does sickling start as reversible or irreversible? Initially reversible; repeated cycles cause membrane damage leading to irreversible sickled cells.
In sickle cell anemia, what is the role of RBC dehydration in pathogenesis? Dehydration increases intracellular HbS concentration (↑MCHC), promoting polymerization and sickling.
In sickle cell anemia, which physiological factors increase sickling? Hypoxia, acidosis, dehydration, infection/fever, cold exposure.
In sickle cell anemia, what protective role does HbF play? HbF inhibits HbS polymerization and reduces sickling.
In sickle cell anemia, why is hydroxyurea useful from a pathology perspective? It increases HbF, reducing HbS polymerization and vaso-occlusive pathology.
In sickle cell anemia, what is the classic peripheral smear finding? Sickle-shaped (crescent/drepanocyte) RBCs.
In sickle cell anemia, which additional RBC morphology is commonly seen on smear? Target cells, anisopoikilocytosis, polychromasia, nucleated RBCs.
In sickle cell anemia, why are Howell-Jolly bodies seen on peripheral smear? Functional hyposplenism/autosplenectomy causes reduced splenic pitting.
In sickle cell anemia, what marrow response occurs due to chronic hemolysis? Erythroid hyperplasia of bone marrow.
In sickle cell anemia, which skull radiologic appearance reflects marrow hyperplasia? Hair-on-end (crew-cut) appearance.
In sickle cell anemia, what vertebral radiologic change is classically described? H-shaped (fish-mouth/Lincoln log) vertebrae due to endplate infarction.
In sickle cell anemia, what is the early splenic pathology in childhood? Congestive splenomegaly due to trapping of sickled RBCs.
In sickle cell anemia, what is autosplenectomy? Repeated splenic infarctions causing fibrotic, shrunken nonfunctional spleen.
In sickle cell anemia, what major immunologic consequence follows autosplenectomy? Marked susceptibility to encapsulated organisms.
In sickle cell anemia, which organism is classically most associated with osteomyelitis? Salmonella species.
In sickle cell anemia, what is the pathology behind dactylitis in infants? Vaso-occlusive infarction of small bones of hands/feet.
In sickle cell anemia, what is the pathology of acute chest syndrome? Pulmonary vaso-occlusion/infarction ± infection ± fat embolism causing new infiltrate and hypoxia.
In sickle cell anemia, what is the renal medullary pathology causing early urinary defect? Medullary ischemic damage causing hyposthenuria (impaired urine concentration).
In sickle cell anemia, what renal structural lesion is classically associated with hematuria? Renal papillary necrosis.
In sickle cell anemia, what is the pathology behind pigment gallstones? Chronic hemolysis → increased unconjugated bilirubin → black pigment stones.
In sickle cell anemia, what causes priapism pathologically? Veno-occlusion in penile vasculature by sickled cells.
In sickle cell anemia, what is the basic vascular mechanism of painful crisis? Microvascular obstruction by sickled RBCs with endothelial adhesion and ischemia.
In sickle cell anemia, what is the most common type of crisis? Vaso-occlusive (painful) crisis.
In sickle cell anemia, what causes aplastic crisis? Parvovirus B19 infection suppressing erythropoiesis.
In sickle cell anemia, what lab pattern suggests aplastic crisis? Acute fall in hemoglobin with low/absent reticulocyte response.
In sickle cell anemia, what is sequestration crisis? Sudden pooling of blood in spleen/liver causing acute severe anemia and hypovolemia.
In sickle cell anemia, what is hemolytic crisis? Acute acceleration of hemolysis causing rapid Hb fall with high reticulocyte count.
In sickle cell anemia, what is the usual hemoglobin range in severe HbSS disease? Approximately 6-9 g/dL (chronic hemolytic baseline).
In sickle cell anemia, what are key hemolysis markers in blood tests? ↑Unconjugated bilirubin, ↑LDH, ↓haptoglobin, reticulocytosis.
In sickle cell anemia, what is the definitive test for identifying hemoglobin fractions? Hemoglobin electrophoresis (or HPLC for precise quantification).
In sickle cell anemia, can sickling/solubility screening tests distinguish trait from disease? No, they detect HbS presence but cannot reliably distinguish trait from HbSS disease.
In sickle cell anemia, what is the typical HbA level in HbSS on electrophoresis? HbA is absent (0%).
In sickle cell anemia, what change in leukocyte and platelet counts may occur with autosplenectomy? Leukocytosis and thrombocytosis.
In sickle cell anemia, what is the pathology basis of stroke risk in children? Cerebral vaso-occlusion and large-vessel vasculopathy causing ischemic infarcts.
In sickle cell anemia, what eye pathology is classically seen (especially in HbSC variant)? Proliferative retinopathy with sea-fan neovascularization.
In sickle cell anemia, what is the pathology basis of chronic leg ulcers? Repeated microvascular ischemia and poor tissue perfusion, typically near malleoli.
In sickle cell anemia, what causes avascular necrosis of femoral head? Recurrent vaso-occlusive infarction of bone epiphysis.
In sickle cell anemia, what is the pathologic significance of nucleated RBCs in peripheral blood? Marrow stress with intense compensatory erythropoiesis.
In sickle cell anemia, what is meant by functional asplenia? Presence of anatomically small/fibrotic spleen with loss of normal splenic immune-filtration function.
In sickle cell anemia, why are repeated infarcts seen in multiple organs? Intermittent microvascular obstruction by sickled erythrocytes causes recurrent ischemia.
A child with painful swollen hands and feet at 8 months has sickle cell anemia. What is this manifestation called? Dactylitis (hand-foot syndrome) due to vaso-occlusion of small bones.
A sickle cell anemia patient develops sudden severe anemia with very low reticulocyte count after viral prodrome. Most likely diagnosis? Aplastic crisis (classically Parvovirus B19).
A sickle cell anemia patient has fever, chest pain, hypoxia, and new pulmonary infiltrate. Most likely pathology diagnosis? Acute chest syndrome.
A sickle cell anemia patient has hematuria and inability to concentrate urine. Most likely renal pathology? Medullary ischemic injury with papillary necrosis and hyposthenuria.
A sickle cell anemia patient develops recurrent right upper abdominal pain and jaundice. Most likely pathology in gallbladder? Black pigment gallstones due to chronic hemolysis.
A peripheral smear shows sickled cells and Howell-Jolly bodies in a sickle cell anemia patient. What does this indicate? Functional hyposplenism/autosplenectomy.
A child with sickle cell anemia develops osteomyelitis. Most likely causative organism in exam questions? Salmonella species.
A sickle cell anemia patient has painful prolonged erection. Underlying pathology? Vaso-occlusive priapism due to venous outflow obstruction.
In a sickle cell anemia MCQ, absent HbA with predominant HbS on electrophoresis points to which genotype? HbSS (sickle cell anemia).
In sickle cell anemia, which crisis is most directly linked to tissue infarction pain episodes? Vaso-occlusive crisis.
In sickle cell anemia, what explains chronic jaundice in pathology terms? Persistent extravascular hemolysis leading to unconjugated hyperbilirubinemia.
In sickle cell anemia, what is the dominant type of hemolysis? Predominantly extravascular hemolysis (with variable intravascular component).
In sickle cell anemia, what membrane-level consequence follows repeated sickling cycles? Membrane injury with loss of deformability and formation of irreversibly sickled cells.
In sickle cell anemia, what is the significance of target cells on smear? Reflects altered membrane and splenic dysfunction; commonly seen in hemoglobinopathies with hyposplenism.
In sickle cell anemia, what pathologic process predisposes to pulmonary hypertension? Chronic hemolysis, endothelial dysfunction, and recurrent pulmonary vaso-occlusion.
In sickle cell anemia, what is the relation between acidosis and sickling? Acidosis promotes deoxygenated HbS state, increasing polymerization and sickling.
In sickle cell anemia, which genotype is usually clinically severe: HbSS or HbAS? HbSS is severe; HbAS is usually asymptomatic carrier state.
In sickle cell anemia, what is the pathology explanation for recurrent severe bacterial infections in childhood? Loss of splenic phagocytic/immune function from repeated splenic infarction.
In sickle cell anemia, what is the expected reticulocyte trend during steady-state disease? Elevated reticulocyte count due to chronic compensatory erythropoiesis.
In sickle cell anemia, what happens to RBC lifespan? Markedly reduced (typically around 10-20 days vs normal ~120 days).
In sickle cell anemia, what term describes crescent-shaped red cells? Drepanocytes.
In sickle cell anemia, what key event converts a vascular episode into end-organ fibrosis over time? Repeated ischemia-reperfusion injury with cumulative infarction and scarring.
In sickle cell anemia, what is the pathology behind growth retardation/delayed puberty in severe cases? Chronic anemia, high metabolic demand, and recurrent ischemic organ injury.
In sickle cell anemia, what finding on smear suggests active marrow compensation after hemolysis? Polychromasia (reticulocytosis).
In sickle cell anemia, what happens to the spleen size over natural course of HbSS disease? Early enlargement, later progressive shrinkage from autosplenectomy.
In sickle cell anemia, what is the diagnostic pathology principle behind HPLC/electrophoresis? Separation and quantification of hemoglobin fractions to identify HbS-dominant phenotype.
In sickle cell anemia, what is the NEET-PG pathology hallmark triad to remember? Hemolysis + vaso-occlusion + progressive end-organ infarction.
- A “super-high-yield only” 40-card version for rapid revision
- A tagged version (for example:
Genetics,Smear,Crisis,Organ pathology,Labs) for filtered practice in AnkiDroid.
Is the above high yeild?
What's High Yield ✅
- Molecular mutation (GAG→GTG, Glu→Val) — always asked
- Sickling triggers — frequently tested
- Autosplenectomy + consequences — classic NEET topic
- Salmonella osteomyelitis — repeat PYQ
- Parvovirus B19 → aplastic crisis — PYQ multiple times
- Dactylitis as earliest manifestation — PYQ
- Hair-on-end skull, H-shaped vertebrae — PYQ
- HbF protective role / Hydroxyurea — frequently asked
- Acute chest syndrome — high yield
- Pigment gallstones — PYQ
- Howell-Jolly bodies + autosplenectomy — PYQ
- Hemoglobin electrophoresis as gold standard — PYQ
What's Missing or Weak ❌
| Gap | Why it matters |
|---|---|
| HbF % in newborns — why SCA presents after 6 months | Classic NEET concept |
| Sickle cell TRAIT specific pathology (hematuria, no anemia, renal) | Frequently confused in MCQs |
| Sequestration crisis — which organ in adults vs children | Spleen (children) vs Liver (adults) — tested |
| Most common cause of death: children vs adults | Pneumococcal sepsis vs Acute Chest Syndrome |
| Heterozygous advantage (malaria protection) mechanism | Asked conceptually |
| Hydroxyurea mechanism of action at molecular level | Beyond just "↑HbF" |
| Newborn screening method | HPLC — asked |
| Sickle cell + pregnancy complications | Occasionally tested |
| Which crisis has splenomegaly as a feature | Sequestration — differentiates from aplastic |
| Etiologies within Acute Chest Syndrome | Fat embolism vs infection distinction |
| Iron overload / hemosiderosis from transfusions | Long-term pathology complication |
| Cerebrovascular: children ischemic, adults hemorrhagic | High yield distinction |
| Renal: which specific zone of kidney is most susceptible | Medulla (hypertonic, hypoxic) — conceptual |
What's Low Yield / Filler (could be removed) 🔻
- "What is the central pathological event" (too vague, not MCQ-style)
- "What does chronic jaundice reflect in pathology terms" (redundant with bilirubin card)
- "What is meant by functional asplenia" (definition card — not MCQ-worthy)
- "What is the dominant type of hemolysis" (rarely asked at this depth)
- A few cards on reticulocytosis and polychromasia are slightly repetitive
Verdict
Okay give high yield cards
In sickle cell anemia, what is the point mutation in β-globin gene? GAG → GTG at codon 6 of HBB gene.
In sickle cell anemia, which amino acid substitution occurs in β-globin chain? Glutamic acid is replaced by valine at position 6 (Glu6Val).
In sickle cell anemia, what is the inheritance pattern? Autosomal recessive.
In sickle cell anemia, which abnormal hemoglobin is produced? HbS (alpha2 betaS2).
In sickle cell anemia, what initiates RBC sickling at molecular level? Polymerization of deoxygenated HbS.
In sickle cell anemia, which condition most strongly promotes sickling? Deoxygenation (hypoxia).
In sickle cell anemia, how does acidosis affect sickling? It increases deoxygenated HbS and promotes polymerization.
In sickle cell anemia, what is the effect of RBC dehydration on sickling? It increases intracellular HbS concentration and accelerates sickling.
In sickle cell anemia, what is the central pathology causing painful crises and organ injury? Microvascular vaso-occlusion by rigid sickled RBCs.
In sickle cell anemia, what are the two major mechanisms of disease pathology? Chronic hemolysis and recurrent vaso-occlusion.
In sickle cell anemia, what is the hallmark peripheral smear finding? Sickle-shaped RBCs (drepanocytes).
In sickle cell anemia, which smear finding indicates functional asplenia? Howell-Jolly bodies.
In sickle cell anemia, which additional smear finding is commonly seen with hyposplenism? Target cells.
In sickle cell anemia, what is the most common crisis type? Vaso-occlusive (painful) crisis.
In sickle cell anemia, what is the cause of aplastic crisis? Parvovirus B19 infection suppressing erythropoiesis.
In sickle cell anemia, what is the key lab clue for aplastic crisis? Low reticulocyte count with sudden anemia.
In sickle cell anemia, what defines sequestration crisis pathologically? Acute pooling of blood in spleen (especially children), causing shock and severe anemia.
In sickle cell anemia, which crisis classically presents with acute splenomegaly in a child? Splenic sequestration crisis.
In sickle cell anemia, what is the earliest clinical manifestation in infants? Dactylitis (hand-foot syndrome).
In sickle cell anemia, why does disease usually manifest after 6 months of age? Decline of protective fetal hemoglobin (HbF) after infancy.
In sickle cell anemia, what is the effect of HbF on pathogenesis? HbF inhibits HbS polymerization and reduces sickling.
In sickle cell anemia, which drug is high yield for reducing crises by increasing HbF? Hydroxyurea.
In sickle cell anemia, what is the most common organism causing osteomyelitis? Salmonella species.
In sickle cell anemia, what is the most common cause of death in children? Overwhelming pneumococcal sepsis.
In sickle cell anemia, what is the most common cause of death in adults? Acute chest syndrome.
In sickle cell anemia, what is acute chest syndrome? New pulmonary infiltrate with fever/respiratory symptoms due to vaso-occlusion plus or minus infection/fat embolism.
In sickle cell anemia, what is the natural splenic progression? Early splenomegaly followed by repeated infarction leading to autosplenectomy.
In sickle cell anemia, what is autosplenectomy? Progressive fibrosis and shrinkage of spleen due to repeated infarcts.
In sickle cell anemia, deficiency of splenic function increases risk of infection by which group? Encapsulated organisms (especially Streptococcus pneumoniae).
In sickle cell anemia, what renal defect appears early due to medullary ischemia? Hyposthenuria (impaired urine concentrating ability).
In sickle cell anemia, what classic renal structural lesion causes hematuria? Renal papillary necrosis.
In sickle cell anemia, what gallbladder pathology is common due to chronic hemolysis? Black pigment gallstones.
In sickle cell anemia, what causes priapism? Vaso-occlusion of penile vasculature.
In sickle cell anemia, what bone complication causes chronic hip pain in young adults? Avascular necrosis of femoral head.
In sickle cell anemia, what skull X-ray finding occurs due to marrow hyperplasia? Hair-on-end (crew-cut) appearance.
In sickle cell anemia, what vertebral X-ray sign is classically seen? H-shaped (fish-mouth) vertebra.
In sickle cell anemia, what is the best confirmatory test for diagnosis and hemoglobin fractionation? Hemoglobin electrophoresis (or HPLC quantification).
In sickle cell anemia, what is the electrophoresis hallmark of HbSS disease? Predominant HbS with absent HbA.
In sickle cell anemia, can solubility/sickling tests differentiate trait from disease? No, they detect HbS presence but do not reliably distinguish trait from disease.
In sickle cell anemia, what are expected hemolysis markers in labs? High indirect bilirubin, high LDH, low haptoglobin, reticulocytosis.
In sickle cell anemia, what is the typical baseline hemoglobin range in HbSS? About 6-9 g/dL.
In sickle cell anemia, stroke in children is usually what type? Ischemic stroke.
In sickle cell anemia, stroke in adults is relatively more likely to be what type? Hemorrhagic stroke.
In sickle cell trait, what key hematologic difference from sickle cell anemia is expected? Usually no chronic hemolytic anemia.
In sickle cell trait, what classic renal manifestation can still occur? Painless hematuria due to medullary sickling.
A 9-month-old with sickle cell disease has painful swelling of both hands and feet. Most likely diagnosis? Dactylitis from vaso-occlusion.
A child with sickle cell disease presents with sudden pallor, fatigue, very low reticulocyte count after viral fever. Most likely crisis? Aplastic crisis (Parvovirus B19).
A child with sickle cell disease presents with enlarged spleen, hypotension, and abrupt Hb fall. Most likely crisis? Splenic sequestration crisis.
A sickle cell patient presents with chest pain, fever, hypoxia, and new lung infiltrate. Most likely diagnosis? Acute chest syndrome.
A sickle cell patient with recurrent transfusions develops organ iron deposition. What pathology complication is this? Secondary hemosiderosis (transfusional iron overload).
A peripheral smear shows sickled RBCs, target cells, and Howell-Jolly bodies. Most likely underlying process? Sickle cell disease with functional asplenia.
In sickle cell anemia, what is the NEET-PG pathology triad to remember? Hemolysis, vaso-occlusion, end-organ ischemic infarction.
Does above cover everything that can be asked from pathology of sca, and will it prime me to answer clinical mcq in neet pg?
What's Still Missing
1. Robbins-Specific Pathology (Direct Source for NEET PG Pathology)
| Missing Concept | Why It's High Yield |
|---|---|
| SCA is classified under which category of anemia | Hemolytic anemia due to intracorpuscular defect — PYQ concept |
| Extravascular vs intravascular hemolysis proportion | Robbins specifically discusses this |
| Congo red staining / amyloidosis as long term complication | Chronic inflammatory state |
| Erythrophagocytosis in spleen/RES | Morphologic pathology concept |
| Endothelial activation — VCAM-1, P-selectin role | Vascular pathology mechanism |
2. Crisis Differentiation (Clinical MCQ Traps)
| Missing Concept | Why It's High Yield |
|---|---|
| Aplastic vs sequestration — reticulocyte differentiator | Classic NEET MCQ trap |
| Hemolytic crisis vs vaso-occlusive — how to distinguish | Frequently confused |
| Which crisis has NO splenomegaly | Aplastic — tricky negative |
3. Organ Pathology Depth
| Missing Concept | Why It's High Yield |
|---|---|
| Liver — hepatic sequestration crisis in adults | Adult equivalent of splenic sequestration |
| Bone marrow — extramedullary hematopoiesis sites | Spleen, liver, lymph nodes |
| Lung — fat embolism from bone marrow infarction mechanism | Cause within ACS |
| Eye — sea fan neovascularization; worse in HbSC | Specific finding tested |
| Kidney — which zone is most vulnerable and why | Medulla — hypertonic + hypoxic = sickling |
4. Comparative/Variant Questions (Highest MCQ Trap Zone)
| Missing Concept | Why It's High Yield |
|---|---|
| HbSC vs HbSS severity comparison | HbSC = milder overall but worse retinopathy |
| HbS-β⁰ thal vs HbSS — clinically similar, no HbA | Electrophoresis distinction |
| HbS-β⁺ thal vs HbSS — some HbA present | Electrophoresis distinction |
| Sickle cell trait — protective against malaria; which species | P. falciparum specifically |
5. Specific PYQ Concepts Not Yet Covered
| Missing Concept | Why It's High Yield |
|---|---|
| Most common presentation/chief complaint of SCA | Painful (vaso-occlusive) crisis |
| Which infection is most common overall (not just osteo) | Pneumococcal (most common overall) |
| Hydroxyurea — additional mechanisms beyond HbF | ↓Neutrophil count, ↓RBC adhesion |
| Newborn screening — best method | HPLC |
| Megaloblastic crisis — cause | Folate depletion from high RBC turnover |
| Why SCA protects against malaria — mechanism | Sickled cells phagocytosed before parasite matures |
| Sequestration — in adults which organ takes over from spleen | Liver |
6. Clinical Scenario Gaps
| Scenario Not Covered | Trap |
|---|---|
| Patient with SCA + bilateral hip pain + young adult | AVN — students confuse with painful crisis |
| SCA patient, smear shows ONLY target cells and no sickle cells | Suggests HbSC not HbSS |
| Patient with sickle trait, hematuria, normal CBC | Papillary necrosis in trait |
| SCA child + meningitis — most likely organism | S. pneumoniae |
| SCA patient, Hb suddenly drops but reticulocytes HIGH | Hemolytic crisis — not aplastic |
Verdict
Yes complete final deck, 100 percent coverage of neet pg
In sickle cell anemia, what is the fundamental genetic defect? Point mutation in beta-globin gene (HBB).
In sickle cell anemia, what codon change occurs in HBB gene? Codon 6 changes from GAG to GTG.
In sickle cell anemia, which amino acid substitution occurs in beta-globin chain? Glutamic acid is replaced by valine at position 6 (Glu6Val).
In sickle cell anemia, what type of mutation is the beta-globin defect? Missense point mutation.
In sickle cell anemia, what is the inheritance pattern? Autosomal recessive.
In sickle cell anemia, what is the hemoglobin composition of HbS? Alpha2 betaS2.
In sickle cell anemia, what initiates RBC sickling at molecular level? Polymerization of deoxygenated HbS.
In sickle cell anemia, why does valine substitution promote polymerization? Valine creates a hydrophobic patch causing intermolecular aggregation in deoxygenated state.
In sickle cell anemia, which physiological state most strongly triggers sickling? Hypoxia (deoxygenation).
In sickle cell anemia, how does acidosis influence sickling? Acidosis enhances deoxygenated HbS and increases polymerization.
In sickle cell anemia, how does dehydration worsen disease? It raises intracellular HbS concentration, increasing polymer formation.
In sickle cell anemia, what is the sequence: deoxygenation -> ? -> sickling? Deoxygenation -> HbS polymerization -> RBC distortion (sickling).
In sickle cell anemia, are early sickling episodes reversible? Yes, early sickling can reverse on reoxygenation.
In sickle cell anemia, what causes irreversible sickled cells to develop? Repeated sickling-unsickling cycles causing membrane damage.
In sickle cell anemia, what is the core pathologic triad? Hemolysis, vaso-occlusion, and ischemic end-organ damage.
In sickle cell anemia, what is the dominant vascular pathology behind pain crises? Microvascular occlusion by rigid sickled erythrocytes.
In sickle cell anemia, what endothelial process amplifies vaso-occlusion? Endothelial activation with increased adhesion molecule expression.
In sickle cell anemia, what is the pathology basis for chronic inflammation? Ongoing hemolysis and ischemia-reperfusion injury causing endothelial dysfunction.
In sickle cell anemia, what is the major mechanism of anemia? Chronic hemolysis due to reduced RBC lifespan.
In sickle cell anemia, what happens to RBC lifespan? It is markedly shortened to about 10-20 days.
In sickle cell anemia, what is the predominant type of hemolysis? Predominantly extravascular hemolysis.
In sickle cell anemia, what are classic peripheral smear findings? Sickle cells, target cells, anisopoikilocytosis, polychromasia, nucleated RBCs.
In sickle cell anemia, what is the name for sickle-shaped RBCs? Drepanocytes.
In sickle cell anemia, what does polychromasia on smear indicate? Reticulocytosis from compensatory marrow response.
In sickle cell anemia, why are nucleated RBCs seen in peripheral blood? Intense marrow stress with accelerated erythropoiesis.
In sickle cell anemia, what does Howell-Jolly body presence indicate? Functional hyposplenism/autosplenectomy.
In sickle cell anemia, why are target cells frequent? Membrane abnormalities and reduced splenic clearance.
In sickle cell anemia, what marrow pathology develops due to chronic hemolysis? Erythroid hyperplasia.
In sickle cell anemia, what skull radiologic sign reflects marrow hyperplasia? Hair-on-end (crew-cut) appearance.
In sickle cell anemia, what vertebral sign is classically described? H-shaped (fish-mouth/Lincoln log) vertebrae.
In sickle cell anemia, what is the earliest splenic change in childhood? Congestive splenomegaly from RBC trapping.
In sickle cell anemia, what is autosplenectomy? Progressive fibrotic shrinkage of spleen after repeated infarctions.
In sickle cell anemia, what functional consequence follows autosplenectomy? Functional asplenia with severe risk of encapsulated bacterial infections.
In sickle cell anemia, which organisms are classically problematic after autosplenectomy? Encapsulated organisms, especially Streptococcus pneumoniae.
In sickle cell anemia, what is the most common cause of death in children? Overwhelming pneumococcal sepsis.
In sickle cell anemia, what is the most common cause of death in adults? Acute chest syndrome.
In sickle cell anemia, what is the most common crisis type? Vaso-occlusive crisis.
In sickle cell anemia, what causes vaso-occlusive crisis pain? Ischemic tissue infarction from microvascular obstruction.
In sickle cell anemia, what causes aplastic crisis? Parvovirus B19 suppression of erythroid precursors.
In sickle cell anemia, what key lab clue supports aplastic crisis? Low reticulocyte count with abrupt hemoglobin fall.
In sickle cell anemia, what defines sequestration crisis? Acute pooling of blood in spleen (or liver), causing severe anemia and hypovolemia.
In sickle cell anemia, in which age group is splenic sequestration most typical? Children.
In sickle cell anemia, which organ can show sequestration more often in adults? Liver (hepatic sequestration).
In sickle cell anemia, which crisis usually presents with enlarged spleen and shock? Sequestration crisis.
In sickle cell anemia, which crisis typically does NOT have splenomegaly and has low reticulocytes? Aplastic crisis.
In sickle cell anemia, what is hemolytic crisis? Acute acceleration of hemolysis causing sudden Hb drop with high reticulocyte count.
In sickle cell anemia, what causes megaloblastic crisis? Folate deficiency due to high erythropoietic turnover.
In sickle cell anemia, what is the earliest typical clinical manifestation in infancy? Dactylitis (hand-foot syndrome).
In sickle cell anemia, what is the pathology basis of dactylitis? Vaso-occlusion in small bones of hands/feet.
In sickle cell anemia, why symptoms usually begin after 6 months of age? Protective fetal hemoglobin declines after infancy.
In sickle cell anemia, how does HbF alter pathology? It inhibits HbS polymerization and decreases sickling.
In sickle cell anemia, what is hydroxyurea's high-yield pathology benefit? Increases HbF and reduces vaso-occlusive events.
In sickle cell anemia, what additional anti-vaso-occlusive effect of hydroxyurea is tested? Reduces leukocyte-mediated endothelial adhesion.
In sickle cell anemia, what pulmonary complication presents with fever, chest pain, hypoxia, and new infiltrate? Acute chest syndrome.
In sickle cell anemia, what are major pathogenic contributors to acute chest syndrome? Pulmonary vaso-occlusion, infection, and fat embolism from marrow infarcts.
In sickle cell anemia, what chronic pulmonary vascular complication can occur? Pulmonary hypertension.
In sickle cell anemia, what kidney region is most vulnerable to sickling injury? Renal medulla (hypoxic, acidic, hypertonic environment).
In sickle cell anemia, what is the earliest renal functional defect? Hyposthenuria (inability to concentrate urine).
In sickle cell anemia, what structural renal lesion causes hematuria? Papillary necrosis.
In sickle cell anemia, what long-term renal outcome can develop? Chronic kidney disease (sickle nephropathy).
In sickle cell anemia, what is the common hepatobiliary pathology due to chronic hemolysis? Black pigment gallstones.
In sickle cell anemia, what explains chronic unconjugated hyperbilirubinemia? Ongoing hemolysis.
In sickle cell anemia, what bone complication causes chronic groin pain in young adults? Avascular necrosis of femoral head.
In sickle cell anemia, which pathogen is classically associated with osteomyelitis? Salmonella species.
In sickle cell anemia, what eye lesion is classically tested in proliferative retinopathy? Sea-fan neovascularization.
In sickle cell anemia, which genotype is especially associated with severe retinopathy? HbSC disease.
In sickle cell anemia, what causes priapism pathologically? Veno-occlusion in penile vasculature.
In sickle cell anemia, what causes chronic leg ulcers? Chronic microvascular ischemia.
In sickle cell anemia, what major CNS complication occurs in children? Ischemic stroke.
In sickle cell anemia, what CNS stroke type is relatively more common in adults? Hemorrhagic stroke.
In sickle cell anemia, what CBC pattern is common in baseline disease? Normocytic hemolytic anemia with reticulocytosis.
In sickle cell anemia, what is a typical baseline hemoglobin range in HbSS? About 6-9 g/dL.
In sickle cell anemia, what hemolysis biomarkers are classically elevated? Indirect bilirubin and LDH.
In sickle cell anemia, what hemolysis biomarker is classically decreased? Haptoglobin.
In sickle cell anemia, what is the role of sickling/solubility tests? Screening for HbS presence only.
In sickle cell anemia, why are solubility tests insufficient for final diagnosis? They cannot reliably distinguish trait from disease.
In sickle cell anemia, what is the confirmatory diagnostic approach for hemoglobin fractionation? Hemoglobin electrophoresis or HPLC.
In sickle cell anemia, what electrophoresis pattern defines HbSS? Predominant HbS with absent HbA.
In sickle cell anemia, what newborn screening method is high yield? HPLC-based hemoglobin analysis.
In sickle cell anemia, what is expected for HbA in homozygous disease? HbA absent.
In sickle cell trait, what is the usual clinical hematology profile? Usually no chronic hemolytic anemia.
In sickle cell trait, what renal manifestation is classically testable? Painless hematuria from papillary necrosis.
In sickle cell trait, what infection-related evolutionary advantage is classically asked? Protection against severe Plasmodium falciparum malaria.
In sickle cell anemia, which genotype is generally most severe: HbSS or HbSC? HbSS is generally more severe.
In sickle cell anemia, how does HbSC compare with HbSS in painful crises and retinopathy? Usually milder anemia/pain than HbSS but relatively more proliferative retinopathy.
In sickle cell anemia, what distinguishes HbS-beta0 thalassemia on electrophoresis? No HbA, resembles severe HbSS phenotype.
In sickle cell anemia, what distinguishes HbS-beta+ thalassemia on electrophoresis? Some HbA is present, usually milder phenotype than HbSS.
In sickle cell anemia, what is the pathology basis of growth delay? Chronic anemia plus recurrent ischemic injury and high metabolic demand.
In sickle cell anemia, what transfusion-related pathology complication is important for exams? Secondary iron overload (hemosiderosis).
In sickle cell anemia, where can extramedullary hematopoiesis occur? Liver and spleen (and other reticuloendothelial sites).
A 10-month-old child with sickle cell disease has painful swollen fingers and toes. Most likely diagnosis? Dactylitis due to vaso-occlusion.
A child with sickle cell disease has sudden pallor and severe anemia with very low reticulocyte count after febrile illness. Most likely crisis? Aplastic crisis due to Parvovirus B19.
A child with sickle cell disease has sudden abdominal distension, splenomegaly, hypotension, and rapid Hb fall. Most likely diagnosis? Splenic sequestration crisis.
A sickle cell disease patient has severe bone pain, high reticulocyte count, and no splenomegaly. Most likely crisis type? Vaso-occlusive crisis.
A sickle cell disease patient has acute Hb fall with jaundice and high reticulocyte count. Most likely crisis? Hemolytic crisis.
A sickle cell disease patient presents with fever, chest pain, tachypnea, and new lung infiltrate. Most likely diagnosis? Acute chest syndrome.
A young adult with sickle cell disease has persistent groin pain with limited hip movement between crises. Most likely pathology? Avascular necrosis of femoral head.
A sickle cell patient with recurrent transfusions develops endocrine and cardiac iron deposition. Most likely complication? Transfusional hemosiderosis.
A peripheral smear shows sickled cells with Howell-Jolly bodies in a teenager with recurrent infections. Underlying pathology? Functional asplenia from autosplenectomy.
A patient with sickle cell disease develops osteomyelitis of femur. Most likely organism in exam context? Salmonella.
A sickle cell disease patient has recurrent hematuria and poor urine concentrating ability. Most likely renal pathology? Medullary ischemic injury with papillary necrosis and hyposthenuria.
A sickle cell disease patient develops prolonged painful penile erection. Most likely mechanism? Veno-occlusive priapism.
A child with sickle cell disease develops sudden focal neurological deficit. Most likely vascular event? Ischemic stroke.
A sickle cell disease patient has chronic jaundice and gallbladder stones. Stone type most likely? Black pigment stones.
A patient has positive sickling test but no anemia and normal routine CBC. Most likely diagnosis? Sickle cell trait.
A patient has predominant HbS with absent HbA on electrophoresis. Most likely diagnosis? HbSS sickle cell anemia.
A patient has HbS plus significant HbC with milder anemia but retinal complications. Most likely genotype? HbSC disease.
A child with recurrent painful crises has improved frequency after therapy that raises HbF. Drug most likely used? Hydroxyurea.
In sickle cell anemia, what single pathology concept best explains multi-organ chronic damage? Repeated vaso-occlusion causing cumulative ischemia, infarction, and fibrosis.