Wry neck
Reading File
Finding Sources
Searching the Web
wry neck torticollis types causes treatment clinical
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a full clinical overview:
Wry Neck (Torticollis)
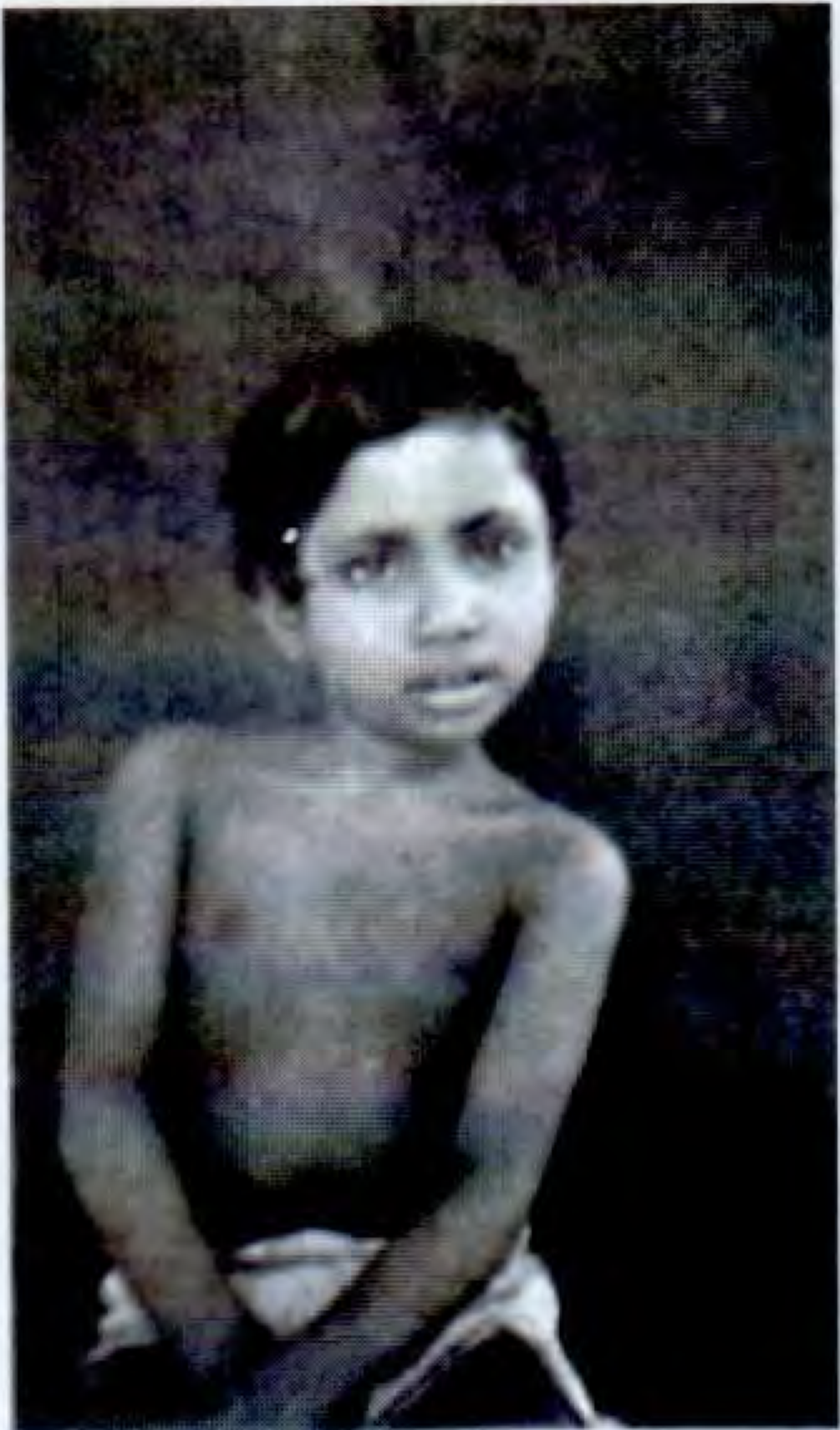
Clinical appearance of torticollis - S Das Manual on Clinical Surgery
Definition
Torticollis (wry neck) is a deformity in which the head is bent to one side while the chin points to the other side. The key biomechanics: the head tilts toward and rotates away from the tight sternocleidomastoid (SCM) muscle. In long-standing cases, there is facial atrophy on the affected side - the distance from the outer canthus of the eye to the angle of the mouth is smaller, the eyebrow is less arched, the nose somewhat flattened, and the cheek less full.
Classification / Varieties
S Das Manual on Clinical Surgery lists the main varieties:
| Type | Key Features |
|---|---|
| (a) Congenital | History of difficult labour; sternomastoid "tumour" (fibrotic nodule); affected muscle feels firm and rigid |
| (b) Traumatic | Fracture-dislocation of the cervical spine |
| (c) Rheumatic | Sudden appearance after exposure to cold or draught |
| (d) Inflammatory | E.g. from inflamed cervical lymph nodes (Grisel syndrome) |
| (e) Spasmodic | SCM of affected side + posterior cervical muscles of opposite side in sustained spasm; a form of cervical dystonia |
| (f) Compensatory | E.g. from scoliosis, or defect in sight (ocular torticollis) |
| (g) Pott's disease | Tuberculosis of the cervical spine |
| (h) Contracture | After burns, ulcers, skin scarring |
Congenital Muscular Torticollis (CMT)
This is by far the most common type.
Pathogenesis
Proposed causes (Campbell's Operative Orthopaedics 2026):
- Malposition of the fetus in utero / intrauterine constraint
- Intrauterine or perinatal compartment syndrome of the SCM (Davids, Wenger, Mubarak hypothesis)
- Birth trauma, vascular injury, infection
The result is fibrosis and contracture of the SCM muscle, sometimes with a palpable fibrotic nodule ("sternomastoid pseudotumour"), which typically appears in the first 6 weeks of life. It is associated with congenital hip dysplasia in up to 20% of cases and with breech positioning.
Diagnosis
- Clinical: ipsilateral head tilt + contralateral chin rotation
- The palpable fibrotic nodule within the SCM typically confirms the diagnosis without further imaging
- When diagnosis is in doubt or neurologic findings exist: cervical spine X-rays, or MRI/CT
- Ultrasonography is useful to evaluate SCM thickness (>5 cm correlates with poorer response to stretching) and to predict which infants will need surgery
- Facial asymmetry (plagiocephaly) develops if untreated; the frontooccipital skull diameter may decrease
Treatment
Nonoperative (first-line):
- Stretching exercises - ideally started before 3-4 months of age
- Results: 92-100% achieve full passive neck rotation; only 1% require surgery if treated this early
- For every month treatment is delayed, the chance of surgery increases
- If CMT persists beyond the first year, nonoperative treatment is rarely successful
- Botulinum toxin type A injection combined with physical therapy may improve outcomes in resistant cases
- A cervical orthosis may supplement stretching
Operative:
- Indicated when stretching fails, deformity is established, or limitation of motion exceeds 30 degrees
- Ideal age: 4-5 years; permanent deformity is prevented by operating in early childhood
- Unipolar release: division of the distal (clavicular/sternal) attachment - appropriate for mild deformity
- Bipolar release: release at both proximal and distal ends - for moderate/severe torticollis
- Endoscopic release has been described (precise division, minimal scarring) but no large series reported
- Outcome measured by the Cheng and Tang Scoring System; most patients show marked improvement in neck motion, head tilt, and cosmesis
Spasmodic Torticollis (Idiopathic Cervical Dystonia)
This is a neurological form affecting adults, described in detail in Adams and Victor's Principles of Neurology (12th ed):
- Most frequent form of restricted focal dystonia
- Onset: early to middle adult life; more common in women (peak in 5th decade)
- Begins as subtle tilting/turning of the head, worsens slowly
- Muscles: SCM is most prominently affected; also levator scapulae and trapezius; posterior cervical muscles on both sides
- Characteristic "sensory tricks" (gestes antagonistes): placing a hand on the chin or neck, counterpressure on the side of deviation, or contact with the back of a chair reduces the spasm - these become less effective as disease progresses
- Spasms worsen on standing/walking; reduced when lying down
- ~15% have oral/mandibular/hand dystonia; ~10% have blepharospasm
- No neuropathologic changes found at autopsy
Treatment of Spasmodic Torticollis
- Botulinum toxin (first-line): Periodic injections (every 3-6 months) into affected muscles; ~90% achieve some relief. Best guided by palpation + EMG. Adverse effects: excessive weakness, local pain, dysphagia (transient). 5-10% develop neutralizing antibodies and become resistant.
- Trihexyphenidyl / benztropine: Anticholinergics may give some relief but are poorly tolerated in high doses.
- Deep brain stimulation (DBS): For cases refractory to medications and botulinum toxin. Targets: globus pallidus internus (GPi) or subthalamic nucleus. Preferable to older ablative procedures.
- Surgical (severe/refractory): Combined sectioning of the spinal accessory nerve + first three cervical motor roots bilaterally - relief in one-third to one-half of cases for up to 6 years.
Acquired Torticollis - Key Causes to Remember
Bailey and Love's Surgery summarises: acquired torticollis may be caused by:
- Inflammation/infection (e.g. retropharyngeal abscess, cervical lymphadenitis - Grisel syndrome)
- Ocular problems (ocular torticollis - compensatory head tilt for diplopia or nystagmus)
- Atlantoaxial rotatory subluxation - must be considered in any child with traumatic torticollis; differentiated from muscular torticollis by history, time course, and imaging
- Posterior fossa tumour - a red-flag cause; must be excluded especially in children
- Paroxysmal torticollis (episodic, associated with migraine in children)
Summary
| Feature | Congenital (CMT) | Spasmodic (Cervical Dystonia) |
|---|---|---|
| Age | Infants | Adults (peak 5th decade) |
| Cause | SCM fibrosis/contracture | Focal dystonia (basal ganglia) |
| Onset | Birth / first weeks | Gradual in adulthood |
| SCM | Firm, fibrotic nodule | Hypertrophied, in spasm |
| Facial changes | Plagiocephaly if untreated | None |
| First-line Rx | Stretching exercises | Botulinum toxin |
| Surgery | SCM release (age 4-5 yr) | DBS / nerve sectioning |
- S Das Manual on Clinical Surgery, 13th Ed, p. 377-378
- Bailey and Love's Short Practice of Surgery, 28th Ed
- Campbell's Operative Orthopaedics, 15th Ed 2026, Chapter 33
- Adams and Victor's Principles of Neurology, 12th Ed, p. 110-111
This is a shared conversation. Sign in to Orris to start your own chat.