Flurosis 5 mark
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Here is a complete 5-mark answer on Fluorosis:
Fluorosis
Definition
Fluorosis is a chronic condition resulting from prolonged ingestion of excessive amounts of fluoride. It is endemic in areas where drinking water naturally contains high fluoride levels (>1.5 mg/L), and is a major public health problem in parts of India (Andhra Pradesh, Punjab, Haryana, Karnataka, Kerala, Tamil Nadu) and other regions worldwide.
Etiology / Cause
- Primary source: drinking water with fluoride concentration >1.5 mg/L (dental fluorosis) or 3-6 mg/L (skeletal fluorosis)
- At concentrations exceeding 10 mg/L, crippling fluorosis can occur
- Dietary factors: diets based on sorghum (jowar) promote higher retention of ingested fluoride compared to rice-based diets
Types / Clinical Manifestations
(a) Dental Fluorosis
- Occurs when excess fluoride is ingested during tooth calcification (first 7 years of life)
- Characterized by mottling of dental enamel (reported at levels >1.5 mg/L)
- Early sign: teeth lose their shiny appearance; chalk-white patches develop
- Progression: white patches become yellow, then brown or black
- Severe cases: loss of enamel gives a corroded appearance
- Most visible on the incisors of the upper jaw
- Almost entirely confined to permanent teeth and develops only during tooth formation
(b) Skeletal Fluorosis
- Associated with lifetime daily intake of 3.0-6.0 mg/L or more
- Heavy fluoride deposition in the skeleton
- Radiological features:
- Osteosclerosis (particularly axial skeleton)
- Enthesopathy with ossification of ligaments
- Large spinal osteophytes and paraspinal ossification
- Periosteal proliferation and degenerative changes
- Paraspinal ossification may cause compression myelopathy
- Leads to permanent disability at high concentrations (>10 mg/L)
(c) Genu Valgum (Endemic Fluorosis variant)
- Characterized by genu valgum and osteoporosis of lower limbs
- Reported in Andhra Pradesh and Tamil Nadu
- Observed among people whose staple diet was sorghum (jowar)
Prevention / Control
- Change water source: Find a new source with lower fluoride content (0.5-0.8 mg/L); surface water has lower fluoride than groundwater
- Chemical defluoridation - Nalgonda Technique (developed by NEERI, Nagpur): Addition of lime and alum in sequence, followed by flocculation, sedimentation, and filtration
- Avoid fluoride supplements in children drinking fluoridated water
- Fluoride toothpaste is NOT recommended in endemic areas for children up to 6 years of age
National Programme for Prevention and Control of Fluorosis (NPPCF)
- Essential services: Referral services and IEC (Information, Education, Communication) activities in fluorosis-endemic districts
- Desirable: Clinical examination and diagnostic assessment for fluorosis cases, monitoring of community-level surveillance
Sources:
- Park's Textbook of Preventive and Social Medicine, pp. 740
- Grainger & Allison's Diagnostic Radiology
Nutritional anemias
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent - I now have comprehensive content from authoritative textbooks. Here is the full answer:
Nutritional Anemias
Nutritional anemias are anemias that result from a deficiency of one or more nutrients essential for red blood cell production - primarily iron, vitamin B12, and folate. Each produces a characteristic blood picture that provides a diagnostic clue to the underlying deficiency.
Classification
| Type | Deficiency | Blood Picture |
|---|---|---|
| Iron Deficiency Anemia | Iron | Microcytic, hypochromic |
| Megaloblastic Anemia | Vitamin B12 / Folate | Macrocytic, normochromic |
| Pernicious Anemia | Vitamin B12 (intrinsic factor) | Macrocytic + neurological |
1. Iron Deficiency Anemia (IDA)
Prevalence
Iron deficiency is the most common nutritional deficiency in the world - affecting ~10% in high-resource countries and 25-50% in low-resource countries.
Causes
- Chronic blood loss - most important cause in high-resource countries (GI bleeds from peptic ulcers, colon cancer, hemorrhoids; menorrhagia)
- Low dietary intake / poor bioavailability - most common in low-resource countries (vegetarian diets); also seen in infants fed exclusively milk, elderly
- Increased demand - pregnancy, infancy
- Malabsorption - celiac disease, gastritis, post-gastrectomy
Iron Metabolism Basis
- Normal body iron: ~2.5 g (women), 3.5 g (men); 80% in hemoglobin/myoglobin/enzymes
- Regulated by hepcidin (liver peptide) - negatively regulates ferroportin, controlling iron export from enterocytes
- Serum ferritin = best surrogate of iron stores
- In deficiency: stores depleted first → serum iron falls → transferrin rises → microcytic anemia develops
Pathogenesis of Microcytosis
Lack of iron → decreased heme synthesis → decreased hemoglobin → maturing red cells continue dividing past their normal stopping point → small, pale (microcytic, hypochromic) red cells
Clinical Features
- Often mild and asymptomatic
- Weakness, listlessness, pallor
- Long-standing anemia: koilonychia (spoon-shaped nails), nail thinning/flattening
- Pica (compulsion to eat non-food substances such as dirt or clay) - characteristic neurobehavioral complication
Laboratory Findings
- Decreased hematocrit, MCV, MCH
- Low serum ferritin and serum iron
- Elevated total iron-binding capacity (TIBC)
- Low transferrin saturation
- Thrombocytosis (platelet count often elevated)
- Elevated erythropoietin
2. Megaloblastic Anemia (Vitamin B12 / Folate Deficiency)
Mechanism (Common to Both)
The central defect is impaired DNA synthesis due to deficiency of folate or B12, both required as cofactors for thymidine (dTMP) synthesis. DNA replication and nuclear division do not keep pace with cytoplasmic maturation, leading to:
- Nuclear-cytoplasmic asynchrony
- Abnormally large erythroid precursors (megaloblasts)
- Ineffective hematopoiesis and pancytopenia
Morphology (Blood Smear)
- Macro-ovalocytes (large, oval red cells) - highly characteristic
- Hypersegmented neutrophils (5+ lobes instead of normal 3-4)
- Anisocytosis and poikilocytosis
- Low reticulocyte count
- Bone marrow: hypercellular with megaloblastic changes at all erythroid stages, giant metamyelocytes, abnormal megakaryocytes
(A) Vitamin B12 Deficiency - Pernicious Anemia
Sources: Animal products (meat, fish, milk, eggs); daily requirement 2-3 μg; body stores last several years.
Absorption Pathway:
- B12 released from food by pepsin → binds salivary haptocorrin
- In duodenum, released from haptocorrin by pancreatic proteases → binds intrinsic factor (IF) secreted by gastric parietal cells
- B12-IF complex → binds cubilin receptor on ileal epithelial cells → endocytosed
- Released into plasma bound to transcobalamin II → delivered to liver and bone marrow
Causes of B12 Deficiency:
- Decreased intake: strict vegetarianism / vegan diet
- Pernicious anemia (most important): autoimmune gastritis destroys parietal cells → no intrinsic factor
- Gastrectomy, ileal resection, ileitis
- Fish tapeworm (Diphyllobothrium latum) - competitive uptake
- Bacterial overgrowth in blind loops
Biochemical Role:
- B12 (as methylcobalamin) converts homocysteine to methionine via methionine synthase
- In doing so, it liberates FH4 (tetrahydrofolate) from its "trapped" form (N5-methyl FH4)
- FH4 is required for dUMP → dTMP (DNA synthesis)
- B12 deficiency thus causes a functional folate deficiency
Neurological Complications (Subacute Combined Degeneration):
- B12 also required for methylmalonyl-CoA → succinyl-CoA (via adenosylcobalamin)
- Deficiency leads to elevated methylmalonic acid → demyelination of posterior and lateral columns of spinal cord
- Not improved by folate (unlike the anemia)
(B) Folate Deficiency Anemia
Causes:
- Inadequate dietary intake (most common) - poor diet, alcoholism, infancy
- Increased requirement: pregnancy, infancy, hemolytic anemias, disseminated cancer
- Malabsorption: celiac disease, tropical sprue
- Drugs: anticonvulsants (phenytoin), oral contraceptives, methotrexate (folate antagonist)
- Increased loss: hemodialysis
Key distinction from B12: No neurological complications (subacute combined degeneration does NOT occur with isolated folate deficiency)
Summary Table
| Feature | IDA | B12 Deficiency | Folate Deficiency |
|---|---|---|---|
| MCV | Low (microcytic) | High (macrocytic) | High (macrocytic) |
| Serum ferritin | Low | Normal | Normal |
| TIBC | High | Normal | Normal |
| Serum B12 | Normal | Low | Normal |
| Serum folate | Normal | Normal | Low |
| Methylmalonic acid | Normal | High | Normal |
| Homocysteine | Normal | High | High |
| Neuro signs | None | Yes (SCD) | None |
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, pp. 608-612
- Robbins & Kumar Basic Pathology, pp. 393-395
- Basic Medical Biochemistry - A Clinical Approach (6e), p. 1537
Balanced diet
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive answer on Balanced Diet:
Balanced Diet
Definition
A balanced diet is defined as one which contains a variety of foods in such quantities and proportions that the need for energy, amino acids, vitamins, minerals, fats, carbohydrates, and other nutrients is adequately met for:
- Maintaining health, vitality, and general well-being
- Making a small provision for extra nutrients to withstand short periods of leanness
A balanced diet has become an accepted means to safeguard a population from nutritional deficiencies.
Components of a Balanced Diet
A balanced diet must supply all six classes of nutrients:
| Nutrient Class | Function | Sources |
|---|---|---|
| Carbohydrates | Primary energy source | Cereals, rice, wheat, bread, pasta |
| Proteins | Growth, repair, enzymes, immunity | Meat, fish, eggs, milk, legumes, nuts |
| Fats | Energy, fat-soluble vitamins, cell membranes | Oils, butter, nuts, fish |
| Vitamins | Metabolic co-factors, immunity | Fruits, vegetables, dairy, eggs |
| Minerals | Bone, enzyme function, electrolytes | Dairy (Ca), meat (Fe, Zn), iodized salt |
| Water | Transport, temperature regulation | Fluids, fruits, vegetables |
| Dietary Fibre | Gut health, prevents constipation, cancer | Whole grains, fruits, vegetables |
Principles of Constructing a Balanced Diet
The following principles guide the construction of a balanced diet:
(a) Protein should be the first priority - should account for 10-15% of daily energy intake
(b) Fat should be limited to 15-30% of daily energy intake
(c) Carbohydrates rich in natural fibre should constitute the remaining food energy (complex carbohydrates preferred)
(d) Energy-dense foods such as fats and alcohol should be restricted
(e) Salt intake should be reduced to not more than 5 g/day (average Indian intake is ~15 g/day)
(f) Protein should account for approximately 10-15% of daily intake
(g) Junk foods (colas, ketchups, processed foods that supply empty calories) should be minimised
The Food Guide Pyramid
The food guide pyramid is a visual tool for constructing a balanced diet, showing recommended daily servings from each food group:
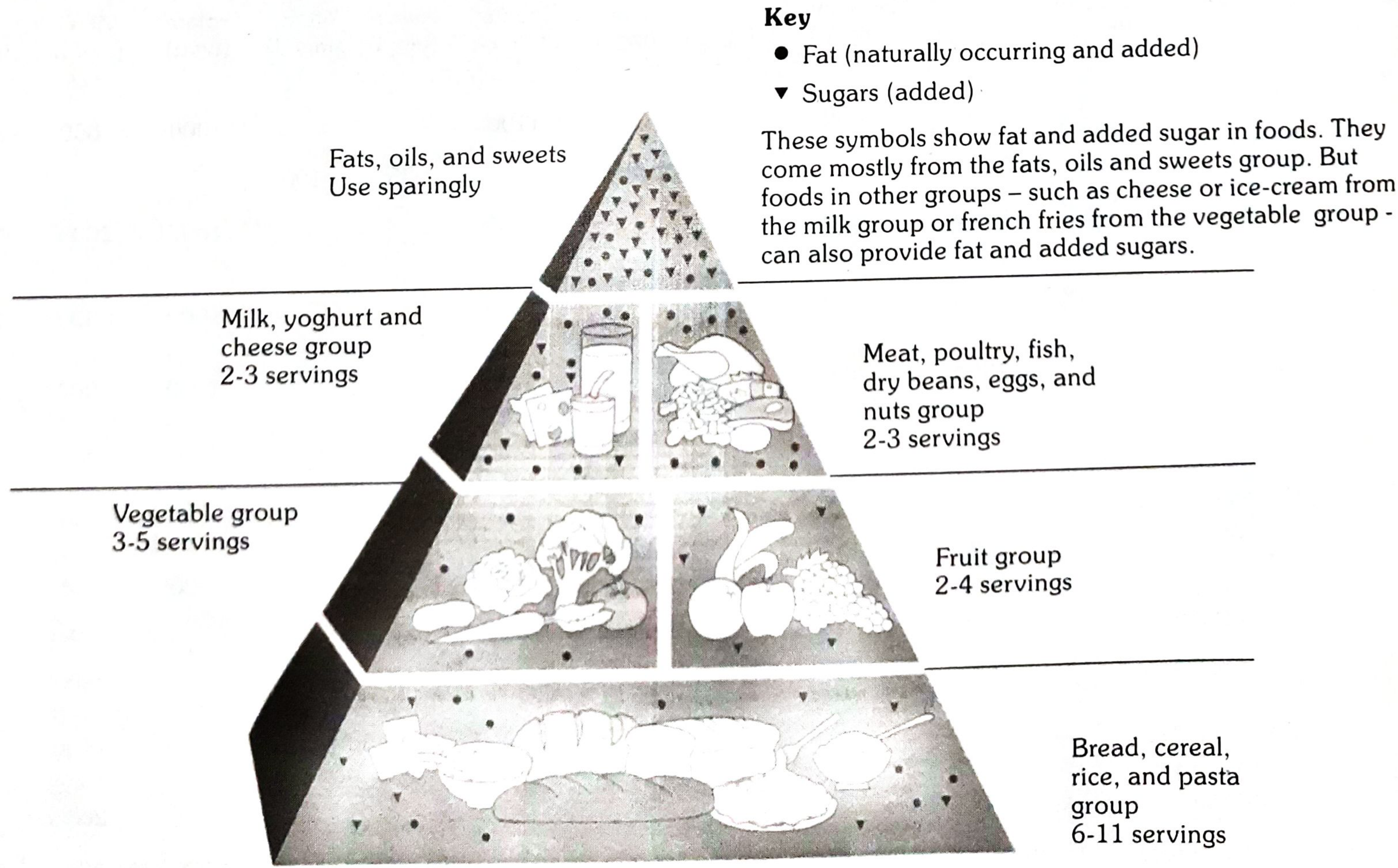
| Food Group | Daily Servings |
|---|---|
| Bread, cereal, rice, pasta (base) | 6-11 servings |
| Vegetable group | 3-5 servings |
| Fruit group | 2-4 servings |
| Milk, yoghurt, cheese | 2-3 servings |
| Meat, poultry, fish, eggs, nuts | 2-3 servings |
| Fats, oils, sweets (apex) | Use sparingly |
Recommended Dietary Allowances (RDA) for Indians - 2020
Key reference values for a moderately active adult Indian male (65 kg):
| Nutrient | RDA |
|---|---|
| Protein | 54 g/day |
| Dietary Fibre | 41 g/day |
| Calcium | 1000 mg/day |
| Iron | 19 mg/day |
| Zinc | 17 mg/day |
| Iodine | 150 μg/day |
| Vitamin C | 80 mg/day |
| Vitamin A | 1000 μg/day |
| Vitamin D | 600 IU/day |
| Folate | 300 μg/day |
| Vitamin B12 | 2.2 μg/day |
For moderately active adult Indian female (55 kg): Protein 46 g/day, Iron 29 mg/day, Calcium 1000 mg/day, Vitamin A 840 μg/day.
Special Dietary Needs
The standard balanced diet must be adapted for:
- Growth (children, adolescents) - increased protein, calcium, iron
- Pregnancy - extra protein (+9.5 g in 2nd trimester, +22 g in 3rd trimester), iron (27 mg/day), folate, iodine
- Lactation - increased caloric intake, calcium, vitamins
- Physical activity - increased energy and B vitamins
- Medical disorders - e.g., diabetics need controlled carbohydrates; renal patients need protein restriction
Characteristics of a Good Balanced Diet (Summary - "ABCDE")
- Adequate - meets all nutrient requirements
- Balanced - correct proportions of macronutrients and micronutrients
- Calorie-appropriate - energy intake matches energy expenditure
- Diverse - variety of foods from all food groups
- Economical - affordable and culturally acceptable
Source: Park's Textbook of Preventive and Social Medicine, pp. 734-735
Lathyrism
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Excellent - comprehensive content from both Park's (PSM) and Adams & Victor's Neurology. Here is the complete answer:
Lathyrism
Definition
Lathyrism is a paralyzing disease of humans and animals caused by the prolonged consumption of the pulse Lathyrus sativus (commonly known as "Khesari dhal"). It exists in two forms:
- Neurolathyrism (in humans) - affects the nervous system; characterized by spastic paralysis of the lower limbs
- Osteolathyrism / Odoratism (in animals) - pathological changes occur in bones, resulting in skeletal deformities
The disease has been known since ancient times - recognized by Hippocrates, Pliny, Galen, and Avicenna.
The Causative Pulse - Lathyrus sativus
- Commonly called "Khesari dhal" (also: Teora dhal, Lak dhal, Batra, Gharas, Matra)
- Seeds have a characteristic triangular shape and grey colour
- When dehusked, resembles red gram or Bengal gram dhal
- A good source of protein, but contains a neurotoxin
- Eaten mainly by poor agricultural labourers because it is relatively cheap
- A drought-resistant, hardy crop that survives when other crops fail - hence consumed during famines
- Diets containing >30% Khesari dhal over 2-6 months result in neurolathyrism
The Toxin
- Identified as Beta-Oxalyl Amino Alanine (BOAA) - also written as beta-N-oxalamino-L-alanine
- Isolated in crystalline form; is water soluble (important for detoxification)
- Acts as a neuroexcitatory amino acid (excitotoxin) at glutamate receptors
- There is a blood-brain barrier to this toxin - the pulse must be eaten in large quantities over at least 2 months for the toxin to overcome this barrier
- BOAA induces corticospinal dysfunction, as demonstrated in primate models
Epidemiology / The Problem
- Endemic in parts of Madhya Pradesh, Uttar Pradesh, Bihar, Orissa, and also reported in Maharashtra, West Bengal, Rajasthan, Assam, Gujarat
- Historical burden: Rewa and Satna districts of MP alone had 25,000 and 32,000 cases respectively at one time
- Also reported in Spain and Algeria
- Fresh outbreaks have declined due to shifting agronomical practices
- Similar disease: Konzo (Africa) - acute spastic paraplegia due to cyanide-like compounds in cassava flour
Clinical Features
The disease affects mainly young men aged 15-45 years and manifests in progressive stages:
Stages of Neurolathyrism
| Stage | Description |
|---|---|
| (a) Latent stage | Apparently healthy; exhibits ungainly gait only on physical stress. Neurological signs present. Complete remission possible if pulse is withdrawn at this stage. |
| (b) No-stick stage | Walks with short, jerky steps without a stick. Most patients found at this stage. |
| (c) One-stick stage | Crossed gait, tendency to walk on toes, muscular stiffness; requires one stick for balance. |
| (d) Two-stick stage | More severe; excessive bending of knees and crossed legs; needs two crutches; slow and clumsy gait, tires easily. |
| (e) Crawler stage | Cannot maintain erect posture; knee joints cannot bear body weight; atrophy of thigh and leg muscles; patient crawls by throwing weight on hands. |
Other Neurological Features (from Adams & Victor)
- Pain, paresthesias, numbness in legs
- Frequency and urgency of micturition
- Erectile dysfunction, sphincteric spasms
- Coarse tremors and involuntary movements of upper extremities
- Symptoms are permanent but not progressive once established; patients live out normal lifespan
Neuropathology
- Loss of ascending and descending tracts in the spinal cord - particularly corticospinal and spinocerebellar tracts
- Loss of myelinated fibres in lateral and posterior columns
- Betz cells (upper motor neurons) disappear; anterior horn cells unaffected
- Gliosis and thickening of blood vessels in degenerated tracts
Interventions (Prevention and Control)
(a) Vitamin C prophylaxis
- 500-1000 mg of ascorbic acid daily for a week may help repair damage and prevent progression
- Protective effect demonstrated in guinea pigs and monkeys with lathyrogenic diets
(b) Banning the crop
- The Prevention of Food Adulteration Act in India has banned Lathyrus in all forms (whole, split, or flour)
- However, the ban is difficult to enforce in endemic states
- If consumption cannot be avoided, the dhal should not form more than 1/4 of total cereals and pulses per day
(c) Removal of toxin (Detoxification)
Since BOAA is water soluble, two main methods:
- Steeping method - soak pulse in hot water for 2 hours, drain and discard soak water, wash again, dry in sun. Drawback: loss of vitamins and minerals.
- Parboiling - suitable for large-scale operations; soaking in lime water overnight followed by boiling also destroys toxin and trypsin inhibitors
(d) Genetic approach
- Certain strains of Lathyrus contain very low levels of toxin (~0.1%)
- Selective propagation and cultivation of low-toxin varieties may be the most effective long-term solution
- Low-toxin varieties available from the Indian Agricultural Research Institute (IARI), New Delhi
(e) Education
- Public education on the dangers of consuming Khesari dhal and the need for detoxification before consumption
(f) Socio-economic changes
- Ultimately, eradicating poverty and improving food security is the only way to root out lathyrism, as it is consumed primarily due to poverty and famine
Sources:
- Park's Textbook of Preventive and Social Medicine, pp. 740-741
- Adams and Victor's Principles of Neurology (12th ed.), pp. 1273-1274
Diff between screening and diagnostic test
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the content needed for a comprehensive answer. Here it is:
Difference Between Screening and Diagnostic Test
Definitions
Screening Test
Screening is the testing for infection or disease in populations or individuals who are NOT seeking health care - i.e., apparently healthy persons. The basic purpose is to sort out from a large group of apparently healthy persons those likely to have the disease or at increased risk, in order to bring those who are "apparently abnormal" under medical supervision and treatment.
"Screening is carried out in the hope that earlier diagnosis and subsequent treatment favourably alters the natural history of the disease." - Park's PSM
Diagnostic Test
Diagnostic tests are the use of clinical and/or laboratory procedures to confirm or refute the existence of disease or true abnormality in patients with signs and symptoms presumed to be caused by the disease.
Examples:
- VDRL testing of patients with lesions suggestive of secondary syphilis
- Endocervical culture for N. gonorrhoeae
Key Differences at a Glance
| Feature | Screening Test | Diagnostic Test |
|---|---|---|
| Purpose | Presumptively identify unrecognized disease in apparently healthy people | Confirm or rule out disease in symptomatic individuals |
| Target population | Large, apparently healthy population (asymptomatic) | Symptomatic individuals who present for care |
| Initiative | Initiated by health authorities / public health programmes | Initiated by the patient's symptoms or clinical signs |
| Stage of disease | Pre-clinical / presymptomatic phase | Clinical / symptomatic phase |
| Nature of result | Presumptive - positive result only suggests disease | Definitive - establishes or rules out diagnosis |
| Sensitivity vs. Specificity | High sensitivity preferred (to catch all true cases; few false negatives) | High specificity preferred (to confirm disease; few false positives) |
| Cut-off value | Set lower (more inclusive) to maximize sensitivity | Set at optimal level for accuracy |
| Cost and simplicity | Must be cheap, simple, rapid, acceptable to mass population | Can be more expensive, complex, invasive |
| Follow-up | A positive screen requires a follow-up diagnostic test | Leads to treatment decision directly |
| Risk | Minimal; non-invasive preferred | May be invasive (biopsy, culture, etc.) |
| False positives | More acceptable | Less acceptable |
| False negatives | Less acceptable (missed cases) | Less acceptable (missed diagnosis) |
| Examples | Pap smear for cervical cancer, Mantoux test for TB, neonatal PKU test, mammography | Colposcopy + biopsy, sputum culture, FNAC, blood culture |
Sensitivity and Specificity in Context
Using the 2×2 table:
| Disease Present | Disease Absent | |
|---|---|---|
| Test Positive | a (True Positive) | b (False Positive) |
| Test Negative | c (False Negative) | d (True Negative) |
- Sensitivity = a / (a+c) × 100 → ability to detect true positives
- Specificity = d / (b+d) × 100 → ability to exclude true negatives
- Positive Predictive Value (PPV) = a / (a+b) × 100
- Negative Predictive Value (NPV) = d / (c+d) × 100
For screening tests: High sensitivity is preferred (minimize false negatives - no case should be missed).
For diagnostic tests: High specificity is preferred (minimize false positives - avoid labelling a healthy person as diseased).
Lead Time
"Lead time" is the advantage gained by screening - the time period between diagnosis by early detection (screening) and diagnosis by other means (when symptoms appear). Early detection is only beneficial if treatment during the lead time alters the final outcome.
Important Concept: Case-Finding (an intermediate category)
Case-finding sits between screening and diagnosis - it is the use of tests to detect disease in individuals seeking health care for OTHER reasons (incidental detection). For example, VDRL for syphilis in pregnant women attending antenatal clinics, or checking blood pressure in a patient consulting for a headache.
Summary Statement
The distinction between screening, case-finding, and diagnosis should be clear-cut, but it is often blurred by the multiplicity of tests used. The same test (e.g., VDRL) may be used in different contexts - as a screening test in premarital screening, as a case-finding test in antenatal care, and as a diagnostic test in a patient with skin lesions of secondary syphilis. In evaluating a test, one must always consider whether it is being used for screening or diagnosis.
Source: Park's Textbook of Preventive and Social Medicine, pp. 155-159; Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Esi benefits
Finding Sources
Searching the Web
ESI benefits Employees State Insurance scheme India 2024
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent - all content is now available. Here is the complete answer:
ESI (Employees' State Insurance) Benefits
Overview
The Employees' State Insurance (ESI) Act was passed in 1948 (amended in 1975, 1984, 1989, 2010, and 2019). It is an important measure of social security and health insurance in India that provides certain cash and medical benefits to industrial employees in case of sickness, maternity, and employment injury.
Finance / Contributions
| Contributor | Rate |
|---|---|
| Employer | 3.25% of total wage bill |
| Employee | 0.75% of wages |
| State Government | 1/8 of total cost of medical care |
| ESI Corporation | 7/8 of total cost of medical care |
- Employees earning below Rs. 176/day are exempted from payment
- Coverage extended to employees earning up to Rs. 21,000/month
Benefits to Employees
The Act provides 7 categories of benefits to insured persons:
1. Medical Benefit
Full medical care, free of cost, for insured persons and their families in case of sickness, employment injury, and maternity. Services include:
- Out-patient care
- Supply of drugs and dressings
- Specialist services in all branches of medicine
- Pathological and radiological investigations
- Domiciliary services
- Antenatal, natal and postnatal services
- Immunization services
- Family planning services
- Emergency services
- Ambulance services
- Health education
- In-patient treatment
Additional provisions:
- Dentures, spectacles, and hearing aids - provided free for those incapacitated due to employment injury
- Artificial limbs - provided free to those who lose limbs in employment injury
- Special appliances (hernia belts, walking callipers, surgical boots, spinal braces) as prescribed
2. Sickness Benefit
- Periodical cash payment at about 70% of average daily wages
- Payable for a maximum of 91 days in any continuous period of 365 days
- Must be certified by an Insurance Medical Officer/Practitioner
- The employee cannot be dismissed by employer during the period of sickness
Extended Sickness Benefit:
- For insured persons with 34 specified long-term diseases, benefit is extended for up to 2 years (if employed continuously for 2 years)
- Diseases include: TB, leprosy, AIDS, malignant diseases, diabetes with complications, neurological disorders (hemiplegia, paraplegia, Parkinson's, etc.), cardiovascular diseases (CAD, CHF, cardiomyopathies), COPD, cirrhosis, chronic renal failure, schizophrenia, MDP, Burger's/Raynaud's disease, major burns, etc.
Enhanced Sickness Benefit (Sterilisation):
- Payable for sterilisation operations at double the standard benefit rate (= full wages)
- Females: 14 days (tubectomy); Males: 7 days (vasectomy)
3. Maternity Benefit
Cash benefit payable to an insured woman:
| Condition | Duration |
|---|---|
| Confinement (normal delivery) | 26 weeks |
| Miscarriage | 6 weeks |
| Sickness arising out of confinement | 30 days |
- Rate: approximately full wages
- Confinement expenses: Rs. 7,500 per confinement
4. Disablement Benefit
Cash payment + free medical treatment in case of employment injury or occupational disease:
| Type | Rate |
|---|---|
| Temporary disablement | ~90% of wages for as long as disability lasts |
| Total permanent disablement | Life pension based on loss of earning capacity (determined by Medical Board) |
| Partial permanent disablement | Portion of above as life pension |
5. Dependant's Benefit
- Payable to dependants of an insured person who dies due to employment injury
- Pension at 90% of wages, shared among dependants in fixed ratio, on monthly basis
- Eligible son/daughter receives benefit up to age 18 (withdrawn on daughter's marriage)
6. Funeral Expenses
- Lump sum cash payment on death of insured person towards funeral expenses
- Amount: up to Rs. 15,000/-
7. Rehabilitation Allowance
- On monthly payment of Rs. 10, the insured person and family continue to receive medical treatment after permanent disablement or retirement
Rajiv Gandhi Shramik Kalyan Yojana (Unemployment Benefit)
Launched by ESIC (effective 1 April 2005) for employees rendered involuntarily unemployed due to retrenchment, factory closure, or permanent invalidity from non-employment injury:
- Eligibility: At least 5 years of insurable employment
- Benefit: Unemployment allowance for up to 6 months (in one or multiple spells, min. 1 month each)
- Rate: Standard benefit rate under ESI (Central) Rules, 1950
Benefits to Employers
- Exemption from the Workmen's Compensation Act, 1923
- Exemption from the Maternity Benefit Act, 1961
- Exemption from providing medical allowance/care to employees
- Income Tax rebate on contribution deposited in ESI Account
- Assurance of a healthy, productive workforce
Current Coverage: By 31.03.2020, the ESI Scheme covered ~309 lakh employees (including 62.6 lakh women), with ~1324 lakh total beneficiaries across 34 States/Union Territories.
Source: Park's Textbook of Preventive and Social Medicine, pp. 919-921
This is a shared conversation. Sign in to Orris to start your own chat.