Treatment of hypertension
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "treatment" AND "guidelines"
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
I have comprehensive content. Now I have enough to write a thorough, well-organized answer.
Treatment of Hypertension
1. Goals of Treatment
The primary goal is to reduce cardiovascular morbidity and mortality by lowering blood pressure (BP) to target levels.
BP Targets (ACC/AHA 2017/2018 guidelines):
- Most patients: < 130/80 mm Hg
- Patients aged ≥65 years: < 130 mm Hg systolic
- Diabetes: < 130/80 mm Hg (consider < 120/80 mm Hg in high CV risk + low medication-adverse-effect risk)
- Note on SPRINT data: Trials using rigorous measurement protocols show mortality benefit at systolic < 120 mm Hg; because standardized protocols yield readings ~10 mm Hg lower than routine clinic measurements, this effectively corresponds to < 130 mm Hg in typical clinical practice
2. Lifestyle Modification
Lifestyle changes are first-line for elevated BP and Stage 1 hypertension, and are additive to drug therapy at all stages. They can reduce systolic BP by 7-15 mm Hg.
| Intervention | Expected SBP Reduction |
|---|---|
| DASH diet (high fruits, vegetables, low-fat dairy; low saturated fat) | ~6 mm Hg |
| Sodium restriction: < 1500 mg/day (or ≥ 1000 mg/day reduction) | 4-8 mm Hg |
| Aerobic/dynamic resistance exercise, 90-150 min/week | 4-8 mm Hg |
| Weight loss (per 10 kg) | ~5-7 mm Hg |
| Limit alcohol: ≤2 drinks/day (men), ≤1 drink/day (women) | 2-4 mm Hg |
| Smoking cessation | Reduces CV risk overall |
~70% of dietary sodium comes from processed food, so simply avoiding added salt is insufficient for most patients.
- Goldman-Cecil Medicine, Treatment of Essential Hypertension, Table 64-6
3. Antihypertensive Drug Classes
Four first-line drug classes form the backbone of treatment:
| Class | Examples | Key Notes |
|---|---|---|
| ACE inhibitors (ACEi) | Lisinopril, ramipril, enalapril | First-line; preferred in diabetes, CKD, HFrEF; avoid in pregnancy |
| Angiotensin receptor blockers (ARBs) | Losartan, valsartan, telmisartan | Equivalent to ACEi; preferred when ACEi-cough occurs |
| Calcium channel blockers (CCBs) | Amlodipine (DHP); verapamil, diltiazem (non-DHP) | DHP preferred in most; non-DHP useful in AF rate control |
| Thiazide/thiazide-like diuretics | Chlorthalidone (preferred by ACC/AHA), hydrochlorothiazide, indapamide | US guidelines specifically prefer chlorthalidone |
Why these four? Monotherapy's BP-lowering effect is blunted by counter-regulatory pressor activation. For example, diuretics activate the renin-angiotensin system; adding an ACEi/ARB blocks this escape mechanism, producing synergistic BP reduction.
- Comprehensive Clinical Nephrology 7e; Fuster and Hurst's The Heart 15e
4. Stepwise Treatment Algorithm
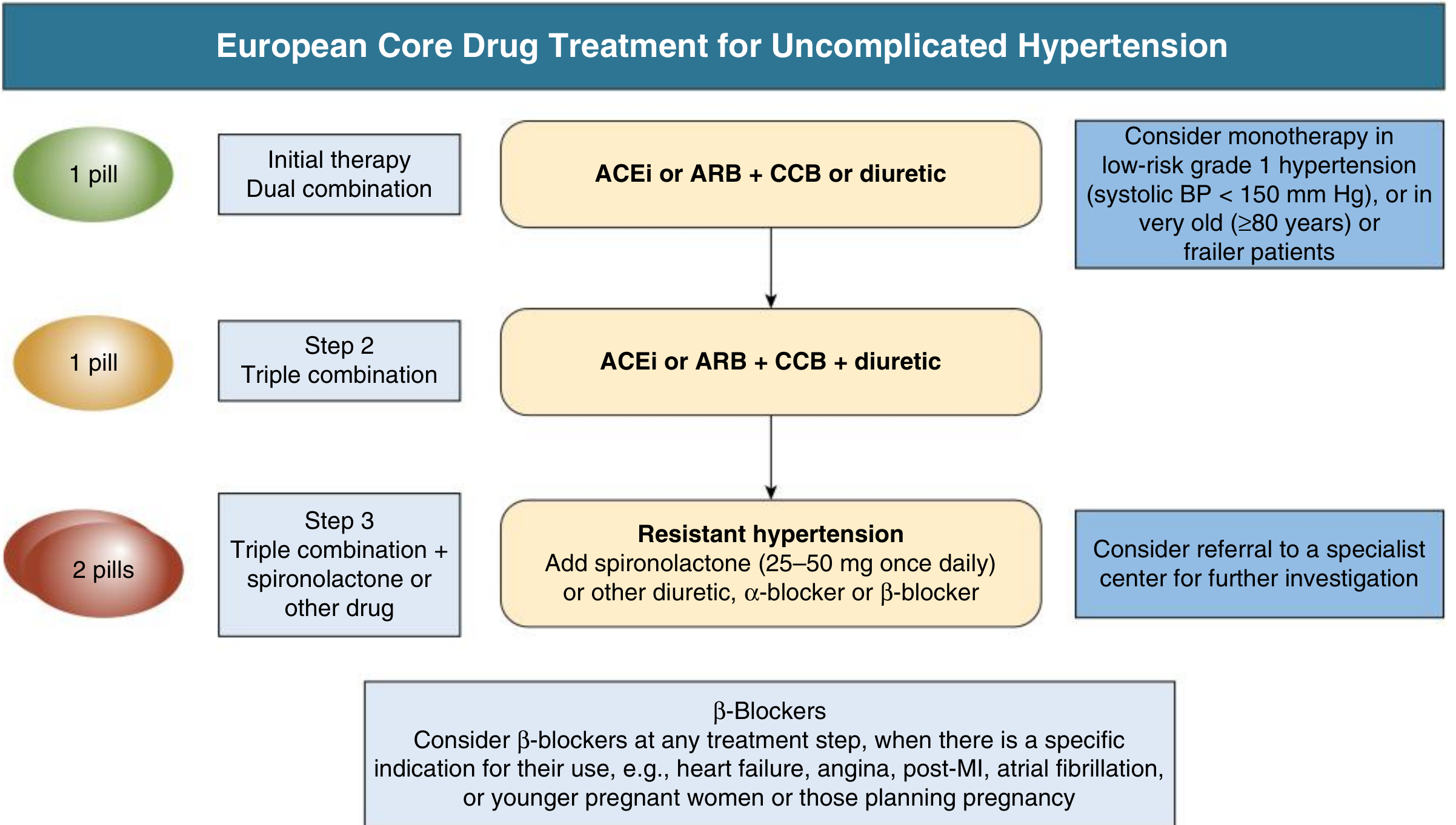
Fig. 37.3 - European Core Drug Treatment Algorithm (also appropriate for hypertension-mediated organ damage, cerebrovascular disease, diabetes, peripheral vascular disease). From Fuster and Hurst's The Heart, 15e.
Step 1 - Initial therapy (dual combination):
- ACEi or ARB + CCB or thiazide diuretic (as a single-pill combination where available)
- Monotherapy is acceptable only in: low-risk Grade 1 hypertension (SBP < 150 mm Hg), very old (≥80 years), or frail patients
Why start with two drugs? Current BP targets (< 130/80 mm Hg) are rarely achievable with one agent, and dual therapy also reduces activation of counter-regulatory pressor systems.
Step 2 - Triple combination:
- ACEi or ARB + CCB + thiazide diuretic (ideally one pill)
Step 3 - Resistant hypertension:
- Add spironolactone 25-50 mg once daily
- Alternatively: additional diuretic, alpha-blocker, or beta-blocker
- Consider specialist referral
Beta-blockers: Used at any step when there is a specific indication (heart failure with reduced EF, angina, post-MI, atrial fibrillation for rate control, younger pregnant women or those planning pregnancy) - not routinely as first-line for uncomplicated hypertension.
US guidance (ACC/AHA Table):
-
Stage 2 HTN (BP > 20/10 mm Hg above target): start with two first-line agents (Grade I, LOE C)
-
Stage 1 HTN with BP goal < 130/80 mm Hg: monotherapy reasonable with titration (Grade IIa, LOE C)
-
Fuster and Hurst's The Heart 15e, Table 37.9; Comprehensive Clinical Nephrology 7e
5. Compelling Indications - Drug Selection by Comorbidity
| Condition | Preferred Agents |
|---|---|
| Heart failure with reduced EF (HFrEF) | ACEi/ARB, beta-blocker, aldosterone antagonist (spironolactone/eplerenone), loop diuretics |
| Post-MI | ACEi/ARB, beta-blocker |
| Diabetes mellitus | ACEi or ARB (nephroprotective); CCB or thiazide as add-on |
| Chronic kidney disease (CKD) / proteinuria | ACEi or ARB (reduce proteinuria, slow progression) |
| Atrial fibrillation (rate control) | Beta-blocker or non-DHP CCB (verapamil/diltiazem) |
| Angina | Beta-blocker, CCB |
| Pregnancy | Methyldopa, labetalol, nifedipine; ACEi/ARBs are CONTRAINDICATED |
| Isolated systolic HTN in elderly | Dihydropyridine CCB, thiazide diuretic |
| High stroke risk / cerebrovascular disease | ACEi + thiazide diuretic combination (PROGRESS trial data) |
- Goldman-Cecil Medicine, Table 64-9
6. Resistant Hypertension
Defined as BP above goal despite 3 antihypertensive agents of different classes (including a diuretic) at optimal doses, or BP requiring ≥4 medications to control.
Before diagnosing true resistance, exclude:
- White coat hypertension (confirm with 24-hour ambulatory BP monitoring)
- Poor medication adherence (most common cause)
- Secondary hypertension (primary aldosteronism, renal artery stenosis, sleep apnea, pheochromocytoma, Cushing syndrome)
- Drug effects raising BP: NSAIDs, oral contraceptives, decongestants, stimulants, cyclosporine
Management:
-
Intensify diuretic therapy - chlorthalidone or thiazide optimization
-
Add spironolactone 25-50 mg/day (most effective fourth agent; particularly useful if covert primary aldosteronism is contributing)
-
Alternatively: eplerenone, amiloride, alpha-blockers (doxazosin), centrally-acting agents (clonidine)
-
Specialist referral recommended
-
National Kidney Foundation Primer on Kidney Diseases 8e; Comprehensive Clinical Nephrology 7e
7. Drug Interactions and Cautions
-
NSAIDs (except sulindac, celecoxib at standard doses): raise BP and impair renal function - avoid or use with caution
-
Acetaminophen: can raise BP by unknown mechanisms
-
Grapefruit + dihydropyridine CCBs (except amlodipine): causes excessive vasodilation via CYP3A4 inhibition - avoid
-
Verapamil/diltiazem + statins (simvastatin, atorvastatin): CYP3A4 inhibition raises statin levels; use lower statin doses; simvastatin ≤20 mg/day with amlodipine
-
ACEi + ARB combination: NOT recommended (dual RAS blockade increases hyperkalemia and AKI risk without added BP benefit)
-
ACEi/ARB in pregnancy: strictly contraindicated (teratogenic - renal dysgenesis, oligohydramnios)
-
Iron + methyldopa: iron reduces methyldopa absorption by 50% in pregnant women
-
Goldman-Cecil Medicine, Antihypertensive Drug Interactions
8. Special Populations
Elderly (≥65-75 years):
- Treat to < 130 mm Hg systolic if tolerated; SPRINT showed benefit in those ≥75 years including frail non-institutionalized patients
- Start low, go slow; monitor for orthostatic hypotension
- A 2024 Cochrane review (PMID 39688187) examined higher BP targets in older adults - ongoing refinement of optimal targets in this group
Pregnancy:
- Target BP: < 140/90 mm Hg (ACOG/SMFM)
- Safe agents: labetalol, nifedipine, methyldopa
- ACEi and ARBs are contraindicated
CKD:
- ACEi or ARB preferred for their antiproteinuric effects
- Target < 130/80 mm Hg (or more aggressive in high-proteinuria states)
- Avoid dual ACEi + ARB blockade
Diabetes:
- Target < 130/80 mm Hg; ACEi/ARB first-line
- SGLT2 inhibitors (empagliflozin, canagliflozin) have emerging antihypertensive and cardiorenal benefits and are increasingly integrated into treatment
9. Key Principles Summary
- Lifestyle modification is foundational at every stage - never omit it
- Start with two drugs for most patients with BP ≥ 140/90 mm Hg (or ≥20/10 mm Hg above target)
- Backbone of therapy: ACEi or ARB + CCB and/or thiazide diuretic
- Single-pill combinations improve adherence substantially
- Beta-blockers are not first-line for uncomplicated hypertension but are appropriate when compelling indications exist
- Spironolactone is the evidence-based fourth agent for resistant hypertension
- Avoid therapeutic inertia - failure to uptitrate or combine drugs is a leading cause of poor BP control
Recent evidence note (PMID 39688187, Cochrane 2024): Ongoing debate exists around optimal BP targets in older adults (≥80 years). The Cochrane meta-analysis examined whether higher targets (less aggressive treatment) may reduce harms in this age group. Clinicians should individualize targets considering frailty, cognitive status, and fall risk.
Sources: Goldman-Cecil Medicine International Edition; Fuster and Hurst's The Heart, 15e; Comprehensive Clinical Nephrology, 7e; ACC/AHA 2017/2018 Hypertension Guidelines; ESC/ESH 2018 Practice Guidelines
What is the indication and importance of chosing CCB or Thiazode diuretics along with arbs
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the material needed for a thorough, focused answer. Here it is:
ARB + CCB vs. ARB + Thiazide Diuretic: Indications and Rationale
Why Combine ARB with a Second Agent at All?
The core reason is pharmacological escape. Monotherapy with any single agent triggers compensatory counter-regulatory responses that blunt its effect:
- A CCB causes vasodilation → reflexively activates the renin-angiotensin-aldosterone system (RAAS) → limits sustained BP reduction
- A thiazide diuretic causes sodium/water loss → activates RAAS → limits sustained BP reduction
Adding an ARB (which blocks angiotensin II at the AT1 receptor) directly interrupts this escape mechanism for both drugs, making the combination genuinely synergistic rather than merely additive.
"A two-drug combination will produce much greater BP lowering than even the most effective monotherapy; studies have shown this approach is twice as effective as monotherapy at achieving BP control within 3 to 4 months."
- Comprehensive Clinical Nephrology, 7e
ARB + CCB
Mechanism of synergy
| Component | Primary Action |
|---|---|
| ARB | Blocks AT1 receptor → prevents vasoconstriction and aldosterone release |
| CCB (dihydropyridine, e.g., amlodipine) | Blocks L-type voltage-gated Ca²⁺ channels → arterial vasodilation |
The ARB counters the RAAS activation that the CCB triggers, while the CCB provides direct arterial dilation that the ARB alone does not produce. Together they address both neurohormonal and vascular smooth muscle mechanisms.
Key indications and advantages (prefer ARB + CCB when)
- High cardiovascular risk (coronary artery disease, diabetes, prior stroke, peripheral vascular disease)
- Metabolic concerns: CCBs are metabolically neutral - no effect on glucose, lipids, or uric acid; ARBs may actually improve insulin sensitivity. This makes the combination ideal in diabetes or metabolic syndrome
- Elderly patients with isolated systolic hypertension: amlodipine is highly effective in this population
- Black patients: CCBs have superior BP-lowering efficacy in this population (and ARBs/ACEi have reduced monotherapy efficacy in Black patients due to lower renin states, but the combination works well)
- Angina coexisting with hypertension: CCB provides additional anti-anginal benefit
- Reduced ankle edema: ARB co-administration reduces the peripheral edema caused by dihydropyridine CCBs (by opposing arteriolar dilation with the venous dilation that ARBs also produce, balancing the Starling forces)
ACCOMPLISH trial evidence
The landmark ACCOMPLISH trial (Jamerson et al., 2008) directly compared:
- Benazepril (ACEi) + amlodipine (CCB) vs. Benazepril + hydrochlorothiazide (thiazide)
Result: the ACEi + CCB combination produced a 20% relative reduction in combined cardiovascular events compared with ACEi + thiazide, across all subgroups including those with diabetes, CAD, and CKD. This was the only hypertension trial with hard CV outcomes designed around combination regimens, and it strongly favored the RAS blocker + CCB combination.
"We have previously suggested that most patients who require dual antihypertensive therapy should strongly consider starting with an ACE inhibitor or ARB plus a CCB."
- Textbook of Family Medicine, 9e
ARB + Thiazide Diuretic
Mechanism of synergy
| Component | Primary Action |
|---|---|
| ARB | Blocks AT1 receptor → opposes RAAS |
| Thiazide (e.g., chlorthalidone, hydrochlorothiazide, indapamide) | Inhibits Na⁺/Cl⁻ cotransporter in distal convoluted tubule → natriuresis → volume reduction |
Thiazides reduce intravascular volume, but this triggers RAAS activation. The ARB directly blocks this counter-regulation, allowing the volume depletion to translate into sustained BP reduction.
Key indications and advantages (prefer ARB + thiazide when)
- Volume-dependent or sodium-sensitive hypertension (common in elderly, Black patients, CKD, high-sodium diet)
- Heart failure with fluid overload: diuretic component addresses congestion, ARB provides cardiac remodeling benefit
- Osteoporosis: thiazides reduce urinary calcium excretion (a secondary benefit in at-risk patients)
- Lower cost: this combination has long been generically available and is very inexpensive
- Stroke prevention: the perindopril + indapamide combination (PROGRESS trial) showed significant stroke reduction; consistent with ARB + thiazide rationale
- When a CCB is not tolerated (e.g., persistent symptomatic edema or flushing despite dose reduction)
Side effects to monitor
Because the ARB partially offsets RAAS activation from the diuretic, hypokalemia is less severe than with thiazide alone. However, other thiazide metabolic effects still occur:
- Hyponatremia
- Hyperuricemia (can precipitate gout)
- Impaired glucose tolerance / new-onset diabetes (higher incidence than with CCB combinations - this was a key finding in ALLHAT)
- Dyslipidemia (mild)
Head-to-Head Comparison
| Feature | ARB + CCB | ARB + Thiazide |
|---|---|---|
| CV outcome evidence | Superior (ACCOMPLISH) | Good (ALLHAT, PROGRESS) |
| Metabolic neutrality | Excellent (no glucose/lipid effects) | Lower (new-onset DM risk) |
| Preferred in diabetes | Yes (first choice) | Acceptable but CCB preferred |
| Preferred in heart failure + fluid overload | Less so | Yes |
| Ankle edema | CCB can cause; reduced by ARB | Not an issue |
| Electrolyte effects | Minimal | Hypokalemia, hyponatremia, hyperuricemia |
| Stroke prevention | Strong | Strong (PROGRESS) |
| Black patients | Good | Good (volume-sensitive HTN) |
| Osteoporosis | No benefit | Benefit (reduced Ca²⁺ excretion) |
| Cost | Moderate (generic available) | Very low (both generic) |
What to Avoid: Dual RAS Blockade (ARB + ACEi)
This is explicitly not recommended. Combining two RAAS-blocking agents (e.g., ARB + ACEi, or ARB + aliskiren) produces no additional cardiovascular benefit over monotherapy but significantly increases the risk of:
- Acute kidney injury
- Hyperkalemia
Multiple large trials (including ONTARGET) confirmed this, and all major international guidelines prohibit dual RAS blockade.
- Comprehensive Clinical Nephrology, 7e; National Kidney Foundation Primer on Kidney Diseases, 8e
Practical Summary
- Default first choice for most patients: ARB (or ACEi) + CCB - better CV outcome data (ACCOMPLISH), metabolically neutral, reduces CCB-induced edema
- Prefer ARB + thiazide in volume-dependent HTN, heart failure with congestion, patients at low metabolic risk, or where cost is the dominant concern
- Step 2: All three together (ARB + CCB + thiazide) as a single-pill triple combination when dual therapy is insufficient
- Never combine ARB + ACEi as a strategy for BP control
This is a shared conversation. Sign in to Orris to start your own chat.