Feeding tube, different part and details structure and how it works
Reading File
Finding Sources
Finding Sources
Searching the Web
feeding tube parts structure types how it works nasogastric PEG tube anatomy
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content and images. Let me compile the full, detailed answer.
Feeding Tubes: Types, Structure, Parts, and How They Work
What Is a Feeding Tube?
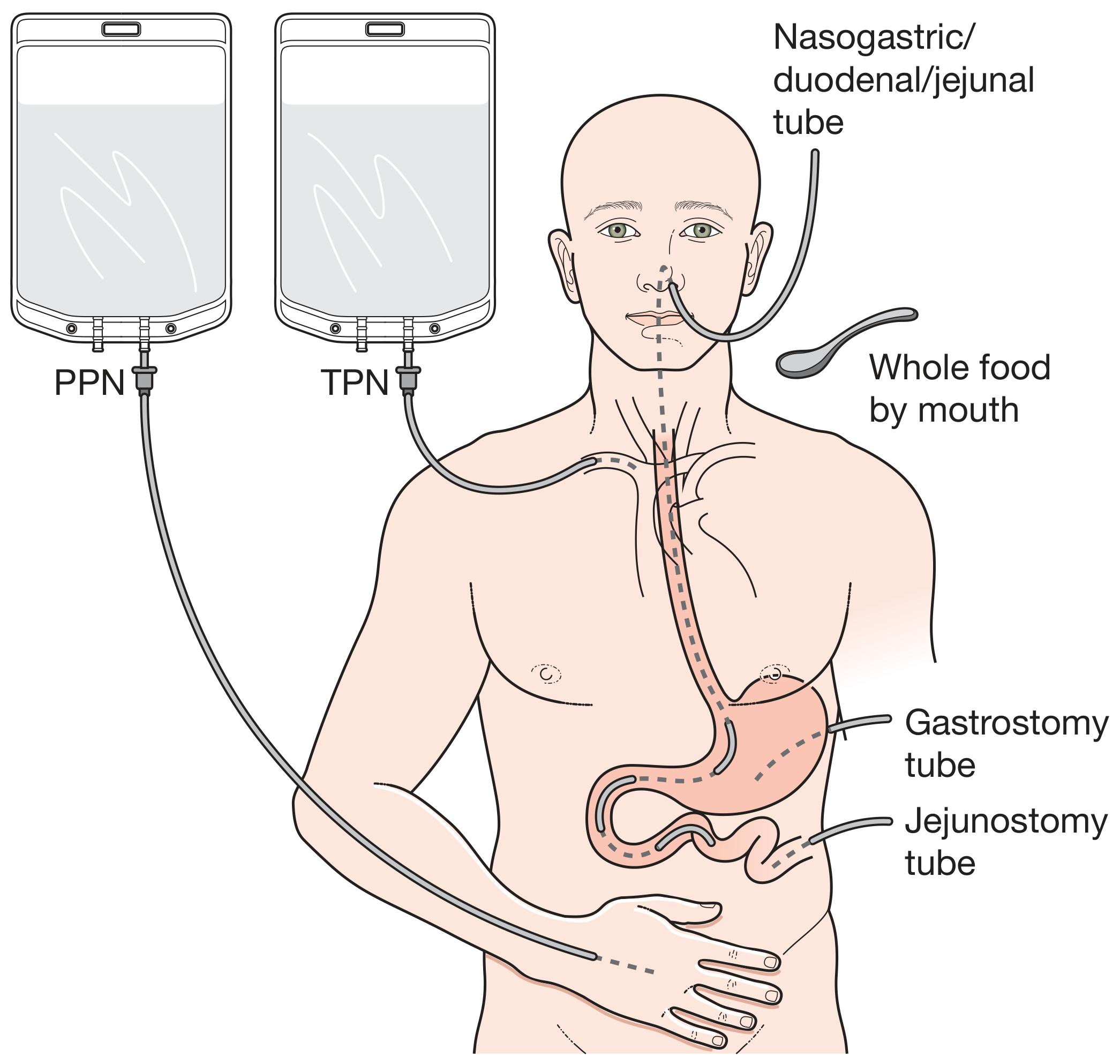
A feeding tube is a flexible medical device inserted into the gastrointestinal (GI) tract to deliver nutrition, fluids, and medications to patients who cannot maintain adequate oral intake. Enteral nutrition (via the gut) is always preferred over parenteral (intravenous) nutrition because it preserves the gut mucosal barrier, maintains gut immunity, prevents gut atrophy, reduces infection rates, improves wound healing, and shortens hospital stays. - Bailey & Love's Surgery, p. 357
Feed formulations typically contain 1-2 kcal/mL and up to 0.6 g/mL protein, with variable fat, nitrogen, and osmolarity content.
Classification: How Tubes Are Categorized
Feeding tubes are classified in two ways:
1. By Entry Site (where the tube enters the body):
- Nasal route - through the nostril (nares)
- Abdominal route - directly through the abdominal wall (ostomy)
2. By Tip Location (where the tube ends inside the body):
-
Stomach (gastric) - nasogastric (NG) tube, gastrostomy (G/PEG) tube
-
Duodenum - nasoduodenal tube
-
Jejunum (small intestine) - nasojejunal (NJ) tube, jejunostomy (J) tube
-
Both stomach and jejunum - PEG-J tube (dual lumen)
-
Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 968-970
Major Types in Detail
1. Nasogastric (NG) Tube
The most common type. Inserted through the nose, travels down the esophagus, and ends in the stomach.
Two main designs:
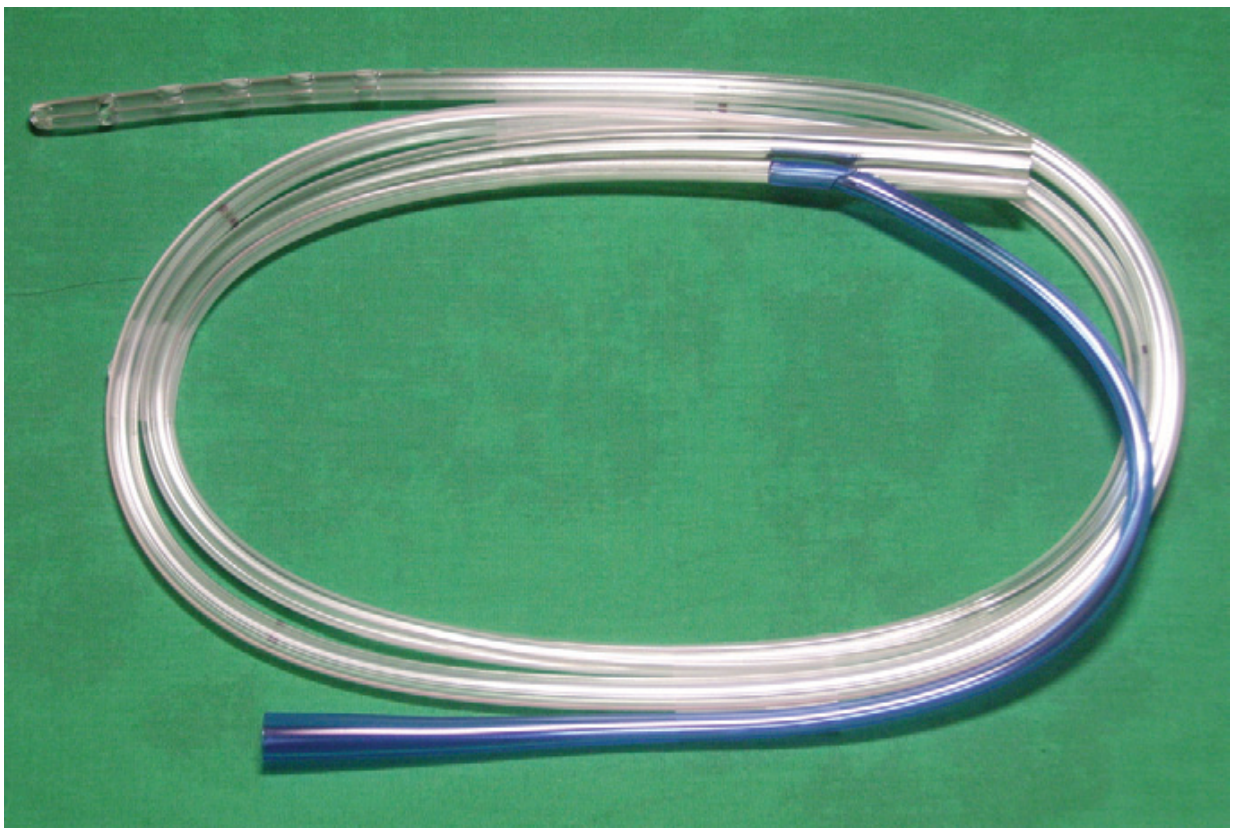
A. Levin Tube (single-lumen)
- Firm, straight, single-lumen construction
- Multiple distal side ports (openings near the tip) for drainage/aspiration
- Used primarily for gastric aspiration, lavage, and short-term feeding
- Limitation: the lumen can become occluded by gastric mucosa when suction is applied, potentially damaging mucosa
B. Salem Sump Tube (double-lumen)
- Two lumens running side by side:
- Main lumen (large): for suction, feeding, medication delivery
- Vent lumen (small, blue "pigtail"): provides a constant low-level airflow into the stomach, preventing the main lumen from being blocked by mucosa
- Multiple distal side ports
- Antireflux valves available for the vent to prevent back-leakage
- Proximal multiport adapters allow the same tube to be used for feeding, irrigating, suctioning, or medicating
- Material: clear radiopaque polypropylene or silicone
C. Fine-Bore Feeding Tube (e.g., Dobhoff, Entri-Flex)
Specifically designed for long-term enteral feeding:
- Made of soft polyurethane or silicone (becomes even softer at body temperature)
- Very small diameter - comfortable for prolonged use
- Tungsten-weighted tip or balloon near the distal end - the weight helps the tube migrate past the pylorus into the duodenum/jejunum under gravity and peristalsis
- Removable stylet/stiffening wire inserted before placement to give rigidity; removed after positioning is confirmed
- Pre-applied lubricant on some models (activated with a 5 mL water flush)
- Radiopaque - visible on X-ray to confirm placement
- Designed to resist collapse when checking gastric residual

- Pfenninger & Fowler's Procedures for Primary Care, p. 1420-1421
2. Nasojejunal (NJ) Tube / Nasoduodenal Tube
- Same construction as the fine-bore feeding tube but positioned beyond the pylorus into the jejunum (or duodenum)
- The weighted tip and gravity, combined with peristalsis and right-decubitus positioning, facilitate passage
- Metoclopramide (10 mg IV) or erythromycin (3 mg/kg IV) can be used to aid passage past the pylorus
- May require endoscopic or fluoroscopic guidance if positioning fails
Why feed into the jejunum? Jejunal feeding reduces gastroesophageal reflux and aspiration risk. Normally ~20% of gastric antral contents pass into the duodenum with 80% refluxing back - positioning the tube tip in the mid-jejunum (not just the proximal duodenum) is needed to meaningfully reduce aspiration risk.
3. Percutaneous Endoscopic Gastrostomy (PEG) Tube
For long-term feeding (>4 weeks) when the stomach is directly accessed through the abdominal wall.
Structural parts:
| Part | Description |
|---|---|
| External bumper/flange | Flat disc on the outside of the abdominal wall; prevents the tube from slipping inward |
| Tube body | Flexible silicone or polyurethane shaft passing through the abdominal wall into the stomach |
| Internal retention device | Either a mushroom/de Pezzer head (original PEG) that deforms to pass through the tract or a balloon (filled with water, 3-10 mL) that holds the tube against the stomach wall |
| Feeding port | Proximal opening for attaching the feeding set |
| Medication/irrigation port | Separate port on some models |
| Balloon inflation port | On balloon-type tubes; used to inflate/deflate the internal balloon |
Placement: Done endoscopically under local anesthesia and sedation - no surgical incision required. - Roberts & Hedges', p. 968
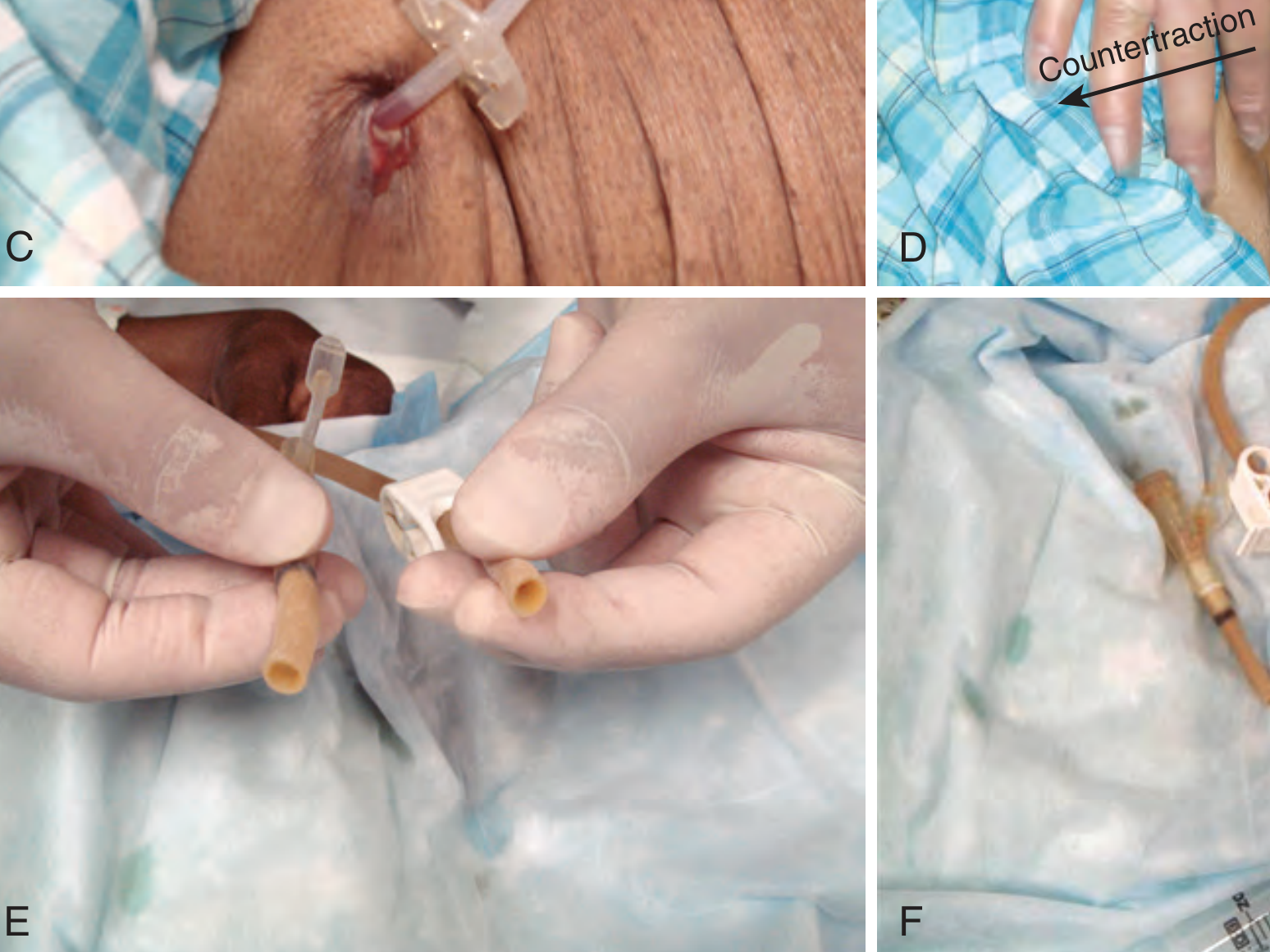
Original vs. Replacement tubes:
- Original PEG = mushroom head (non-balloon) - requires traction/countertraction or endoscopic removal
- Replacement PEG = balloon-type - much easier to change; simply deflate the balloon and slide out
4. PEG-J Tube (Gastro-Jejunal)
- A single entry through the stomach wall (like a PEG) but the inner tube extends through the pylorus into the jejunum
- Has two separate lumens - one for gastric venting/decompression and one for jejunal feeding
- Used when gastric feeding is not tolerated (gastroparesis, severe reflux)
5. Surgical Jejunostomy (J-Tube)
- Inserted directly through the abdominal wall into the small bowel (not via the stomach)
- Requires a surgical incision under general anesthesia - results in a surgical scar at the insertion site
- Used when the stomach is inaccessible or must be bypassed (e.g., after gastrectomy)
- Reduces aspiration compared to gastric feeding but tolerance can be lower (diarrhea risk)
Structural Parts Common to All Feeding Tubes
| Component | Function |
|---|---|
| Tube body | Flexible conduit made of polyurethane, silicone, or PVC; the shaft through which feed travels |
| Distal tip | Sits inside the target organ (stomach/jejunum); may be open-ended or have side ports |
| Side ports/eyes | Small openings near the tip for drainage or infusion; spread flow to reduce mucosal trauma |
| Weighted tip (fine-bore) | Tungsten or mercury weight aids gravitational passage into the small bowel |
| Stylet/guidewire | Temporary stiffening wire inserted through the lumen during placement; removed before use |
| Proximal connector/port | Standardized fitting (ENFit or legacy) that connects to feeding sets, syringes, or pumps |
| Feed clamp | Clamps the tube to stop flow when not feeding |
| External fixator/nose clip | Secures the tube to the nose (nasal tubes) or abdominal wall (transabdominal tubes) |
| Centimeter markings | Depth markings on the tube to confirm correct placement depth |
| Radiopaque stripe | Embedded barium or radiopaque material to make the tube visible on X-ray |
How It Works: The Feeding Process
- Placement - The tube is passed through the nose (or abdominal wall) and advanced to the target site
- Placement confirmation - Chest/abdominal X-ray is mandatory before starting feeds; auscultation alone is unreliable and can be misleading
- Feed initiation - Feeding typically starts at 10-20 mL/hour and is increased gradually to prevent refeeding syndrome in malnourished patients
- Delivery method - Feed is delivered via:
- Gravity drip - feed bag hung above patient
- Enteral pump - programmable pump controls rate precisely
- Bolus feeding - syringe-driven bolus over 15-30 min (mimics meal timing; used for stable patients at home)
- Gastric digestion - Gastric feeding allows normal stomach acid, enzyme mixing, and incremental delivery to the small bowel. Gastric feeding produces better overall digestion than intestinal feeding
- Residual checks - Gastric residual volume is periodically aspirated to check for delayed gastric emptying and aspiration risk
Indications at a Glance
| Tube Type | Route | Indication |
|---|---|---|
| NG (Levin/Salem) | Nasal → Stomach | Short-term decompression, lavage, feeding |
| Fine-bore NG | Nasal → Stomach | Short-to-medium-term enteral feeding |
| NJ / Nasoduodenal | Nasal → Jejunum | High aspiration risk, gastroparesis |
| PEG | Abdominal → Stomach | Long-term feeding (>4 weeks), dysphagia |
| PEG-J | Abdominal → Jejunum | Gastric intolerance + long-term feeding |
| Surgical J-tube | Abdominal → Jejunum | Post-gastrectomy, stomach not available |
Key Contraindications
NG tube contraindications: Skull base fractures (risk of intracranial placement), severe coagulopathy, esophagogastric surgery/perforation, distal bowel obstruction.
PEG tube contraindications: Interposed organs (liver, colon), portal hypertension/varices, ascites, peritoneal metastasis, gastroparesis, gastric outlet obstruction, esophagogastric surgery, limited life expectancy, patient refusal.
- Scott-Brown's Otorhinolaryngology, p. 9025-9086
Common Complications
- Pulmonary misplacement - the most dangerous; tube passes into the trachea/bronchus instead of the esophagus (especially in obtunded patients)
- Esophageal coiling - tube fails to advance; coils in pharynx or esophagus
- Aspiration - feed entering the airway, especially with gastric feeding
- Tube occlusion - lumen blocked by feed residue or medications
- Refeeding syndrome - electrolyte shifts (hypokalemia, hypophosphatemia, hypomagnesemia) when feeding is started too quickly in malnourished patients
- Diarrhea - more common with jejunal feeding or hyperosmolar feeds
Sources:
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, Chapter 40
- Pfenninger & Fowler's Procedures for Primary Care, Chapter 203
- Bailey & Love's Short Practice of Surgery, 28th Ed., Chapter 25
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter on Enteral Tube Feeding
Feeding tube in paediatric
Finding Sources
Finding Sources
Searching the Web
pediatric feeding tube types sizes nasogastric PEG children infants clinical guide
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer on pediatric feeding tubes. Let me compile it.
Feeding Tubes in Paediatrics
Why Paediatrics Is Different
Children are not simply small adults. Several anatomical, physiological, and developmental factors make paediatric tube feeding a distinct clinical domain:
-
Smaller anatomy - nasal passages, nostrils, and GI tract are proportionally much smaller and more easily injured
-
Larger tonsils, adenoids, and tongue relative to airway size, which can obstruct tube passage and increase bleeding risk during insertion
-
Developing feeding skills - premature infants and neonates have not yet developed coordinated sucking and swallowing, making oral feeding temporarily impossible
-
Higher caloric demands per kg - growing children need far more calories per kilogram than adults
-
Different disease spectrum - indications include prematurity, congenital anomalies, failure to thrive, and craniofacial abnormalities that are unique to paediatrics
-
Psychosocial impact - tube feeding affects bonding, oral feeding skill development, and quality of life for both child and family
-
Pfenninger & Fowler's Procedures for Primary Care, p. 1421; Schwartz's Principles of Surgery, 11th Ed.
Anatomy Relevant to Paediatric NG Tube Insertion
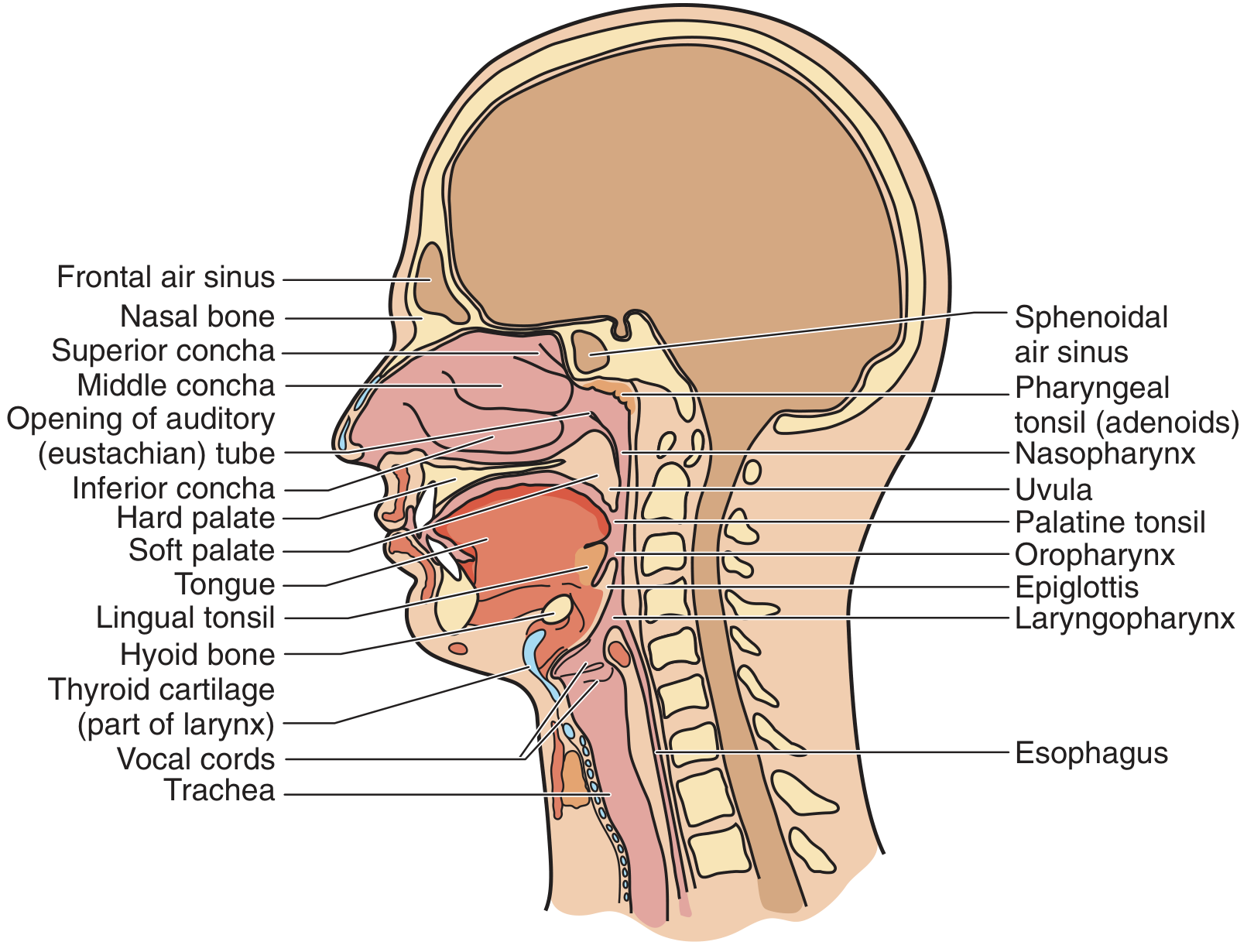
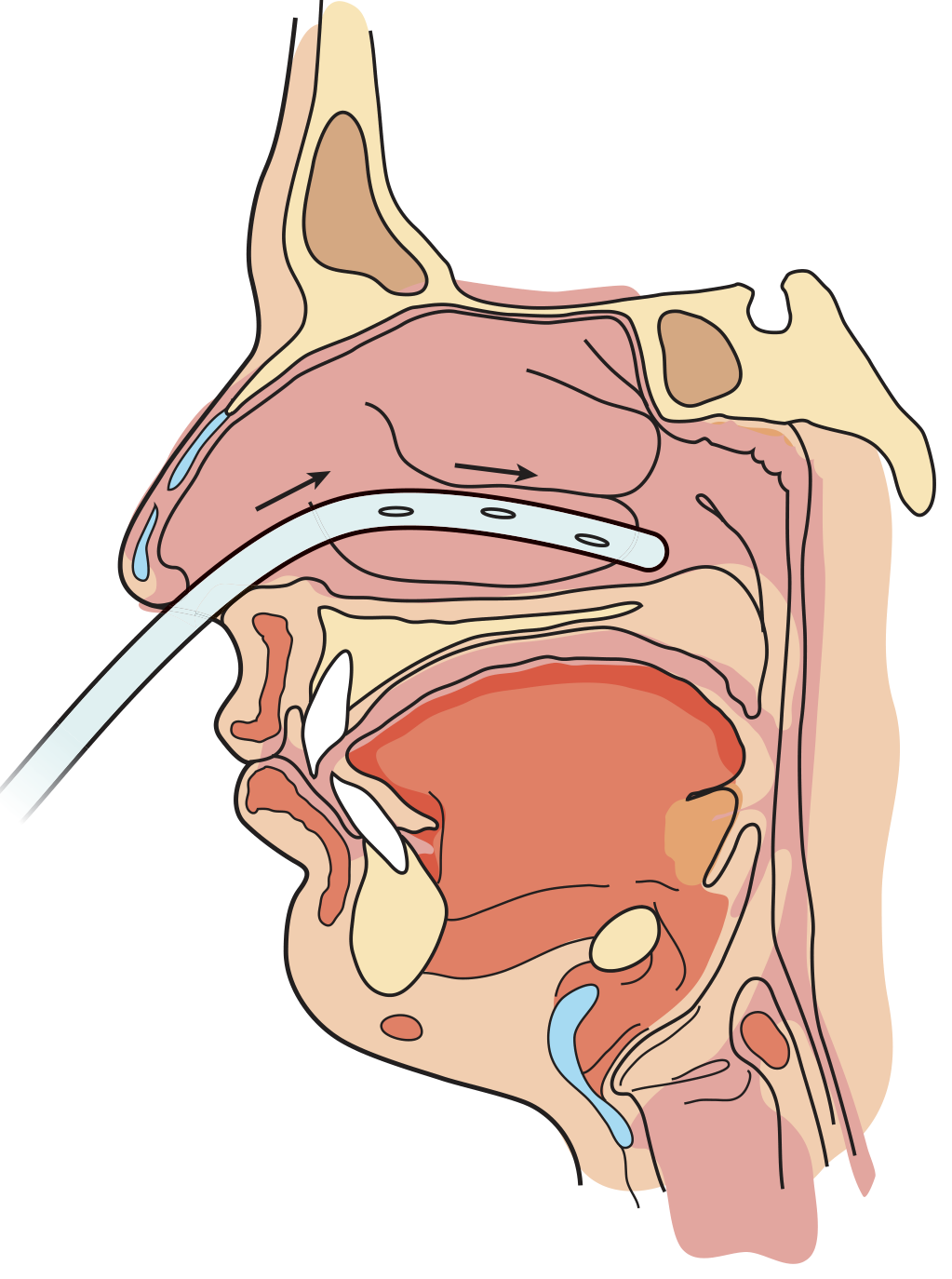
The tube follows this path:
Nostril → nasal floor (inferior meatus) → nasopharynx → oropharynx → esophagus → stomach (or jejunum)
In children, the key anatomical differences are:
- Larger pharyngeal tonsils (adenoids) and palatine tonsils narrow the nasopharyngeal passage
- The tongue is proportionally large and may push into the oropharynx
- Soft tissues are easily injured, making hemorrhage a more significant risk
- Limiting tube size to match the smallest nostril dimension is essential
Tube Sizing in Paediatrics
Tube size is measured in French (Fr) gauge - the larger the number, the wider the tube.
| Patient Group | Recommended NG Tube Size |
|---|---|
| Adults | 16-18 Fr (Salem sump) |
| Children | 10 Fr |
| Nasoenteric feeding tubes (all ages) | 5-12 Fr (fine-bore) |
| Premature/small neonates | 5-6 Fr (ultra fine-bore) |
-
Smaller tubes (5-8 Fr) are more comfortable and less likely to become occluded - preferred for prolonged feeding
-
Larger tubes (12 Fr) should only be used short-term as they are more uncomfortable and more prone to blockage
-
Tube length must also be proportionally shorter - the insertion depth is estimated by measuring from the ear to the nose, then extending to 6 inches below the xiphoid (or 8-10 inches for nasoenteric tubes)
-
Pfenninger & Fowler's, p. 1422
Types of Feeding Tubes Used in Paediatrics
1. Nasogastric (NG) Tube
The most common type in children. Passes through the nose into the stomach.
Uses in paediatrics:
- Premature neonates who cannot coordinate suck-swallow
- Short-term supplemental feeding (illness, post-surgery)
- Gastric decompression (bowel obstruction, ileus)
- Drug/formula administration
- Gastric lavage (poisoning)
Key features for children:
- Fine-bore silicone or polyurethane preferred for comfort
- 10 Fr as standard for children (vs 16-18 Fr for adults)
- Orogastric (OG) route - through the mouth - is preferred in neonates who are obligate nasal breathers, as an NG tube can significantly obstruct airflow through their narrow nasal passages
2. Orogastric (OG) Tube
- Passed through the mouth into the stomach
- Preferred in neonates and young infants (obligate nasal breathers) where nasal obstruction by an NG tube could cause respiratory compromise
- Also safer when nasal route is contraindicated (choanal atresia, skull base fractures)
- Less comfortable for conscious older children, so less used beyond the neonatal period
3. Nasojejunal (NJ) Tube
- Fine-bore tube advanced past the pylorus into the jejunum
- Used when gastric feeding is not tolerated (e.g., severe gastroparesis, high aspiration risk, severe reflux)
- In children, position is usually confirmed by fluoroscopy
- Reduces aspiration and reflux but requires more precise monitoring
4. Gastrostomy Tube (G-tube / PEG)
For long-term feeding (typically >4-6 weeks) when the nasal route is impractical or harmful.
Indications in paediatrics:
- Neurological conditions (cerebral palsy, brain injury) with chronic dysphagia
- Craniofacial anomalies (cleft palate, Pierre Robin sequence) impairing oral feeding
- Congenital heart disease with high metabolic demand
- Premature infants with prolonged feeding difficulties
- Failure to thrive not resolving with NG feeding
Structure and parts (same as adult PEG but smaller gauge):
- External bumper (skin disc) holds tube outside the abdomen
- Tube body passes through abdominal wall into the stomach
- Internal retention device: balloon type (easiest replacement) or mushroom/button type
- Feeding port + medication port proximally
Balloon Gastrostomy Button ("Mickey Button"):
A low-profile device sitting flush against the skin with no external tube - popular for children because it is less visible, less likely to be accidentally pulled, and allows greater physical activity. A separate extension set is attached at feeding times and detached afterward.
5. Jejunostomy (J-tube)
-
Tube enters the abdominal wall directly into the jejunum (bypasses the stomach entirely)
-
Used surgically after gastric procedures, severe gastroparesis, or when the stomach is unavailable
-
In the paediatric surgical neonate (e.g., gastroschisis, intestinal atresia, necrotizing enterocolitis), this is sometimes the only viable enteral route
-
Schwartz's Principles of Surgery, p. 1735-1736; Kaplan & Sadock's Psychiatry
Paediatric Indications for Tube Feeding
| Clinical Situation | Preferred Tube |
|---|---|
| Premature neonate (<34 weeks), undeveloped suck | OG or NG (5-6 Fr) |
| Neurological dysphagia (cerebral palsy) | G-tube or PEG |
| Craniofacial anomalies (cleft palate, Pierre Robin) | NG short-term → G-tube |
| Congenital heart disease (high metabolic need) | NG or G-tube |
| Failure to thrive | NG or G-tube |
| Gastroschisis / intestinal atresia (post-op) | NJ or J-tube |
| Bowel obstruction / ileus (decompression) | NG |
| Gastric aspiration risk / severe reflux | NJ tube |
| Feeding disorder with behavioral component | NG short-term, specialist input |
- Schwartz's Surgery, p. 1735; Kaplan & Sadock's, p. 2563-2571
Nutritional Requirements by Age Group
This is critical in paediatrics - children have far higher caloric needs per kg than adults, and requirements change rapidly with growth:
| Age | Calories (kcal/kg/day) | Protein (g/kg/day) |
|---|---|---|
| 0-6 months | 100-120 | 2.0 |
| 6 months-1 year | 100 | 1.5 |
| 1-3 years | 100 | 1.2 |
| 4-6 years | 90 | 1.0 |
| 7-10 years | 70 | 1.0 |
| 11-14 years | 55 | 1.0 |
| 15-18 years | 45 | 1.0 |
- Schwartz's Principles of Surgery, Table 39-1, p. 1736
Feed Formulas in Paediatrics
Unlike adults (who receive standard 1-2 kcal/mL enteral formulas), children require age-specific formulas. Neonates, especially premature ones, have distinct needs:
| Formula | kcal/mL | Protein (g/mL) | Fat (g/mL) | Carbohydrate (g/mL) |
|---|---|---|---|---|
| Human milk | 0.67 | 0.011 | 0.040 | 0.070 |
| Enfamil 20 (milk-based) | 0.67 | 0.015 | 0.038 | 0.069 |
| Similac 20 (milk-based) | 0.67 | 0.015 | 0.036 | 0.072 |
| Prosobee (soy-based) | 0.67 | 0.020 | 0.036 | 0.070 |
| Pregestimil (hydrolysed) | 0.67 | 0.019 | 0.028 | 0.091 |
| Alimentum (hydrolysed) | 0.67 | 0.019 | 0.038 | 0.068 |
| Enfamil Premature (preterm) | 0.80 | 0.024 | 0.041 | 0.089 |
-
Premature formula (0.80 kcal/mL) is more calorie-dense because preterms need extra energy for catch-up growth and have limited gastric capacity
-
Hydrolysed formulas (Pregestimil, Alimentum) are used when the infant has malabsorption or cow's milk protein intolerance
-
Human milk is always preferred when available
-
Schwartz's Surgery, Table 39-2, p. 1736
Insertion Technique: Key Paediatric Differences
Measuring Insertion Depth
The standard adult measurement (nose to ear to xiphoid) is adapted for children. The estimated tube length at the nose:
- NG tube: nose to ear + nose to xiphoid + 6 inches below xiphoid
- The nasal septum to tracheoesophageal junction is about 8 inches in adults; this distance is proportionally shorter in children
Challenges in Children
- No ability to cooperate (infants, young children) - ask the child to swallow; if they cannot, induce swallowing with a small amount of water in the mouth or through the tube
- Restrain hands of young/uncooperative children to prevent tube removal
- Never force - if significant resistance, respiratory distress, or nasal hemorrhage occurs, stop immediately and withdraw the tube
- In intubated patients, tube passage may be the hardest; a second ET tube as a conduit can be used if oral route is needed
Confirming Placement
- X-ray confirmation is mandatory before feeding begins - auscultation alone is unreliable
- In neonatal units, pH testing of aspirate (pH <5.5 confirms gastric position) may be used to reduce radiation exposure, per local protocol
- Check the carina level on CXR - a tracheally placed tube deviates sharply at the carina into the right or left bronchus
Complications Specific to Paediatrics
| Complication | Paediatric Specifics |
|---|---|
| Pulmonary misplacement | More common in neonates with absent cough reflex; potentially fatal if formula infused into lung |
| Nasal hemorrhage | Higher risk due to proportionally large, soft, vascular nasal mucosa and adenoids |
| Tube coiling in oropharynx | More common in young children with large tongues and tonsils |
| Aspiration | Neonates at higher risk due to poor gag reflex and supine position |
| Refeeding syndrome | Risk in malnourished infants - start feeds slowly and monitor electrolytes (K⁺, PO₄, Mg²⁺) |
| TPN-associated cholestasis | Specific to neonates on prolonged parenteral nutrition - prevented by introducing even minimal enteral feeds as early as possible |
| Accidental decannulation | Children (especially toddlers) often pull tubes out - may need mittens or elbow restraints |
| Granulation tissue at G-tube site | Common in children with PEG/gastrostomy - treated with silver nitrate or topical steroids |
When to Use Enteral vs. Parenteral Nutrition
In paediatric surgical patients, the principle is unambiguous: enteral nutrition is always preferred when the GI tract is functional, because it:
- Promotes growth and function of the GI system
- Ensures the infant continues to learn and develop oral feeding skills
- Prevents parenteral nutrition-associated cholestasis (a major cause of liver failure in long-term TPN neonates)
Parenteral nutrition is used only when enteral feeding is mechanically, ischemically, or functionally impossible - and even then, minimal enteral (trophic) feeds should be started as early as possible to stimulate gut maturation.
- Schwartz's Principles of Surgery, p. 1735
Summary Table: Adult vs. Paediatric Feeding Tube Comparison
| Feature | Adult | Paediatric |
|---|---|---|
| Standard NG tube size | 16-18 Fr | 10 Fr |
| Fine-bore feeding tube | 8-12 Fr | 5-8 Fr |
| Preferred route in neonates | Nasal | Oral (orogastric) |
| Insertion cooperation | Usually possible | Often impossible; restraint may be needed |
| Caloric needs | 25-35 kcal/kg/day | 45-120 kcal/kg/day depending on age |
| Formula | Standard 1-2 kcal/mL | Age/condition-specific; premature formulas 0.8 kcal/mL |
| Long-term tube | PEG | PEG or gastrostomy button (Mickey button) |
| Key complication concern | Aspiration, misplacement | Misplacement, hemorrhage, oral feeding skill regression |
Sources:
- Pfenninger & Fowler's Procedures for Primary Care, 3rd Ed., Chapter 203
- Schwartz's Principles of Surgery, 11th Ed., Chapter 39 (Pediatric Surgery)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry (Feeding Disorders in Early Childhood)
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, Chapter 40
Foleys catheter details of different parts and its use also in paediatric uses
Finding Sources
Finding Sources
Searching the Web
Foley catheter parts structure balloon lumen tip paediatric sizing French gauge clinical use
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
I now have excellent content from multiple authoritative textbooks. I have the procedural steps, catheter anatomy, complications, and clinical use. Let me now generate a comprehensive, well-illustrated answer.
Foley Catheter: Parts, Structure, and Use - Including Paediatric Applications
What Is a Foley Catheter?
A Foley catheter (also called an indwelling urethral catheter or retention catheter) is a flexible tube inserted through the urethra into the bladder to continuously drain urine. It is held in place by a small balloon inflated with water inside the bladder - this is the defining feature that distinguishes it from a simple straight catheter.
It was named after American urologist Frederic Foley, who designed the self-retaining balloon catheter in the 1930s.
Anatomy: The Path the Catheter Takes
Male path: External urethral meatus → penile urethra → bulbar urethra → membranous urethra → prostatic urethra → bladder neck → bladder
Female path: External urethral meatus (shorter, ~4 cm) → urethra → bladder
Detailed Anatomy of a Foley Catheter: All Parts
External (Proximal) End - Outside the Patient
| Part | Description |
|---|---|
| Funnel-shaped proximal end | The wide open end connecting to the drainage bag or syringe |
| Drainage port (main lumen port) | The large opening where urine drains out; connects via tubing to a urine collection bag |
| Balloon inflation port | A smaller, separate port (usually colour-coded, e.g., blue or red) used to inflate and deflate the retention balloon with sterile water using a syringe |
| Valve/self-sealing valve | On the inflation port; prevents water escaping after balloon is inflated |
| Third port (3-way catheters only) | Additional port for continuous bladder irrigation (e.g., post-TURP) |
| External clamp | Used to clamp the drainage lumen when needed |
Tube Body (Shaft)
| Feature | Detail |
|---|---|
| Material | Latex (standard), silicone (latex-free, for allergy), silicone-coated latex, hydrogel-coated (for long-term use) |
| Size | Measured in French (Fr) gauge - 1 Fr = 0.33 mm diameter |
| Length | ~40 cm (standard); paediatric versions are shorter |
| Lumens | 2-way (most common) or 3-way (for irrigation) |
| Centimetre markings | Depth markings along the shaft to confirm insertion depth |
| Radiopaque stripe | Embedded line visible on X-ray to confirm position |
Internal (Distal) End - Inside the Bladder
| Part | Description |
|---|---|
| Tip | Rounded, atraumatic tip that enters the bladder first |
| Drainage eye (side ports) | One or two openings just proximal to the balloon, through which urine enters the catheter lumen to drain |
| Retention balloon | Sits just above the tip; inflated after confirmed bladder entry; holds the catheter in place at the bladder neck. Standard sizes: 5 mL (paediatric) or 10-30 mL (adult) |
Lumen Configurations
2-Way (Two-Lumen) Foley - Most Common
Port 1: Drainage lumen → urine drains out
Port 2: Balloon lumen → inflated to retain catheter
Used for: standard urinary drainage, urinary retention, monitoring urine output, post-op care, immobile patients.
3-Way (Three-Lumen) Foley
Port 1: Drainage lumen → urine drains out
Port 2: Balloon lumen → inflated to retain catheter
Port 3: Irrigation lumen → sterile saline flows IN continuously
Used for: continuous bladder irrigation after transurethral resection of the prostate (TURP) or other bladder surgery, to prevent clot formation and maintain catheter patency.
Catheter Sizes: French Gauge Reference
| French (Fr) Size | Outer Diameter | Common Use |
|---|---|---|
| 5 Fr | 1.7 mm | Neonates / premature infants |
| 6 Fr | 2.0 mm | Neonates / small infants |
| 8 Fr | 2.7 mm | Infants / young children |
| 10 Fr | 3.3 mm | Young children (2-5 years) |
| 12 Fr | 4.0 mm | Older children (5-10 years) |
| 14 Fr | 4.7 mm | Adolescents / women |
| 16 Fr | 5.3 mm | Standard adult women |
| 18 Fr | 6.0 mm | Standard adult men |
| 20-24 Fr | 6.7-8.0 mm | Haematuria / clot evacuation |
Standard adult male catheterization uses a 14F to 18F Foley catheter. If a standard Foley fails (e.g., due to urethral stricture or prostatic enlargement), a coudé catheter (firmer, angled tip) may be tried.
- Tintinalli's Emergency Medicine, 7th Ed., Chapter 92
Types of Foley Catheter
| Type | Key Feature | Use |
|---|---|---|
| Standard 2-way Foley | Two lumens | Urinary drainage, retention |
| 3-way irrigation Foley | Three lumens | Post-TURP, haematuria with clots |
| Coudé catheter | Angled curved tip | BPH, urethral stricture, difficult catheterization |
| Silicone Foley | Latex-free | Latex allergy, long-term use |
| Hydrogel-coated Foley | Slippery coating | Long-term indwelling (reduces infection, encrustation) |
| Antimicrobial-coated | Silver alloy or nitrofurazone | ICU, CAUTI prevention |
| Suprapubic catheter | Enters via abdominal wall | When urethral route not possible |
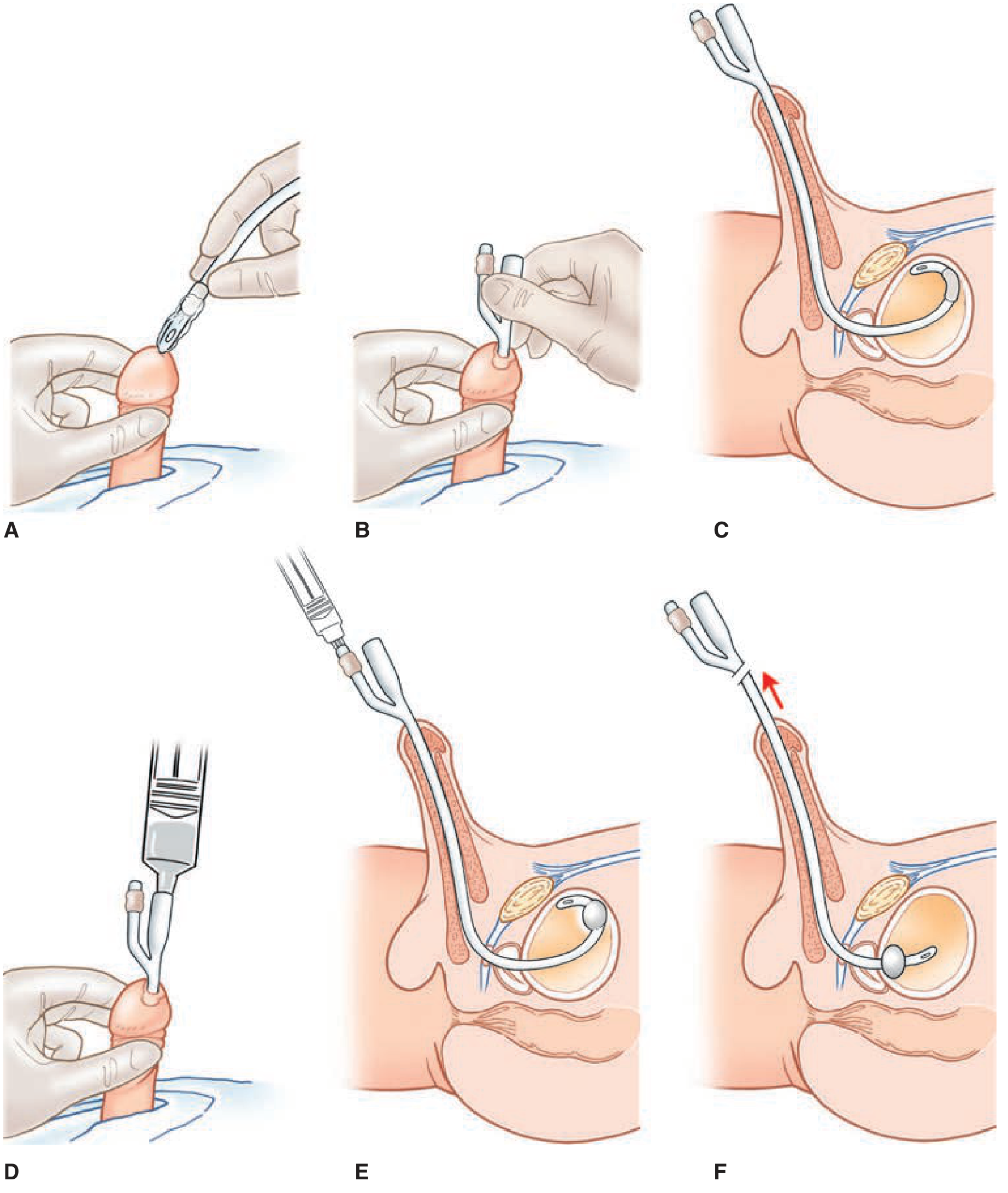
How It Works: Step by Step
Step 1 - Preparation:
Anesthetic lubricant (2% lidocaine jelly, 10-15 mL) injected into the urethra 5-10 minutes before insertion. In males, retract foreskin if uncircumcised.
Step 2 - Insertion:
Insert the lubricated catheter horizontally into the meatus. In males, hold the penis at 90° (perpendicular to body) to straighten the penile urethra.
Step 3 - Advance:
Gently advance until the catheter bifurcation (the proximal Y-junction) is at the meatus - this confirms the tip is well inside the bladder, not just at the bladder neck.
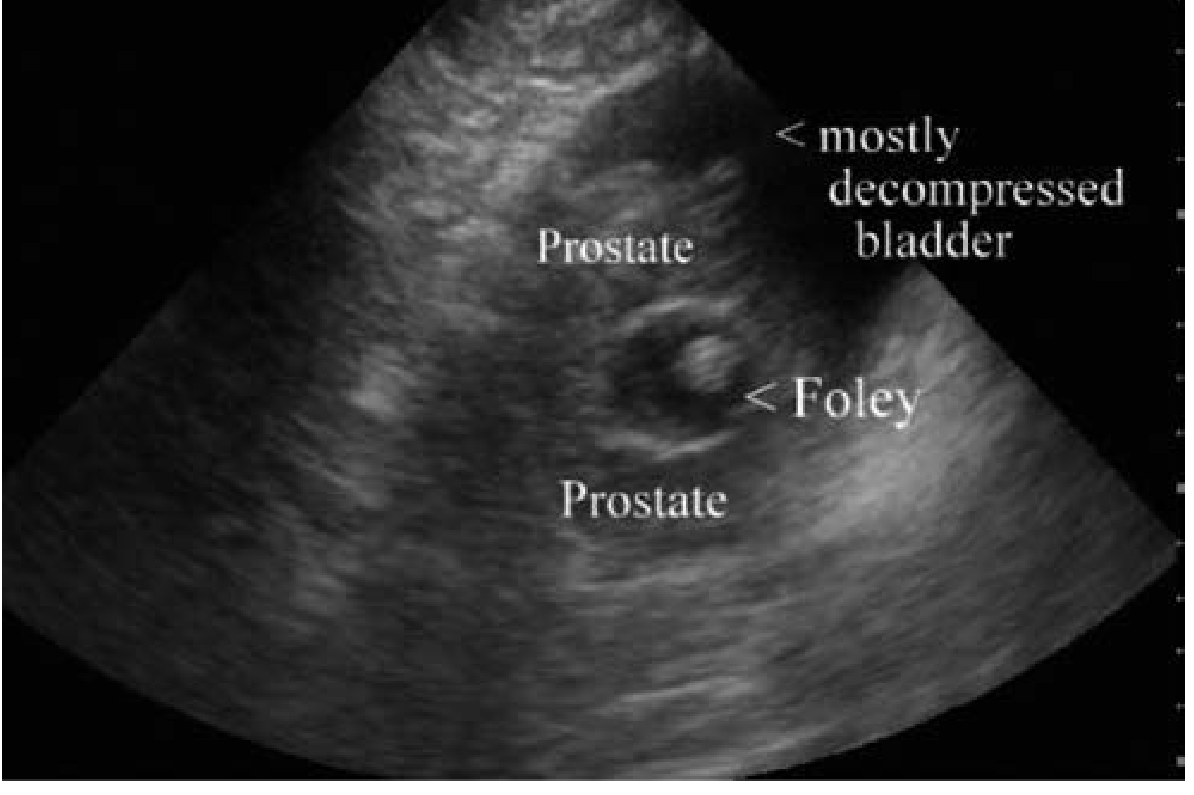
Step 4 - Confirm placement:
Urine freely flows back through the drainage lumen - this confirms bladder entry.
Step 5 - Inflate balloon:
Inflate the retention balloon with sterile water (NOT saline, which can crystallize in the valve):
- 5-10 mL for adult (10 mL balloon)
- 3-5 mL for paediatric
- Never inflate before urine return - inflating in the urethra causes severe pain and urethral injury
Step 6 - Seat at bladder neck:
Gently pull back on the catheter until slight resistance is felt - the balloon seats against the bladder neck, securing the catheter.
Step 7 - Connect drainage bag:
Connect to a closed sterile drainage system (leg bag for mobile patients, bedside bag for immobile/inpatient).
Step 8 - Secure to thigh:
Tape or strap catheter to inner thigh to prevent traction-related urethral injury.
Clinical Indications for Foley Catheterization
Therapeutic
- Acute urinary retention - the primary indication; provides immediate bladder decompression
- Chronic urinary retention (neurogenic bladder, spinal cord injury)
- Perioperative monitoring - accurate hourly urine output measurement in surgery/ICU
- Immobile patients - prevention of skin breakdown from urinary incontinence
- Bladder irrigation after prostate/bladder surgery (3-way catheter)
- Bladder decompression before abdominal procedures (e.g., before paracentesis, laparotomy)
- Urethral obstruction bypass (stricture, BPH, tumour)
Diagnostic
- Urine specimen collection for culture (especially in women/children where clean-catch is unreliable)
- Voiding cystourethrography (VCUG) - catheter fills bladder with contrast for imaging
- Urodynamic studies - measuring bladder pressures
- Measure post-void residual volume
Causes of Urinary Retention Requiring Catheterization
| Category | Examples |
|---|---|
| Obstructive (Men) | BPH, prostate cancer, phimosis, meatal stenosis, urethral stricture |
| Obstructive (Women) | Cystocele, uterine/ovarian tumour, pelvic organ prolapse |
| Neurogenic | Spinal cord injury, MS, Parkinson's, cauda equina syndrome, diabetes |
| Pharmacological | Anticholinergics, opiates, alpha-agonists, antidepressants, antihistamines |
| Post-operative | Epidural anaesthesia, post-surgery bleeding/clots |
| Traumatic | Urethral/bladder injury |
| Paediatric-specific | Posterior urethral valves, rhabdomyosarcoma of bladder, urethral atresia |
- Tintinalli's Emergency Medicine, Tables 92-1 to 92-3
Post-Catheterization Care
After draining a long-standing, large-volume retention (800-1500 mL):
- Monitor for postobstructive diuresis (>200 mL/hour urine output)
- Monitor renal function - may develop postobstructive acute kidney injury
- Monitor electrolytes - especially in prolonged retention
- Antibiotics are NOT routinely given for asymptomatic bacteriuria; reserved for symptomatic UTI
- Alpha-blockers (alfuzosin 10 mg/day, or tamsulosin 0.4 mg/day) can be started to relax the bladder neck and improve the chance of successful voiding when the catheter is eventually removed
Home care:
- Connect to a leg bag during the day (smaller, concealed under clothes)
- Swap to a larger overnight bag at night (greater capacity)
- Clean meatal area daily with soap and water
- Keep drainage bag below bladder level at all times (gravity drainage)
Foley Catheter in Paediatrics
Key Differences in Children
Children require special consideration for catheterization due to:
- Smaller urethral calibre - much smaller bore tubes, extreme care to avoid mucosal trauma
- Proportionally longer urethra relative to body size in males
- Undescended testes, phimosis, hypospadias, epispadias - anatomical variants common in male children
- Psychological distress - catheterization is frightening; appropriate restraint, distraction, and analgesia are essential
- Different disease spectrum - congenital anomalies, posterior urethral valves, neurogenic bladder (spina bifida), trauma
- Smaller balloon volumes - paediatric catheters use 3-5 mL balloons (vs 10 mL in adults)
Paediatric Catheter Sizes by Age
| Age Group | Catheter Size | Balloon Volume |
|---|---|---|
| Premature neonate | 5 Fr feeding tube (no balloon) | N/A |
| Neonate (0-1 month) | 5-6 Fr | 1.5-3 mL |
| Infant (1-12 months) | 6-8 Fr | 3 mL |
| Toddler (1-3 years) | 8-10 Fr | 3-5 mL |
| Child (3-8 years) | 10-12 Fr | 5 mL |
| Child (8-12 years) | 12-14 Fr | 5-10 mL |
| Adolescent | 14-16 Fr (female), 14-18 Fr (male) | 10 mL |
In very young infants or neonates, a feeding tube (5 Fr) without a balloon is sometimes used as a urinary catheter, held in place by taping to the skin rather than a balloon.
Specific Paediatric Indications
| Indication | Notes |
|---|---|
| Posterior urethral valves (PUV) | Most common obstructive uropathy in boys; catheter decompresses bladder acutely; may require valve ablation |
| Neurogenic bladder (spina bifida/myelomeningocele) | Long-term intermittent catheterization (clean intermittent catheterization, CIC) every 4-6 hours; parents and eventually the child perform this themselves |
| Urethral atresia / stenosis | Rare congenital cause; may need surgical dilation before catheterization |
| Rhabdomyosarcoma of bladder | Catheterization for urine output monitoring and diagnosis |
| Urinary tract infection (diagnosis) | Catheter urine specimen is the gold standard in infants <2 years (suprapubic aspiration also used) |
| VCUG (voiding cystourethrogram) | Catheter fills bladder with contrast to diagnose vesicoureteral reflux - very common in paediatric urology workup |
| Post-operative monitoring | Major surgery (cardiac, abdominal, urological) |
| Trauma / spinal cord injury | Acute retention; neurogenic bladder |
| Acute urinary retention | Posterior urethral valves, infection, pelvic mass |
Clean Intermittent Catheterization (CIC) in Children
This is a cornerstone of paediatric urology. Instead of a permanently indwelling Foley catheter, the child (or parent) inserts a straight catheter every 4-6 hours to empty the bladder, then removes it. Benefits over indwelling catheter:
- Dramatically lower infection rates (catheter-associated UTI risk nearly eliminated)
- Preserves bladder capacity and compliance
- Allows normal social activity, schooling, sports
- Children as young as 5-6 years can be taught self-catheterization
- Used lifelong in spina bifida, neurogenic bladder
- Uses straight (non-retention) catheters - no balloon
Paediatric Insertion Technique - Key Differences
Female Children
- Urethral meatus is small and difficult to visualise in infants
- Use good lighting; spread labia gently with non-dominant hand
- Insert catheter ~2-3 cm (infants) to 3-5 cm (children) to reach bladder
- If tube enters vagina - withdraw, do not reuse (contaminated), use a new catheter and redirect
Male Children
- Hold penis perpendicular to body to straighten penile urethra
- In uncircumcised boys, gently retract foreskin only as far as it naturally moves - never force; phimosis is common in young boys
- Phimosis (inability to retract foreskin) requires smaller catheter or occasionally urological assistance
- Advance until urine flows; in young children the bladder neck is close to the surface so depth is short
Sedation / Analgesia
- Topical lidocaine gel (2%) applied to meatus 3-5 minutes before insertion is standard
- Young children and infants may need mild sedation or intranasal midazolam for the procedure
- Oral sucrose (for neonates) reduces procedural pain
- Parent presence/comfort reduces distress significantly
Complications of Foley Catheterization (Adult and Paediatric)
| Complication | Details | Paediatric Specifics |
|---|---|---|
| Catheter-associated UTI (CAUTI) | Most common complication; risk increases with duration | Higher risk in children with neurogenic bladder |
| Balloon inflation in urethra | Severe pain, urethral injury | Critical to confirm urine flow before inflating |
| Urethral trauma / false passage | Forceful insertion; blood at meatus | More risk with phimosis, small meatus |
| Bladder spasm | Sensation of urgency around catheter | Oxybutynin 2.5 mg 2-3x/day can help |
| Catheter migration | Balloon migrates to proximal urethra - causes penile pain | Secure catheter well; check position |
| Bladder calculi | Long-term indwelling catheters - mineral encrustation | Encourage hydration; change catheters regularly |
| Urethral erosion/stricture | Large catheters, long-term use | Use smallest effective size |
| Postobstructive diuresis | After draining large volume retention | Monitor urine output after drainage |
| Haematuria | Trauma of insertion (usually clears) | May require irrigation catheter if clots |
If gross blood and severe pain occur without urine return - deflate balloon immediately and remove. Do NOT reinsert - a false passage may have been created. Seek urological consultation.
Catheter Care and Prevention of CAUTI
- Use closed drainage system at all times
- Keep drainage bag below bladder level (but not on the floor)
- Secure catheter to thigh - prevents traction and urethral trauma
- Clean urethral meatus daily with soap and water
- Change catheter every 4 weeks (latex) or 12 weeks (silicone) if long-term
- Remove catheter as early as clinically possible - the longer it stays in, the higher the infection risk
- Avoid routine antibiotic prophylaxis for asymptomatic bacteriuria (increases resistance)
- In children on CIC - rinse catheters with sterile water; may be reused up to 1 week (per local protocol)
Summary: Adult vs. Paediatric Foley Catheter
| Feature | Adult | Paediatric |
|---|---|---|
| Standard size | 14-18 Fr | 6-12 Fr (age-dependent) |
| Balloon volume | 10-30 mL | 3-5 mL |
| Material | Latex or silicone | Silicone preferred (less trauma) |
| Long-term management | Indwelling catheter | CIC (clean intermittent catheterization) preferred |
| Common indication | BPH, post-op, retention | Posterior urethral valves, neurogenic bladder, VCUG |
| Insertion depth (male) | 15-25 cm | 3-8 cm (age-dependent) |
| Insertion depth (female) | 5-6 cm | 2-4 cm (age-dependent) |
| Sedation needed | Usually not | Often yes (infants, young children) |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Chapter 92 (Urinary Retention)
- Campbell-Walsh-Wein Urology, 3-Volume Set (Catheterization Techniques)
- Pfenninger & Fowler's Procedures for Primary Care, Chapter 110 (Bladder Catheterization)
- Schwartz's Principles of Surgery, 11th Ed. (Paediatric Urology)
- Bailey & Love's Short Practice of Surgery, 28th Ed. (Urological Emergencies)
This is a shared conversation. Sign in to Orris to start your own chat.