Act as an expert Intensivist and Neuro-critical Care Specialist. I am a 1st-year MCh Neurosurgery resident trying to master mechanical ventilation, specifically tailored to neurological injuries (e.g., severe TBI, poor-grade SAH, large MCA infarcts, post-op posterior fossa craniectomies). Please provide a highly structured, evidence-backed breakdown of the following specific topic: [INSERT TOPIC HERE - e.g., Volume Control vs. Pressure Control modes, or Interpreting Flow-Time waveforms for air trapping]. In your breakdown, ensure you address: 1. THE CORE MECHANICS: How this setting/mode/waveform works mechanically on the ventilator (trigger, limit, cycle, variables). 2. INTENSITY & BRAIN PHYSIOLOGY: How these settings directly impact cerebral physiology, specifically: - PaCO2 regulation and its effect on cerebral blood flow (CBF) and Intracranial Pressure (ICP). - Mean Airway Pressure (Pmean) and its impact on venous return, jugular venous bulb saturation, and CPP. 3. WAVEFORM/GRAPHICAL ANALYSIS: Describe exactly what the Pressure-Time, Flow-Time, and Volume-Time waveforms look like under these conditions. Explain how to visually identify patient-ventilator dyssynchrony (e.g., double triggering, flow starvation, auto-PEEP) on the screen. 4. CLINICAL NEUROSURGICAL SCENARIOS: Provide concrete examples of how to set or titrate these parameters in a patient with a tight brain or high ICP, vs. a patient requiring neuroprotection, vs. a post-op patient ready for early weaning. Cite relevant neuro-critical care guidelines or physiological principles where appropriate. Use clear formatting, bullet points, and clinical reasoning. Topic is basics of ventilator settings with physiology and with examples of pt. Related to neurosx
"mechanical ventilation" AND "traumatic brain injury" AND "intracranial pressure"
"lung protective ventilation" AND "neurological injury" AND "cerebral perfusion"
"ventilator settings" AND "cerebral perfusion pressure" AND "neurocritical care"
PMID: 41082009
"PEEP" AND "intracranial pressure" AND "cerebral perfusion"
PMID: 40982016
PMID: 38681785
brain protective ventilation neurocritical care 2024 2025 guidelines TBI SAH PaCO2 PEEP ICP
Mechanical Ventilation Fundamentals for the Neurosurgical ICU
A Structured Reference for MCh Neurosurgery Residents
Evidence base: Barash Clinical Anesthesia 9e | Roberts & Hedges Clinical Procedures in EM | Rosen's Emergency Medicine | Bradley & Daroff's Neurology in Clinical Practice | Fishman's Pulmonary Diseases | Sabiston's Surgical Textbook | Goldman-Cecil Medicine | Iavarone et al., Intensive Care Med 2025 (PMID 40982016) | Zunino et al., J Intensive Med 2024 (PMID 38681785) | Al Sharie et al., Curr Neurol Neurosci Rep 2025 (PMID 41082009)
PART I: THE CORE MECHANICS OF MECHANICAL VENTILATION
1.1 The Four Variables Framework (Trigger - Limit - Cycle - Baseline)
| Variable | Definition | Clinical Relevance |
|---|---|---|
| Trigger | What initiates the breath | Pressure trigger (-1 to -2 cmH2O) or flow trigger (1-3 L/min); patient-triggered = assisted breath; time-triggered = controlled breath |
| Limit | What is held constant DURING inspiration | In VC: flow is limited (constant); in PC: pressure is limited (constant) |
| Cycle | What terminates inspiration | Volume-cycled: set VT reached; Pressure-cycled: set inspiratory time (Ti) expires; PSV: flow drops to % of peak |
| Baseline | End-expiratory pressure | PEEP — the "floor" of the respiratory cycle |
1.2 Volume Control Ventilation (VCV)
- Trigger: Patient effort or time
- Limit: Flow is constant (square wave pattern by default)
- Cycle: Set tidal volume is delivered; ventilator delivers whatever pressure is needed
- What the clinician controls: VT (mL/kg IBW), RR, PEEP, FiO2, flow rate (L/min), I:E ratio
- What varies: Peak airway pressure (Ppeak), plateau pressure (Pplat)
- Key advantage for neuro patients: Guarantees minute ventilation (MV = VT x RR), thus guarantees PaCO2 targeting - critical in TBI/SAH
- Key risk: If compliance falls (brain-lung crosstalk, neurogenic pulmonary edema), Ppeak rises without warning
1.3 Pressure Control Ventilation (PCV)
- Trigger: Patient effort or time
- Limit: Inspiratory pressure is constant throughout the set inspiratory time (Ti)
- Cycle: Set Ti expires (time-cycled)
- What the clinician controls: Inspiratory pressure (above PEEP), RR, Ti, PEEP, FiO2
- What varies: Tidal volume (VT changes with compliance and resistance)
- Key advantage: Decelerating flow waveform improves gas distribution, limits overdistension, potentially better for neurogenic pulmonary edema
- Key risk for neuro patients: If airway secretions accumulate or compliance drops, VT decreases silently - you can lose minute ventilation and PaCO2 can rise, causing cerebral vasodilation and ICP spikes
1.4 Pressure Support Ventilation (PSV)
- Trigger: Patient effort only (flow or pressure)
- Limit: Pressure
- Cycle: When inspiratory flow drops to ~25% of peak flow (flow-cycled)
- Baseline: PEEP
- Role in neuro: Used for weaning when patient is making reliable respiratory effort; contraindicated if patient has unreliable drive (GCS <8, brainstem injury, Cheyne-Stokes)
1.5 Assist-Control (AC) Mode
- Every breath triggered by the patient reaches the full set target (VT in AC-VC, or pressure in AC-PC)
- The ventilator delivers a backup rate if the patient doesn't trigger
- Preferred mode in acute neuro-critical patients - ensures minimum MV regardless of neurological state
1.6 SIMV (Synchronized Intermittent Mandatory Ventilation)
- Mandatory breaths are delivered at set rate; spontaneous breaths between them receive only PSV
- Falls out of favor in acute neuro because partial support may increase WOB and cause dyssynchrony
- Appropriate in late-stage weaning
1.7 Initial Settings Cheatsheet for Neuro ICU
| Parameter | Target | Notes |
|---|---|---|
| Mode | AC-VC (default) | Guarantees MV; switch to AC-PC if plateau pressures are high |
| VT | 6-8 mL/kg IBW | Lung-protective; 6 mL/kg for concurrent ARDS |
| RR | 12-18 breaths/min | Titrate primarily to PaCO2 |
| PEEP | 5 cmH2O (default) | Individualize based on ICP response (see Part II) |
| FiO2 | Start 1.0, wean to SpO2 94-98% | Avoid hyperoxia (PaO2 > 150 causes ROS injury) |
| Pplat | < 30 cmH2O | Mandatory target to avoid VILI |
| Driving pressure | < 15 cmH2O (Pplat - PEEP) | Best surrogate for VILI risk |
| I:E ratio | 1:2 (default) | Increase expiratory time if air trapping |
PART II: VENTILATION AND BRAIN PHYSIOLOGY
2.1 PaCO2 and Its Effect on CBF and ICP
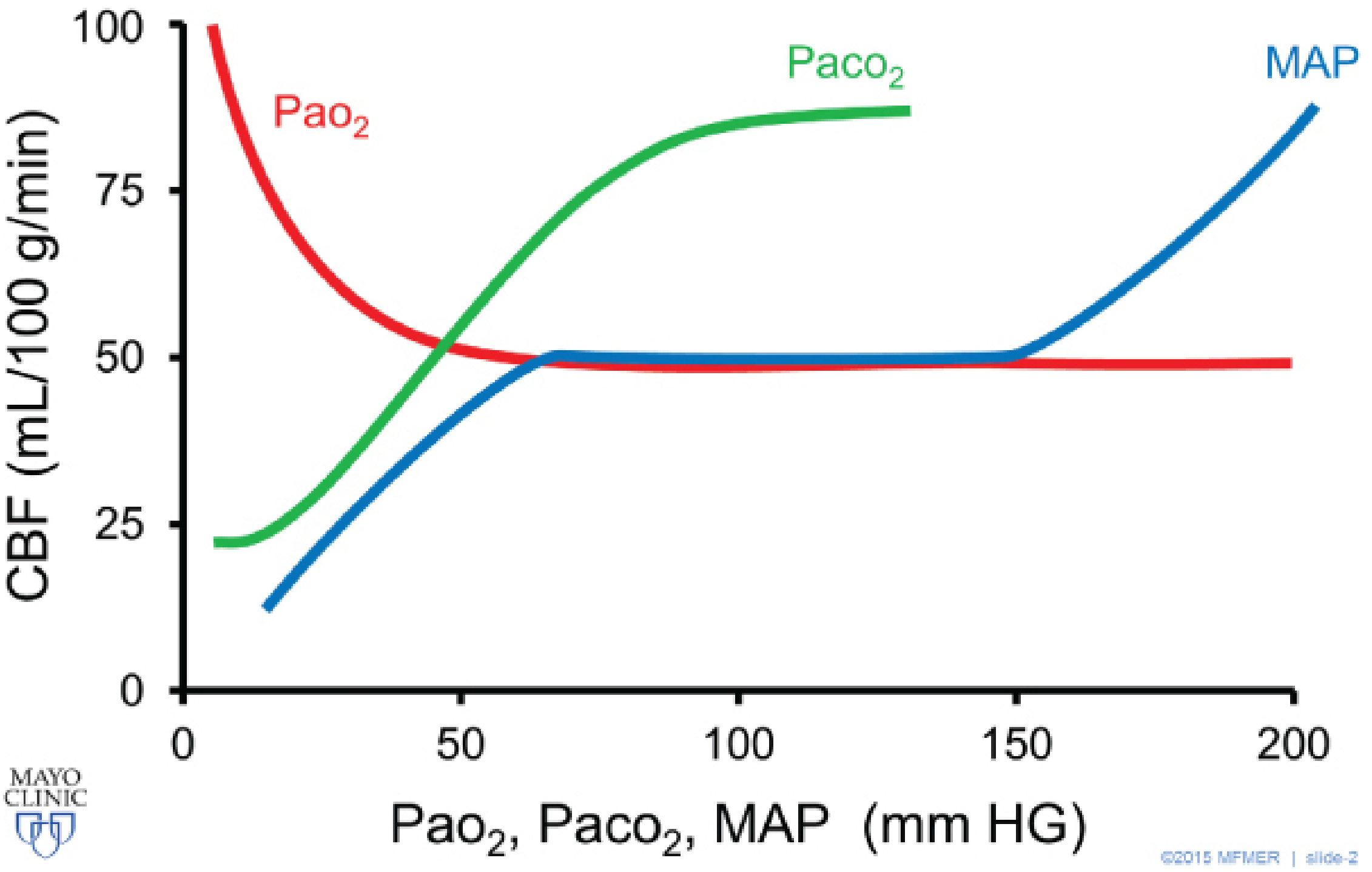
- CO2 is the most potent vasoactive agent in the cerebral circulation
- PaCO2 causes cerebral vasodilation - raising CBF ~1-2 mL/100g/min per mmHg rise in PaCO2
- Hypocapnia causes cerebral vasoconstriction - reducing CBF and thus cerebral blood volume (CBV)
- Since CBV contributes to intracranial volume, hyperventilation reduces ICP within 30-120 seconds
Intracranial Volume = Brain parenchyma + CSF + CBV
CBV is modified by PaCO2 → the ONLY ventilator-modifiable Monroe-Kellie component
- Each 1 mmHg decrease in PaCO2 → ~3% decrease in CBF
- Lowering PaCO2 from 40 to 30 mmHg → ~30% decrease in CBF → significant ICP reduction
| PaCO2 Target | Effect on ICP | Effect on CBF | Risk |
|---|---|---|---|
| 35-40 mmHg | Normal | Normal (~50 mL/100g/min) | None |
| 30-35 mmHg | Moderate reduction | Reduced ~15-20% | Borderline ischemia in vulnerable zones |
| 25-30 mmHg | Significant reduction | Reduced ~30-40% | Ischemia, worsens outcome if sustained |
| < 25 mmHg | Maximum acute reduction | Reduced > 50% | High ischemia risk, CONTRAINDICATED routinely |
- "Hyperventilation (PaCO2 of 25 mmHg or less) is not recommended routinely"
- "Hyperventilation should be avoided during the first 24 hours after TBI, when CBF is already critically low"
- Prophylactic hyperventilation is harmful; therapeutic hyperventilation (PaCO2 30-35 mmHg) is a BRIDGE, not a treatment - use only until definitive ICP reduction (mannitol, CSF drainage, surgery) is implemented
2.2 PaO2 and Oxygenation Targets
- CBF rises sharply as PaO2 falls below ~50 mmHg - a protective vasodilatory response that increases ICP
- Hyperoxia (PaO2 > 150-200 mmHg) does not further reduce CBF but generates reactive oxygen species (ROS) that worsen secondary neuronal injury
- Target: PaO2 80-120 mmHg (SpO2 94-98%), FiO2 < 0.5 once stable
2.3 Mean Airway Pressure (Pmean) and Its Impact on the Brain
↑ PEEP
→ ↑ Intrathoracic pressure (ITP)
→ ↓ Venous return (impedes vena cava)
→ ↓ Cardiac output → ↓ MAP → ↓ CPP
→ ↑ Central venous pressure (CVP)
→ ↑ Jugular venous backpressure
→ Impedes cerebral venous drainage
→ ↑ CBV → ↑ ICP
- In normal lungs: PEEP transmits ~50% to pleural space → significant venous effects
- In stiff lungs (ARDS, neurogenic pulmonary edema): PEEP transmits < 20% to pleural space → minimal venous/ICP effects
- Therefore: in a patient with concurrent lung injury, higher PEEP may be safe from an ICP standpoint because the stiff chest wall/lung absorbs the pressure
- PEEP ≤ 8 cmH2O is generally safe in ABI with normal lung compliance
- Individual variability is high - ICP monitoring should guide PEEP titration
- A PEEP trial under continuous ICP/CPP monitoring is the most pragmatic approach
- SjvO2 normal: 55-75%
- If ventilation causes excessive cerebral vasoconstriction (aggressive hyperventilation) → ↓ CBF → more O2 extracted → SjvO2 falls < 50% = cerebral ischemia
- If PEEP impairs venous drainage or MAP falls → ↓ CPP → compensatory CBF increase → SjvO2 rises > 75% = luxury perfusion or loss of autoregulation
- These thresholds guide your ventilator adjustments during continuous neuromonitoring
- Every ventilator decision that lowers MAP (high PEEP, high Pmean reducing venous return) attacks CPP from the denominator
- Every decision that raises ICP (hypercapnia, venous obstruction from PEEP) attacks CPP from the other side
- Target CPP: 60-70 mmHg for TBI (BTF Guidelines), >60 mmHg for SAH
- HOB 30 degrees - facilitates cerebral venous drainage, reduces ICP by 3-5 mmHg
- Do NOT place flat for CVP/PEEP assessment if ICP is elevated
PART III: WAVEFORM ANALYSIS
3.1 The Three Core Waveforms
Pressure
^
| Ppeak
| /-------\
| / Pplat \
| / | \
|--+-------+-------> Time
| PEEP baseline
Rise = Active inspiration (flow delivery)
Plateau = Inspiratory hold (no flow; if Ppeak-Pplat > 5: airway resistance high)
Drop = Expiration
- Ppeak - Pplat gap:
- < 5 cmH2O: normal resistance
-
10 cmH2O: high airway resistance (bronchospasm, secretions, kinked tube)
- Pplat alone rises (Ppeak-Pplat normal): decreased compliance (pneumothorax, worsening pulmonary edema, ARDS, abdominal distension)
- In PCV, the pressure-time waveform is a square wave held at the set pressure
Flow
^
|++++++++++ Inspiration (constant, set flow)
|
|__________ Zero crossing
|
|-----------\ Expiration (passive, decelerating)
| \___ Returns to zero = complete exhalation
Flow
^
|\
| \ Inspiration (ramp down from peak)
| \___
|________ Zero
|
|---------\ Expiration
Flow
^
|\
| \ Inspiration: high initial flow, decelerates rapidly as pressure equilibrates
| \
| \__ Approaches zero near end of Ti (if compliance and set time match)
|________
|
|---------\ Expiration
Volume
^
| ___
| / \ Rise during inspiration, VT delivered
| / \ Should return to ZERO before next breath starts
|____/ \___
- Failure to return to zero = gas trapping/auto-PEEP
3.2 Identifying Patient-Ventilator Dyssynchrony - Visual Diagnosis
- What happens: Patient makes an effort, ventilator delivers a breath; before expiration is complete, patient takes another effort that triggers a SECOND full breath - effectively receiving 2x VT
- Pressure-Time: Two pressure peaks in rapid succession with no complete expiratory phase between them
- Flow-Time: Two inspiratory flow peaks, second begins before expiratory flow reaches zero
- Volume-Time: Volume staircase - volume does not return to baseline between cycles
- Neuro relevance: Dangerous - VT of 12-16 mL/kg causes overdistension, barotrauma, and extreme transpulmonary pressures that spike ICP via intrathoracic pressure transmission
- Fix: Increase VT slightly to match patient demand, increase flow rate, consider AC-PC mode, deepen sedation if ICP refractory
- Only occurs in VC with constant flow
- What happens: Patient wants more flow than the set constant flow; generates negative pressure throughout inspiration, "pulling" against ventilator
- Pressure-Time: Characteristic scooping/"saddleback" concave deformity on the inspiratory plateau - pressure dips mid-inspiration
- Flow-Time: Flow remains constant (set value) but patient effort is visible as notches
- Neuro relevance: Increased WOB spikes sympathetic tone, raises ICP; hypercapnia if patient is "fighting" the ventilator
- Fix: Increase flow rate (80-100 L/min), switch to decelerating flow or AC-PC mode
- What happens: Expiration is incomplete before the next breath - air traps in alveoli, creating "intrinsic PEEP" not shown on the set PEEP display
- Flow-Time: Expiratory flow does not return to zero before the next inspiratory cycle starts (key diagnostic sign - see Fishman's Pulmonary Diseases, Fig 146-4)
- Volume-Time: Progressive volume stacking (volume doesn't return to baseline)
- Measurement: Perform an expiratory hold - close the expiratory valve at end-expiration; pressure equilibrates throughout the circuit and rises to the true total PEEP = set PEEP + auto-PEEP (Fishman's, Fig 146-5)
- Neuro relevance: Auto-PEEP raises Pmean → impairs venous drainage → raises ICP; often missed because it's invisible on set-PEEP display
- Fix: Increase expiratory time (increase I:E to 1:3 or 1:4), decrease RR, decrease VT, treat underlying cause (bronchospasm)
- What happens: Ventilator terminates inspiration before patient's neural inspiratory time ends
- Flow-Time: Flow cycling threshold reached before patient finishes effort
- Pressure-Time: Post-cycling notch/dip as patient continues to pull
- Neuro relevance: Patient discomfort, dyssynchrony, fragmented sleep - relevant in weaning phase
- Fix: Adjust flow cycling threshold (e.g., from 25% to 15% of peak flow)
- What happens: Patient makes effort that doesn't trigger a ventilator breath - effort is subthreshold
- Pressure-Time: Small negative deflection (patient effort) with no subsequent breath delivery
- Flow-Time: Small negative flow blips without inspiration following
- Cause: Trigger sensitivity too low, high auto-PEEP (patient must first overcome intrinsic PEEP before triggering)
- Neuro relevance: Patient exhaustion, CO2 retention, agitation
- Fix: Increase trigger sensitivity, add extrinsic PEEP to match auto-PEEP, treat cause
PART IV: CLINICAL NEUROSURGICAL SCENARIOS
Scenario 1: Severe TBI (GCS 6T) - TIGHT BRAIN / REFRACTORY HIGH ICP (ICP 35 mmHg)
Mode: AC - Volume Control
VT: 6 mL/kg IBW (480 mL for 80 kg patient)
RR: 16 breaths/min → titrate to PaCO2 35 mmHg
PEEP: 5 cmH2O (do NOT increase PEEP unless SpO2 < 92%)
FiO2: 0.4-0.5 (target SpO2 94-97%)
Flow: 60-80 L/min (decelerating preferred, reduces Ppeak)
I:E: 1:2 minimum (ensure complete exhalation)
Pplat: < 28 cmH2O (check every shift)
- PaCO2 35-38 mmHg - maintain normocapnia as the baseline
- If acute ICP spike (ICP > 30 with herniation signs): Transiently hyperventilate to PaCO2 30-35 mmHg - a BRIDGE while EVD drainage or osmotherapy is optimized. This is acceptable for < 30-60 minutes; do not sustain
- Avoid PaCO2 > 45 mmHg at all costs - even a brief hypercapnic episode (e.g., from a mucous plug) can cause ICP to spike 15-20 mmHg
- PEEP and ICP trial: Before increasing PEEP for hypoxia, perform 30-second ICP/CPP monitoring at each PEEP increment (5 → 8 → 10 cmH2O). If ICP rises > 5 mmHg or CPP drops > 10 mmHg, do not advance PEEP
- Check for auto-PEEP - perform expiratory hold at bedside; if auto-PEEP exists, it's contributing to elevated ICP invisibly
- Sedation-ventilation synergy: Propofol infusion reduces CMRO2 and CBF, which reduces ICP independently; well-sedated patients also synchronize better, eliminating dyssynchrony-driven ICP spikes
- Do NOT use SIMV (breath-stacking dyssynchrony, variable MV)
- Do NOT allow spontaneous breathing in acute phase without neuromuscular blockade if agitated
- Do NOT target SpO2 > 99% with high FiO2 (hyperoxia worsens outcomes)
Scenario 2: Poor-Grade SAH (WFNS Grade 4-5) - NEUROPROTECTION + VASOSPASM WINDOW
- ICP management (needs normocapnia/mild normalization)
- Vasospasm prevention/treatment (needs euvolemia, maintained CPP > 60, avoid ANY factor that reduces MAP or CBF)
Mode: AC - Volume Control
VT: 6-7 mL/kg IBW
RR: 14-16 breaths/min → target PaCO2 38-42 mmHg
PEEP: 5-8 cmH2O (accept slightly higher if pulmonary status demands)
FiO2: minimize; SpO2 95-98%
Pplat: < 30 cmH2O
- Permissive normocapnia (PaCO2 38-42): In vasospasm window, CBF is already critically reduced; hyperventilation would further reduce CBF in already ischemic zones. Slight permissive normocapnia or even mild hypercapnia (40-42) may help vasospasm by mild vasodilation - discuss with neurosurgeon
- PEEP and CPP: Be conservative - every 5 cmH2O PEEP increase may reduce MAP 3-5 mmHg via reduced venous return. If MAP-driven CPP falls below 60, PEEP must be reduced even at cost of slight oxygenation
- SjvO2 monitoring (if available): SjvO2 < 55% = vasospasm-related ischemia; indicates need for CPP augmentation, NOT ventilator change
- Neurogenic pulmonary edema (NPE): Common in poor-grade SAH; stiff lungs actually protect against PEEP-to-ICP transmission - if NPE present, higher PEEP (8-10 cmH2O) is safer for ICP than it appears
- Tracheostomy at Day 7-10: For poor-grade SAH requiring prolonged ventilation, early tracheostomy (Day 7-10) reduces sedation requirements, facilitates neurological assessment, and improves weaning
Scenario 3: Large MCA Infarct (Malignant MCA) - SPACE-OCCUPYING EDEMA, DAY 3-5
Mode: AC - Volume Control
VT: 6 mL/kg IBW
RR: 16-18/min → PaCO2 35-38 mmHg
PEEP: 5 cmH2O (increase only with continuous ICP monitoring)
FiO2: 0.35-0.45 (target PaO2 80-120 mmHg)
I:E: 1:2 (minimum)
- Head position: HOB 30 degrees facilitates venous drainage; do not nurse flat for hemodynamic reasons
- Prophylactic hyperventilation: AVOIDED - already compromised ipsilateral and contralateral penumbra are at risk; hyperventilation worsens ischemia in salvageable penumbra tissue
- Post-decompressive craniectomy (if performed): After DC, the ICP physiology changes - one Monroe-Kellie wall is gone. PaCO2 management remains important but the urgency of ICP spikes is reduced. Can accept slightly more liberal PaCO2 (38-42 mmHg)
- Opioid-ventilator interaction: Morphine causes CO2 retention; fentanyl preferred if ongoing sedation needed
Scenario 4: Post-Op Posterior Fossa Craniectomy - EARLY WEANING
| Criterion | Target | Notes |
|---|---|---|
| LOC | GCS ≥ 13, following commands | Non-verbal is okay if commands followed |
| Airway reflexes | Intact gag, cough | Critical in posterior fossa - risk of bulbar dysfunction |
| Respiratory drive | Spontaneous RR > 12 with PS | SIMV or PSV trial |
| PaO2/FiO2 ratio | > 200 on PEEP 5, FiO2 ≤ 0.4 | Standard liberation criterion |
| ICP | < 15 mmHg stable | Check 30 min after reducing sedation |
| Swallowing assessment | ENT/SLP evaluation | Especially critical if lower CN at risk |
- Reduce to PSV 8-10 cmH2O + PEEP 5 → monitor for 30-60 min
- Check: patient-initiated RR < 30, SpO2 stable, no excessive WOB, no agitation, no ICP rise
- 30-minute SBT on CPAP 5 cmH2O (no pressure support) - the gold standard weaning trial
- If passed: check ICP trend during SBT (spontaneous breathing increases intrathoracic pressure variation, which can transiently increase ICP by 2-3 mmHg - acceptable if baseline is low)
- Extubate with full team present; have re-intubation kit at bedside
- Post-extubation: maintain HOB 30-45 degrees; if stridor develops, racemic epinephrine + dexamethasone; plan for early tracheostomy if re-intubation needed twice
PART V: SPECIAL TOPICS - BRAIN-LUNG CROSSTALK
5.1 Neurogenic Pulmonary Edema (NPE)
- Mechanism: catecholamine storm after acute brain injury → systemic vasoconstriction → pulmonary hydrostatic overload + endothelial leak
- Common after SAH (10-30% of cases), severe TBI, status epilepticus
- Ventilator consequence: Stiff lungs (low compliance) → driving pressure rises on same VT → higher Ppeak; but PEEP transmits less to ICP
- Management: standard lung-protective ventilation (VT 6 mL/kg, PEEP 8-10 under ICP monitoring), diuresis, optimize CPP
5.2 Driving Pressure (ΔP) - The Modern Ventilation Target
Driving Pressure (ΔP) = Pplat - PEEP = VT / Crs
- ΔP is the best single predictor of VILI and mortality in ARDS
- Target ΔP < 15 cmH2O
- In neuro patients, VILI worsens secondary brain injury via systemic inflammation (ventilator-induced neuro-inflammatory cascade)
- If ΔP is high, do not simply lower PEEP; optimize VT and check for auto-PEEP first
5.3 Mechanical Power (MP)
- Emerging concept: total energy delivered to lungs per minute
- MP = 0.098 x RR x VT x (Ppeak - PEEP/2)
- High MP even with "protective" VT can cause VILI if RR is very high
- Relevant when using RR > 25 to manage PaCO2 - you may be generating VILI through rate, not volume
SUMMARY TABLE: VENTILATOR DECISIONS IN NEUROSURGICAL CONDITIONS
| Parameter | Tight Brain/High ICP | SAH Vasospasm Window | Large MCA Infarct | Post-Op PF Craniectomy |
|---|---|---|---|---|
| Mode | AC-VC | AC-VC | AC-VC | Wean to PSV |
| PaCO2 target | 35-38 mmHg | 38-42 mmHg | 38-40 mmHg | 38-42 mmHg |
| Acute ICP spike | Temporary 30-35 mmHg | AVOID hypervent | AVOID | Usually not needed |
| VT | 6 mL/kg | 6-7 mL/kg | 6 mL/kg | 6-8 mL/kg |
| PEEP | 5 cmH2O | 5-8 cmH2O | 5 cmH2O | 5 cmH2O |
| PEEP increase | Only with ICP monitoring | Caution - watch CPP | With ICP monitoring | Wean rapidly |
| FiO2 target | 0.4-0.5 | 0.35-0.45 | 0.35-0.4 | ≤ 0.4 |
| Pplat | < 28 cmH2O | < 30 cmH2O | < 30 cmH2O | < 30 cmH2O |
KEY REFERENCES AND EVIDENCE
- Al Sharie et al. 2025 (Curr Neurol Neurosci Rep, PMID 41082009) - 10 evidence-based principles for brain-protective ventilation; emphasizes individualized settings, PaCO2 precision, and PEEP under neuromonitoring
- Iavarone et al. 2025 (Intensive Care Med, PMID 40982016) - Detailed mechanistic review of PEEP in acute brain injury; lung-chest wall elastance governs PEEP-ICP transmission
- Zunino et al. 2024 (J Intensive Med, PMID 38681785) - Scoping review, 36 studies on PEEP in ABI; PEEP ≤ 8 cmH2O generally safe, individual monitoring essential
- Brain Trauma Foundation (BTF) Guidelines - PaCO2 35-40 mmHg; hyperventilation only as temporary bridge; ICP monitoring-guided management
- Roberts & Hedges' Clinical Procedures in EM - Mode mechanics, VCV vs PCV definitions
- Fishman's Pulmonary Diseases - Waveform analysis, auto-PEEP detection, driving pressure physiology
- Barash Clinical Anesthesia 9e - CO2-CBF autoregulation curves, PaCO2 physiology
- Bradley & Daroff's Neurology in Clinical Practice - BTF-aligned TBI ventilation guidelines table
Bottom line for your practice: The ventilator is a tool for controlling PaCO2 and oxygenation - the two most readily adjustable determinants of cerebral blood flow and secondary brain injury. In every setting change you make, ask: "What will this do to my patient's PaCO2, and therefore their CBF and ICP?" Get an ABG within 30 minutes of any significant change. Use waveform analysis not as an academic exercise but as a real-time dyssynchrony screen - because every bout of patient-ventilator fighting spikes ICP. And always check auto-PEEP - it is invisible, common, and directly raises ICP.