Scaphoid , lunate in ortho
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full structured answer:
Scaphoid & Lunate - Orthopaedics
SCAPHOID
Anatomy & Blood Supply
The scaphoid is the most commonly fractured carpal bone. Its blood supply enters distally through the scaphoid tuberosity and runs in a retrograde (distal-to-proximal) direction. This is the critical anatomical fact: fractures of the waist interrupt this blood supply to the proximal pole, setting the stage for avascular necrosis (AVN) and nonunion - risks that increase with more proximal fractures.
- In ~10% of individuals, the scaphoid has a sole blood supply from the radial artery entering at the waist, making those patients especially vulnerable.
- It is located in the anatomical snuffbox and forms part of the lateral border of the carpal tunnel.
Fracture Classification (by location)
| Location | Frequency | AVN Risk |
|---|---|---|
| Tuberosity / Distal pole | Least common | Low |
| Waist | Most common (~70%) | Moderate-High |
| Proximal pole | Least common | Highest |
Clinical Features
- Mechanism: fall on an outstretched hand (FOOSH) - hyperextension of wrist
- Pain in the anatomical snuffbox (radial-sided, distal to radial styloid)
- Decreased wrist and thumb ROM
- Clinical tests: anatomical snuffbox tenderness, scaphoid tubercle tenderness, Watson scaphoid shift test, axial compression of 1st metacarpal, resisted supination, "clamp sign"
- Key rule: Snuffbox tenderness = treat as scaphoid fracture until proven otherwise
Imaging
- Plain X-ray: ulnar-deviated PA view (scaphoid view) helps, but fracture may be occult initially
- Pronator quadratus fat pad obliteration on lateral view = clue to wrist injury
- MRI: highest sensitivity; also detects soft tissue injury - preferred for occult fractures
- CT: good for cortical disruption, fracture geometry
- Bone scan: highest sensitivity but low specificity (false positives)
- If X-ray negative but clinically suspected: thumb spica + repeat X-ray at 10-14 days, or early MRI
Management
| Fracture Type | Treatment |
|---|---|
| Nondisplaced distal pole / waist | Short arm thumb spica cast; screw fixation gives faster recovery |
| Displaced / unstable (>1 mm) | ORIF with headless compression screw |
| Proximal pole | Longer immobilization; higher surgical rate due to AVN risk |
| Suspected (X-ray normal) | Thumb spica + ortho follow-up within 1 week |
- No consensus on whether thumb should be included - most surgeons terminate at the IP joint
- Long arm spica (prevents pronation/supination) may be used for the first few weeks
Complications
- AVN (especially proximal pole fractures) - due to retrograde blood supply
- Nonunion - most clinically problematic complication
- Malunion
- Carpal instability (DISI deformity from scapholunate dissociation)
LUNATE
Anatomy
The lunate is the carpal keystone - the central bone in perilunate injury patterns. Its blood supply is variable; a single arterial supply with limited intraosseous branching is most susceptible to AVN. It is crescent-shaped and sits in the lunate fossa of the radius.
Lunate Fracture
- Relatively uncommon; tends to occur with congenitally short ulna (negative ulnar variance)
- Mechanism: FOOSH causing extreme dorsiflexion - force transmitted from capitate to lunate
- Signs: dorsal wrist pain, tenderness just distal to Lister's tubercle, pain on axial loading of long finger metacarpal
- Imaging: often missed on plain X-ray (overlap of radius/ulna); CT or MRI needed; arthroscopy is gold standard
- Management:
- Nondisplaced: short arm cast (double sugar-tong or thumb spica); ortho follow-up 5-7 days
- Displaced (>1-2 mm) / avulsion / comminuted: ORIF (K-wires, cannulated screws, suture anchors)
KIENBÖCK'S DISEASE (AVN of the Lunate)
Overview
- Progressive osteonecrosis of the lunate leading to fragmentation and collapse
- Demographics: men aged 20-40 years
- Multifactorial etiology: negative ulnar variance, single arterial supply, increased intraosseous pressure from venous stasis, decreased radial inclination
- Negative ulnar variance increases shear stress on the marginally perfused lunate - a key risk factor
Diagnosis
- Dorsal wrist pain, mild swelling, limited motion, weakness
- Unexplained persistent non-activity-related dorsal wrist pain in a young adult with negative ulnar variance = do MRI
- X-ray: initially normal or linear fracture → later: lunate sclerosis → lunate collapse
- MRI (early diagnosis): diffuse low signal intensity throughout lunate on T1-weighted images; increased T2 signal = revascularization
Lichtman Classification
| Stage | Description |
|---|---|
| I | Normal X-ray or linear fracture; increased uptake on bone scan |
| II | MRI shows low T1 signal; lunate sclerosis; possible fracture lines; possible early collapse at radial border |
| IIIA | Lunate collapse with normal carpal alignment |
| IIIB | Lunate collapse with fixed scaphoid rotation (ring sign); radioscaphoid angle >60° |
| IV | Severe lunate collapse; proximal capitate migration; degenerative changes at midcarpal and/or radiocarpal joints |
Treatment (based on Lichtman stage + ulnar variance)
- Goal in stages I-IIIA: save the lunate
- Stage I: trial of cast immobilization (limited long-term success)
- Stage II+: surgical treatment per MRI findings
- Joint-leveling procedure is first-line surgery:
- Negative ulnar variance: radial shortening osteotomy preferred (goal: neutral or +1mm)
- Positive ulnar variance: capitate shortening + capitohamate fusion
- Core decompression of radius and ulna: option in early stages (stimulates local vascular healing)
- Vascularized bone grafting (stages I-IIIA): 4th-5th extracompartmental artery (4-5 ECA) is preferred pedicle; may combine with scaphocapitate pinning
- Stage IIIB: must address carpal instability - options: STT fusion, scaphocapitate fusion, proximal row carpectomy (PRC)
- Stage IV: PRC or wrist arthrodesis
- Stages IIIB-IV: salvage procedures only (lunate cannot be revascularized)
SCAPHOLUNATE DISSOCIATION (SLD)
- Most common form of carpal ligament injury
- Mechanism: wrist hyperextension + ulnar deviation + intracarpal supination
- 40% of distal radius fractures may have concomitant SL injury
Diagnosis
- Wrist pain, reduced grip strength
- X-ray: Terry Thomas sign (UK) / David Letterman sign (USA) = gap between scaphoid and lunate >3 mm on PA view, indicating SLD
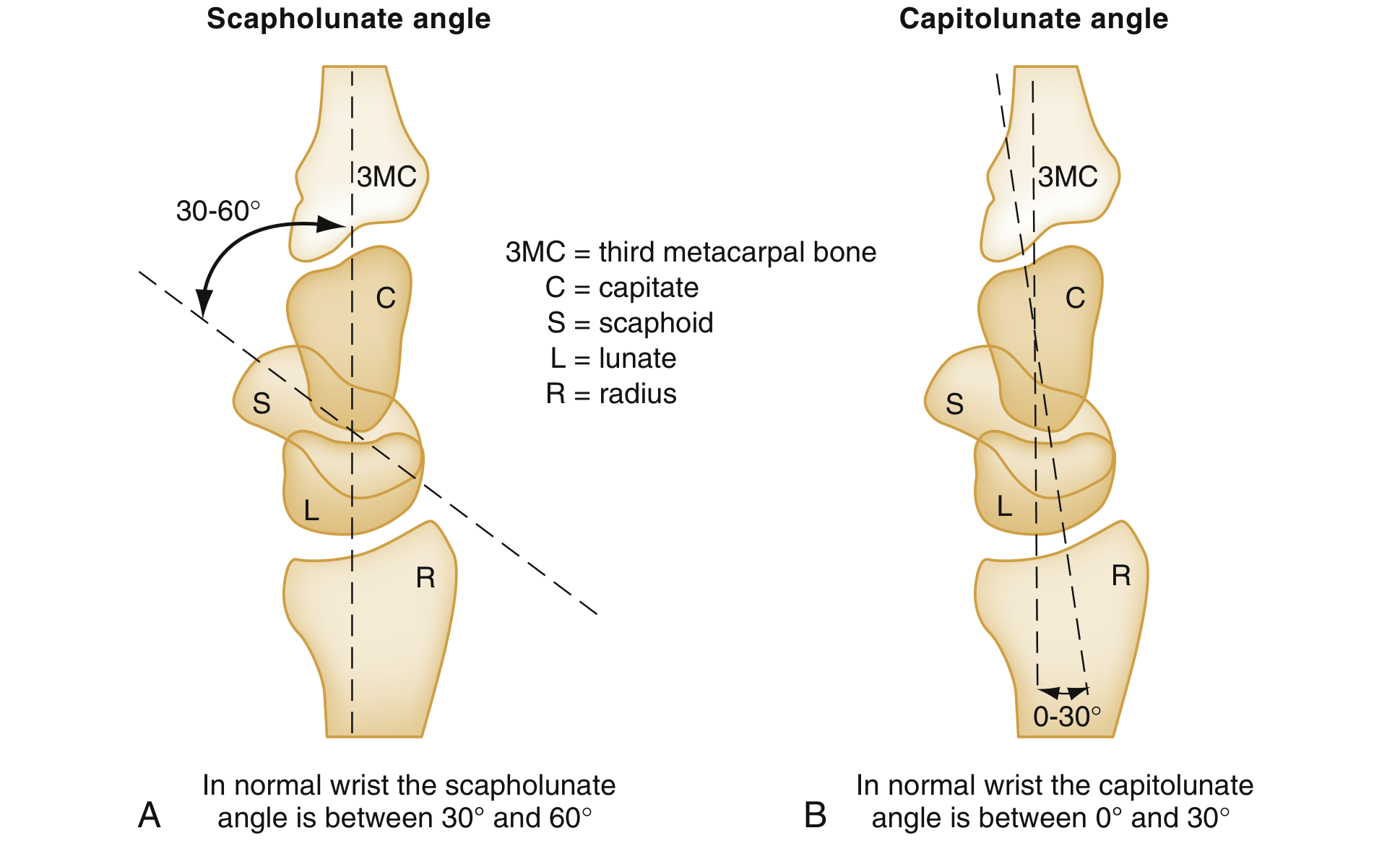
- Lateral X-ray: DISI deformity - scapholunate angle >60° (normal: 30-60°), capitolunate angle >30° (normal: 0-30°)
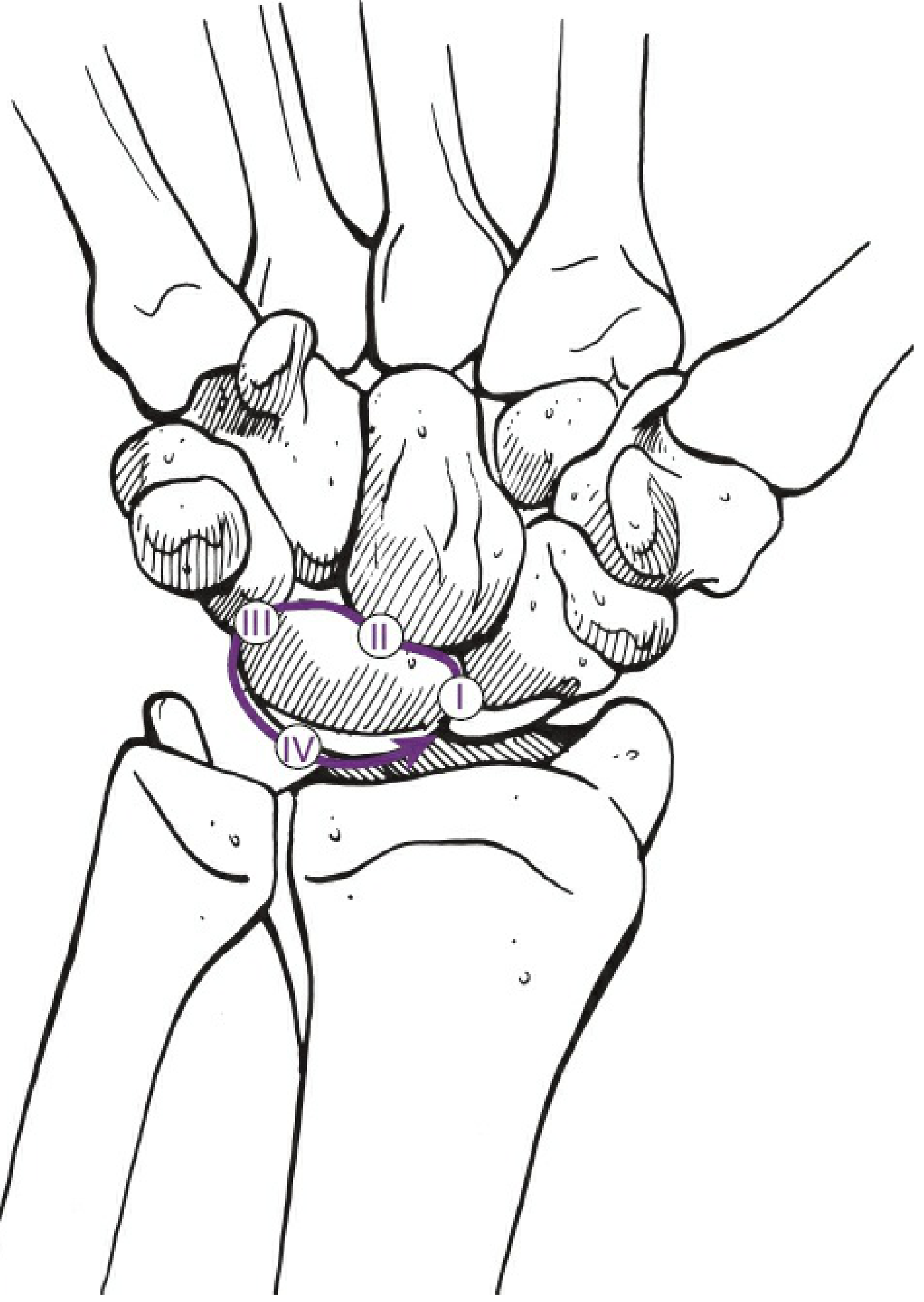
PERILUNATE DISLOCATION (Mayfield Classification)
The lunate is the "keystone" - the distal carpal row dislocates around the lunate in a predictable arc with high-energy FOOSH (hyperextension + supination + ulnar deviation).
- Lesser arc injuries: purely ligamentous
- Greater arc injuries: ligamentous + fractures (scaphoid, radial styloid, capitate, triquetrum, etc.)
Mayfield Stages
| Stage | Event |
|---|---|
| I | Scapholunate disruption (SLD) or scaphoid fracture |
| II | Lunocapitate dislocation (capitate dislocates dorsally through Space of Poirier) |
| III | Lunotriquetral disruption - midcarpal dislocation |
| IV | Lunate dislocates palmarly into the carpal tunnel (using intact palmar ligaments as hinge) - median nerve at risk |
- Perilunate dislocation = lunate stays in radiocarpal fossa; rest of carpus dislocates around it (Stages I-III)
- Lunate dislocation = lunate itself dislocates palmarly (Stage IV) - can cause median nerve compression / acute carpal tunnel syndrome
Management
- Closed reduction in ED to decompress median nerve
- Definitive: surgical reconstruction of intrinsic ligaments + K-wire fixation
- K-wires for 8 weeks; cast/splint for 3 months
- These injuries are easily missed - always check lateral X-ray carpal alignment carefully: the capitate should sit in the "cup" of the lunate
Key High-Yield Summary
| Feature | Scaphoid | Lunate |
|---|---|---|
| Most common fracture | Yes (most common carpal bone Fx) | No (uncommon) |
| AVN cause | Retrograde blood supply | Variable supply (single vessel variant) |
| AVN disease name | - | Kienböck's disease |
| Key risk factor for AVN | Proximal pole fracture | Negative ulnar variance |
| Key radiological sign | Snuffbox tenderness + occult Fx on X-ray | Terry Thomas sign (SLD); DISI |
| Key imaging for early AVN | MRI (low T1 signal) | MRI (low T1 signal) |
| Worst complication | Nonunion + AVN | Carpal collapse + OA (Kienböck stage IV) |
Sources: Rockwood and Green's Fractures in Adults 10e, Rosen's Emergency Medicine, Bailey and Love's Surgery 28e, Campbell's Operative Orthopaedics 15e, Miller's Review of Orthopaedics 9e
Anatomy of hip
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.