As I have neuroimaging on neurocystocercosis, make a short note regarding its findings, etiology , clinical features and management in short
Reading File
Finding Sources
Finding Sources
Searching PubMed
neurocysticercosis neuroimaging MRI CT findings
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I have comprehensive content from multiple authoritative textbooks. Let me now compile the complete note on Neurocysticercosis.
Neurocysticercosis (NCC) - Short Note
Etiology
Neurocysticercosis is the most common parasitic disease of the CNS worldwide and the leading cause of symptomatic epilepsy globally.
- Causative organism: Larval stage (cysticercus) of Taenia solium (pork tapeworm)
- Transmission: Humans become accidental intermediate hosts by ingesting food or water contaminated with T. solium eggs (feco-oral route), or via autoinfection from a tapeworm carrier (eggs attach to hands, transmitted orally)
- After ingestion, ova hatch in the gut, releasing oncospheres which invade the intestinal wall, migrate hematogenously, and lodge in the CNS (as well as muscle, eye, subcutaneous tissue)
- Endemic regions: Latin America, India, sub-Saharan Africa, Southeast Asia
(Bradley and Daroff's Neurology in Clinical Practice; Harrison's Principles of Internal Medicine, 22E)
Clinical Features
- Seizures - the most common presentation; new-onset partial seizures with or without secondary generalization (explains up to 29% of new-onset epilepsy in endemic areas)
- Headache and raised intracranial pressure (ICP) - from hydrocephalus when cysts obstruct CSF flow in ventricles or subarachnoid space
- Focal neurological deficits - depending on cyst location in parenchyma
- Meningitis/encephalitis - when heavy infestation triggers diffuse inflammatory response
- Sudden death - possible with intraventricular cysts causing acute obstructive hydrocephalus
- Spinal cysticerci can mimic intraspinal tumors
Symptoms arise largely from the host's inflammatory response as the cyst degenerates and dies - not from the live parasite itself. Eventually after cyst death (process taking several years), seizures often abate.
(Harrison's, 22E; Tintinalli's Emergency Medicine)
Neuroimaging Findings
This is a staging-based diagnosis. Four stages are recognized, each with distinct CT/MRI appearances:
Stage 1 - Vesicular Stage (Live cyst)
- Cyst contains viable larva with an invaginated scolex
- MRI: Well-defined cystic lesion with a small eccentric nodule (scolex) - the classic "hole-with-dot" sign (cyst + scolex)
- No significant perilesional edema
- No surrounding enhancement
- Fluid isointense to CSF on all sequences
Stage 2 - Colloidal Stage (Degenerating cyst)
- Host immune response begins as larva degenerates
- MRI: Ring or peripheral enhancement on post-contrast images
- Substantial surrounding edema on T2/FLAIR images
- Cyst contents become turbid (hyperintense to CSF on T1)
Stage 3 - Granulonodular Stage
- Cyst shrinks, scolex mineralizes
- MRI post-contrast: Homogeneous solid nodular enhancement (no central cyst cavity)
- No surrounding edema on FLAIR
- Lesion is smaller and more solid
Stage 4 - Nodular-Calcified Stage (Dead/burnt-out)
- Cyst completely dies and calcifies
- CT: Best modality - shows punctate parenchymal calcifications (most common finding overall)
- MRI: Calcifications can be difficult to detect; susceptibility-weighted imaging (SWI) is the most sensitive MRI sequence for these small calcific foci
- No enhancement, no edema
Key teaching point: Multiple lesions at different stages may coexist simultaneously in the same patient - active enhancing lesions, ring-enhancing cysts with edema, and calcified "burnt-out" lesions all visible together.
Special Forms on Imaging
| Form | Imaging Features |
|---|---|
| Leptomeningeal/Basal | Soft tissue filling basal cisterns with marked contrast enhancement; granulomata with variable calcification in subarachnoid space |
| Intraventricular | Cyst within ventricle (may be isointense to CSF, easy to miss on CT); MRI superior for detecting cyst + scolex; risk of acute hydrocephalus |
| Racemose | Multilobular cysts without a scolex in subarachnoid space; typically in cerebellopontine angles, suprasellar region, basal cisterns, and Sylvian fissures; may enhance |
| Complications | Hydrocephalus, brain infarcts (from vasculitis), meningeal enhancement |
MRI vs CT: MRI is superior for detecting intraventricular cysts and the scolex; CT is better for calcifications.
(Grainger & Allison's Diagnostic Radiology; Harrison's Principles of Internal Medicine, 22E)
Management
Treatment is individualized based on the number, location, viability, and stage of cysts.
1. Antiparasitic (Anthelminthic) Therapy
| Scenario | Treatment |
|---|---|
| Parenchymal viable/enhancing (1-2 cysts) | Albendazole monotherapy + steroids |
| Parenchymal viable/enhancing (>2 cysts) | Albendazole + Praziquantel + steroids |
| Calcified cysts (any number) | No antiparasitic treatment (parasite already dead) |
| Encephalitis / diffuse cerebral edema | No antiparasitic treatment - steroids only |
- Standard dose: Albendazole 15 mg/kg/day (in 2 divided doses) x 8-28 days; Praziquantel 50-100 mg/kg/day x 15-30 days
2. Corticosteroids
- Used to control the inflammatory response triggered by dying parasites
- Dexamethasone or prednisolone - mandatory when using antiparasitic drugs to reduce edema and seizure risk
3. Antiepileptic Drugs (AEDs)
- Seizures are typically controlled with antiepileptic monotherapy
- AEDs are first-line for symptomatic seizures regardless of cyst stage
4. Surgical / Interventional
| Scenario | Approach |
|---|---|
| Intraventricular (lateral or 3rd ventricle) | Neuroendoscopic removal (preferred) |
| 4th ventricle cyst | Neuroendoscopic or microsurgical removal |
| Removal not feasible | Ventricular shunt first, then antiparasitic + steroids |
| Subarachnoid (extraparenchymal) | Ventricular shunt if hydrocephalus, then prolonged albendazole ± praziquantel |
| Hydrocephalus with no visible cysts | Ventricular shunt only; no antiparasitic treatment |
| Ocular cysticercosis | Surgical resection of cysts |
| Spinal cysticercosis | Surgical removal or antiparasitic + steroids (individualized) |
5. Diagnosis Confirmation (if needed)
- Enzyme-linked immunotransfer blot (EITB) is the recommended serological confirmatory test
- Fundoscopy is recommended for all suspected cases (to rule out ocular involvement before starting antiparasitic therapy - treatment can cause inflammatory damage to the eye if cysts are present)
(Bradley and Daroff's Neurology - Table 79.7, adapted from IDSA/ASTMH 2017 Clinical Practice Guidelines; Harrison's 22E; Tintinalli's)
Sources:
- Harrison's Principles of Internal Medicine, 22E (McGraw Hill, 2025)
- Grainger & Allison's Diagnostic Radiology
- Bradley and Daroff's Neurology in Clinical Practice
- Tintinalli's Emergency Medicine
- Goldman-Cecil Medicine
What are different types of imaging seen in MRI
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything I need to write a thorough, well-illustrated note on MRI imaging types. Here is the complete answer:
Types of MRI Imaging (MRI Sequences / Modalities)
MRI generates images by detecting radiofrequency energy emitted by hydrogen protons returning to their resting alignment after a pulse sequence. The image is essentially a map of water/hydrogen content in tissue, but different pulse sequences highlight different tissue properties.
Standard / Conventional Sequences
1. T1-Weighted Imaging
- Physics: Uses short TR (repetition time) and short TE (echo time). Highlights longitudinal (spin-lattice) relaxation
- Appearance:
- White matter: bright (hyperintense)
- Gray matter: intermediate
- CSF: dark (hypointense)
- Fat: bright
- Extravasated blood (subacute): bright
- Calcium/bone cortex: dark
- Best for: Anatomy, fat, subacute hemorrhage, gadolinium contrast enhancement, posterior pituitary "bright spot," marrow infiltration
- Gadolinium-enhanced T1: Areas of blood-brain barrier (BBB) disruption (tumors, abscess walls, active inflammation, demyelination) light up brightly due to T1-shortening effect of gadolinium
2. T2-Weighted Imaging
- Physics: Uses long TR and long TE. Highlights transverse (spin-spin) relaxation
- Appearance:
- CSF: bright (hyperintense)
- Gray matter: hyperintense to white matter
- Edema, inflammation, tumor, demyelination: bright
- Calcium: dark (signal void)
- Flowing blood: dark (flow void)
- Best for: Edema, demyelination (MS plaques), ischemic lesions, spinal cord lesions, disc herniation, tumors, encephalitis
- Key teaching: In neurocysticercosis, perilesional edema (colloidal stage) shows bright on T2
3. FLAIR (Fluid-Attenuated Inversion Recovery)
- Physics: A T2-weighted sequence with an inversion pulse that nulls/suppresses the bright CSF signal. This makes lesions near CSF-containing spaces (periventricular, cortical) much easier to see
- Appearance:
- CSF: dark (suppressed)
- White matter lesions, cortical lesions: bright against dark background
- Gray-white differentiation: accentuated
- Best for: Periventricular MS plaques, cortical and subcortical lesions, subarachnoid hemorrhage (SAH - CSF appears bright rather than dark on FLAIR), leptomeningeal disease, establishing chronicity of lesions
- In NCC: Vesicular (live) cysts show no FLAIR signal; granulonodular stage shows no surrounding edema on FLAIR
Here you can see the standard sequences side by side on the same normal brain - note how CSF (ventricles) is dark on T1 (A), bright on T2 (B), and suppressed/dark on FLAIR (C):
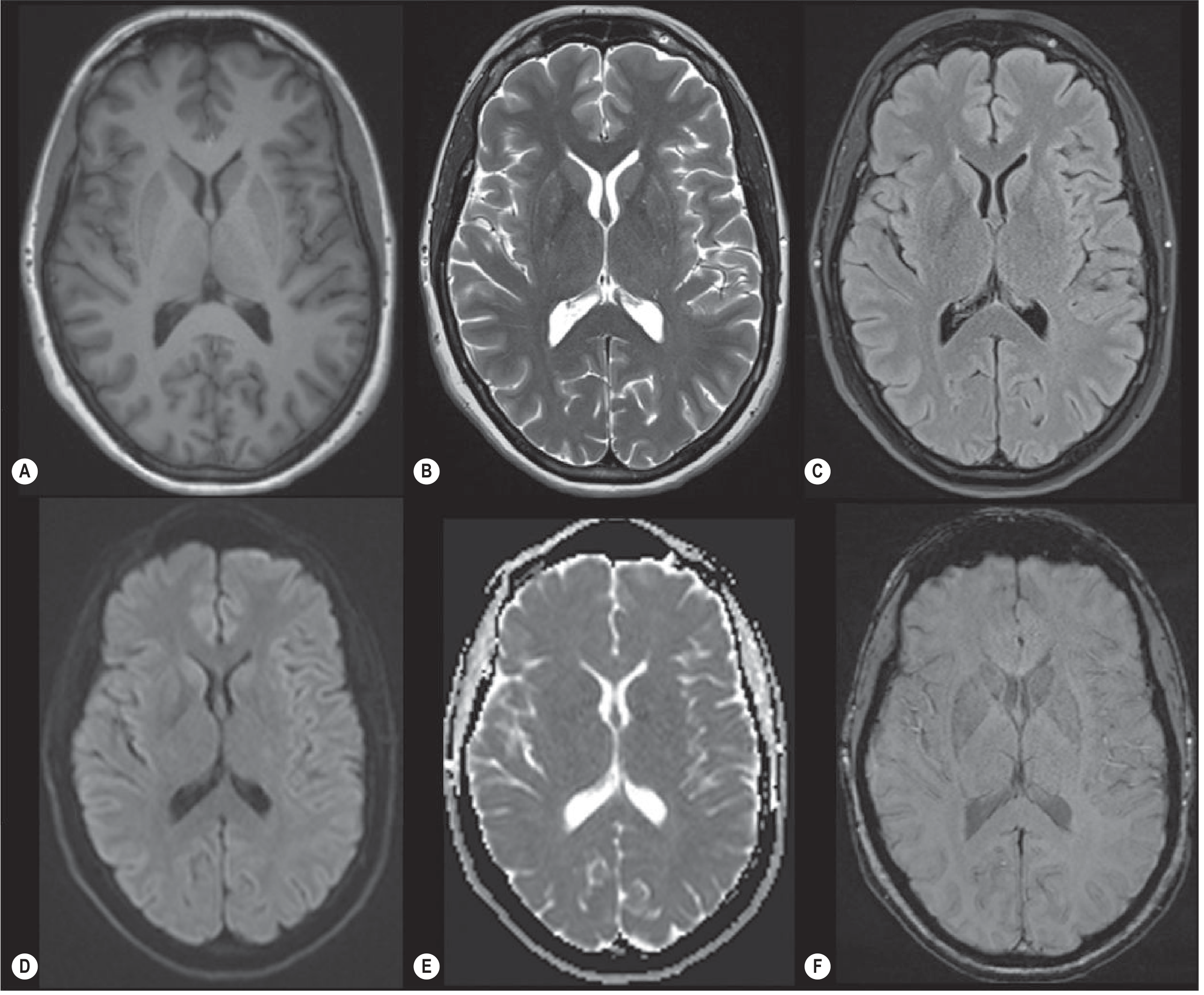
(A) T1 - (B) T2 - (C) FLAIR - (D) DWI - (E) ADC map - (F) SWI
- Grainger & Allison's Diagnostic Radiology, Fig. 53.32
4. Proton Density (PD) Weighted Imaging
- Uses long TR and short TE
- Reflects the actual density of hydrogen protons in tissue
- Both CSF and lesions appear bright; good tissue contrast
- Used mainly in musculoskeletal MRI; less common in brain imaging now
Diffusion-Based Sequences
5. DWI - Diffusion-Weighted Imaging
- Physics: Measures the free diffusion of water molecules within tissue. Uses strong gradient pulses that dephase/rephase moving water
- Appearance on DWI:
- Restricted diffusion (impeded water movement) = bright (hyperintense)
- Free/facilitated diffusion = dark
- Key uses:
- Acute ischemic stroke - the most important indication. In stroke, failure of Na-K ATPase causes cytotoxic edema and intracellular swelling, restricting water movement. DWI becomes positive within minutes to hours, far earlier than T1, T2, or CT
- Brain abscess (pus shows restricted diffusion)
- Epidermoid cysts
- Dense tumors
- Creutzfeldt-Jakob disease (cortical ribboning)
6. ADC Map (Apparent Diffusion Coefficient)
- Always interpreted alongside DWI
- True restricted diffusion: Bright on DWI + dark (hypointense) on ADC = confirms restriction (e.g., acute infarct, abscess)
- T2 shine-through: Bright on DWI + bright on ADC = not true restriction (just residual T2 signal)
- ADC map is a calculated quantitative map of water diffusivity
Advanced Functional/Specialized Sequences
7. SWI - Susceptibility-Weighted Imaging
- Physics: Exploits the magnetic susceptibility differences between tissues. Blood products (deoxyhemoglobin, hemosiderin), calcium, iron, and air create local field distortions
- Appearance: These substances appear as dark "blooming" signal voids, more conspicuous than on standard sequences
- Best for:
- Microhemorrhages (e.g., in diffuse axonal injury, cerebral amyloid angiopathy)
- Cerebral venous thrombosis (thrombus appears dark)
- Cavernous malformations
- Old calcifications in NCC - SWI is the most sensitive MRI sequence for detecting small calcific foci in the nodular-calcified stage
- Mineral deposition disorders
8. MR Perfusion Imaging
Three main techniques:
| Technique | Contrast needed | What it measures |
|---|---|---|
| DSC (Dynamic Susceptibility Contrast) | Yes (gadolinium) | CBV, CBF, MTT from T2* signal drop |
| DCE (Dynamic Contrast Enhanced) | Yes (gadolinium) | Ktrans (capillary permeability) - elevated in gliomas, metastases |
| ASL (Arterial Spin Labeling) | No (contrast-free) | Blood flow via magnetic labeling of inflowing blood |
- Best for: Brain tumor grading (high CBV in high-grade gliomas), tumor vs. treatment effect, infarct penumbra, vasospasm assessment
9. MRS - MR Spectroscopy
- Physics: Instead of using spatial gradient info to build an image, MRS creates a spectrum of resonance peaks for different metabolites in tissue
- Key metabolites:
- NAA (N-acetylaspartate): Neuronal viability marker - reduced in neuronal loss/injury
- Cho (Choline): Cell membrane turnover marker - elevated in tumors, inflammation
- Cr (Creatine): Reference metabolite in metabolically active tissue
- Lac (Lactate): Anaerobic metabolism marker
- Lip (Lipids): Released with cell membrane damage - necrosis
- mI (Myo-inositol): Marker of gliosis/Alzheimer's
- Best for: Brain tumor grading, tumor vs. radiation necrosis, metabolic/leukodystrophic diseases, infection characterization
10. fMRI - Functional MRI
- Physics: Uses BOLD (Blood-Oxygenation-Level-Dependent) signal - neural activity causes local over-delivery of oxygenated blood, changing T2* signal in active cortex
- Best for: Pre-operative mapping of eloquent cortex (motor, language, memory) before tumor or AVM surgery; epilepsy surgical work-up; research
11. DTI - Diffusion Tensor Imaging
- Advanced form of DWI that measures directionality of water diffusion (anisotropy) along white matter tracts
- Used to generate tractography - 3D maps of white matter fiber bundles
- Best for: Pre-surgical white matter tract mapping, traumatic brain injury, demyelinating disease progression
12. MR Angiography (MRA)
- Time-of-Flight (TOF) MRA: No contrast; relies on flow-related enhancement of moving blood against suppressed background tissue
- Contrast-enhanced MRA: Gadolinium-based; better for large vessels
- Best for: Intracranial aneurysms, arteriovenous malformations (AVMs), carotid/vertebral stenosis, cerebral venous sinus thrombosis
Summary Table
| Sequence | CSF | WM | GM | Best Use |
|---|---|---|---|---|
| T1 | Dark | Bright | Intermediate | Anatomy, gadolinium enhancement, fat |
| T2 | Bright | Dark | Bright | Edema, demyelination, tumors |
| FLAIR | Dark (suppressed) | Dark | Bright | Periventricular/cortical lesions, SAH |
| DWI | Dark | Dark | Dark | Acute stroke, abscess |
| ADC | Bright | Bright | Bright | Confirm true restriction (dark = real) |
| SWI | - | - | - | Microbleed, calcification, iron |
| Perfusion | - | - | - | Tumor, penumbra |
| MRS | - | - | - | Metabolites, tumor vs. necrosis |
| fMRI | - | - | - | Eloquent cortex mapping |
| DTI | - | - | - | White matter tracts |
| MRA | - | - | - | Vessels, aneurysm, stenosis |
Sources:
- Adams and Victor's Principles of Neurology, 12th Edition (McGraw Hill)
- Grainger & Allison's Diagnostic Radiology (Elsevier)
- Bradley and Daroff's Neurology in Clinical Practice (Elsevier)
- Neuroanatomy through Clinical Cases, 3rd Edition
What can external else ask for CT and MRI in general rather than smcase specific ?
Finding Sources
Finding Sources
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.