Lymphadenitis
Reading File
Finding Sources
Searching PubMed
lymphadenitis diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have excellent content from multiple authoritative sources. Let me compile a comprehensive answer.
Lymphadenitis
Lymphadenitis is inflammation of lymph nodes, resulting from immune activation by infectious or inflammatory stimuli. It is classified as acute or chronic, and further as nonspecific (reactive) or specific (granulomatous, etc.).
Normal Lymph Node Physiology (Background)
Lymph nodes are discrete encapsulated structures containing separate B-cell zones (cortical follicles) and T-cell zones (paracortex), richly supplied with phagocytes and antigen-presenting cells. On antigenic stimulation, primary follicles enlarge to form secondary follicles with pale germinal centers within days. Lymph nodes in adults are almost never truly "resting," making it necessary to distinguish past residual changes from active disease.
- Robbins & Cotran Pathologic Basis of Disease
1. Acute Nonspecific Lymphadenitis
Causes
- Cervical region: drainage from dental or tonsillar infections (Streptococcus, Staphylococcus, Actinomycosis)
- Axillary / inguinal: infections of the extremities
- Mesenteric: acute appendicitis, inflammatory gut conditions, self-limiting viral infections
- Generalized: systemic viral infections (especially in children) and bacteremia
Morphology
- Nodes are swollen, gray-red, and engorged
- Microscopically: enlarged reactive germinal centers with numerous mitotic figures
- Macrophages contain particulate debris from dead bacteria/necrotic cells
- Pyogenic organisms → neutrophilic infiltration, follicle center necrosis, possible conversion of entire node to pus
- Activated, enlarged endothelial cells line the sinuses
- With abscess formation: nodes become fluctuant, overlying skin becomes red
- Suppurative infections may track through the capsule to form draining sinuses
- Healing may leave residual scarring
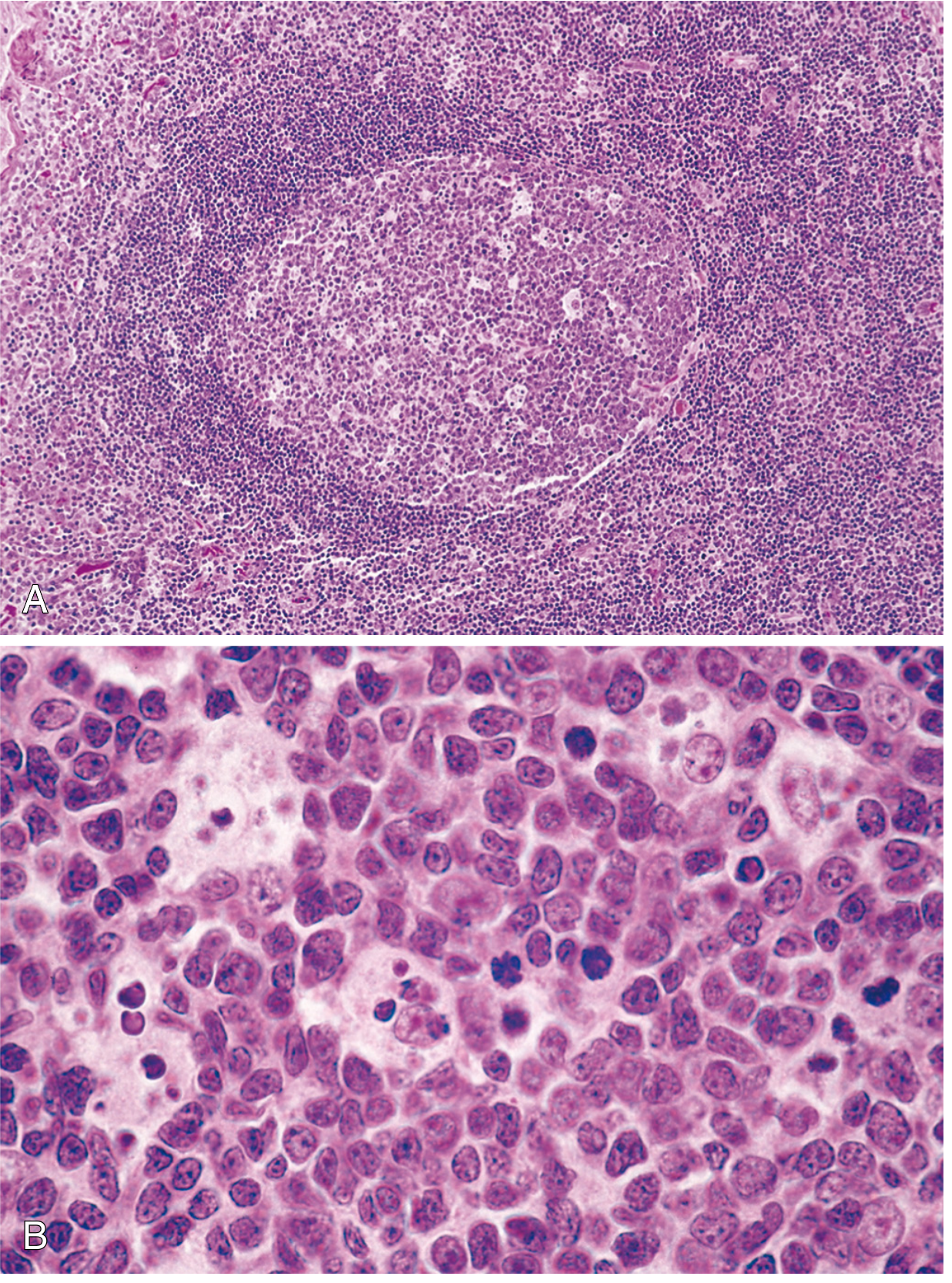
Fig. 13.3 - Follicular hyperplasia in reactive lymphadenitis. Robbins & Cotran Pathologic Basis of Disease.
Clinical Features
- Enlarged, tender nodes
- Systemic: pyrexia, anorexia, malaise
- Fluctuance when abscess formation is extensive
Treatment
- Directed at the primary focus of infection (e.g., treat tonsillitis or dental abscess)
2. Chronic Nonspecific Lymphadenitis
Various chronic immunological stimuli produce three distinct histological patterns (often coexisting):
| Pattern | Mechanism | Causes | Histology |
|---|---|---|---|
| Follicular hyperplasia | Humoral immune activation | Rheumatoid arthritis, toxoplasmosis, early HIV | Large oblong secondary follicles with polarized germinal centers (dark zone of centroblasts + light zone of centrocytes); tangible body macrophages |
| Paracortical hyperplasia | T-cell mediated | Acute viral infections (e.g., EBV/infectious mononucleosis) | Expanded T-cell zones with immunoblasts (3-4x size of resting lymphocytes), can efface B-cell follicles |
| Sinus histiocytosis | Sinusoidal macrophage proliferation | Lymph nodes draining cancers (e.g., breast carcinoma) | Increased endothelial cells and intrasinusoidal macrophages distending sinusoids |
Distinguishing reactive hyperplasia from follicular lymphoma:
- Preserved lymph node architecture (T-cell zones, sinusoids intact)
- Marked variation in follicle shape/size
- Frequent mitotic figures, phagocytic macrophages, and recognizable light/dark zones (all tend to be absent from neoplastic follicles)
3. Specific (Granulomatous) Lymphadenitis
TB Lymphadenitis (Scrofula)
This is the most common form of extrapulmonary TB.
Epidemiology:
- Most common in young women and children
- In the USA, scrofula is more often caused by non-tuberculous mycobacteria than M. tuberculosis
- More common in HIV-coinfected individuals (tends to be generalized in HIV+)
- Pulmonary disease coexists in only a minority of isolated TB lymphadenitis cases
Clinical features:
- Painless, enlarging, firm, red mass - most commonly anterior/posterior cervical chain or supraclavicular fossa
- Early: discrete, rubbery, freely mobile nodes with normal overlying skin
- Late: matted, harder nodes with inflamed skin; fluctuance, abscess, or sinus tract if node erodes through skin
- Systemic symptoms (fever, night sweats) uncommon in immunocompetent patients
Secondary effects by nodal location:
- Intrathoracic adenopathy → bronchial compression, upper airway obstruction
- Intrathoracic/intraabdominal nodes → chylothorax, chylous ascites (from lymphatic disruption)
Diagnosis:
- Fine-needle aspiration (FNA) of the affected node is the preferred method
- AFB smear: positive in only ~20% of cases
- Granulomatous inflammation may be apparent on cytology
- FNA sensitivity 77%, specificity 93% for TB
Treatment:
- First-line: standard anti-tuberculous drug therapy
- Surgical excision: reserved for failure of medical therapy or diagnostic uncertainty
- Incision and drainage is contraindicated - results in permanent sinuses and prolonged drainage
4. Filarial Lymphadenitis (Special Form - Acute Retrograde)
Seen in endemic areas (bancroftian/Malayan filariasis), caused by dying adult worms.
- Inguinal lymphadenitis most common; painful, with overlying skin erythema
- Precedes lymphangitis; accompanied by fever and chills
- Episodes last ~1 week, frequently recur
- Can be complicated by epididymitis, orchitis in men
- Repeated episodes → lymphatic vessel dilation → chronic lymphedema (elephantiasis)
Causes of Cervical Lymphadenopathy - Summary
| Category | Examples |
|---|---|
| Reactive hyperplasia | Non-specific stimuli |
| Viral | Infectious mononucleosis (EBV), HIV |
| Bacterial | Streptococcus, Staphylococcus, actinomycosis, TB, brucellosis |
| Protozoan | Toxoplasmosis |
| Primary malignancy | Lymphoma (Hodgkin and non-Hodgkin) |
| Metastatic malignancy | Squamous cell carcinoma (common in older adults), other carcinomas |
Key Differentiating Points
| Feature | Acute Bacterial | Reactive (Viral) | TB | Lymphoma |
|---|---|---|---|---|
| Pain | Tender | Mild tenderness | Painless | Painless |
| Consistency | Soft/fluctuant | Rubbery | Firm, matted | Rubbery/"rubbery-hard" |
| Skin changes | Erythema | None | May perforate | None |
| Systemic | Fever, malaise | Pharyngitis, rash | Rare (unless HIV+) | B-symptoms (drenching sweats, weight loss, fever) |
| Treatment | Antibiotics | Supportive | Anti-TB drugs | Chemotherapy/radiotherapy |
Sources: Robbins & Cotran Pathologic Basis of Disease, p.552 | Robbins & Kumar Basic Pathology | Rosen's Emergency Medicine | Goldman-Cecil Medicine | Bailey and Love's Short Practice of Surgery, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.