trigeminal nerve examination
Reading File
Finding Sources
Searching the Web
trigeminal nerve cranial nerve 5 clinical examination technique
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, textbook-grounded guide to trigeminal nerve (CN V) examination.
Trigeminal Nerve (CN V) Examination
Anatomy Overview
The trigeminal nerve is the largest cranial nerve - a mixed sensory and motor nerve. Its sensory cell bodies lie in the Gasserian (semilunar) ganglion in Meckel's cave on the floor of the middle cranial fossa. Three divisions exit the skull through separate foramina:
| Division | Foramen | Area Supplied |
|---|---|---|
| V1 - Ophthalmic | Superior orbital fissure | Forehead, scalp (to vertex), upper eyelid, cornea, conjunctiva, nasal bridge |
| V2 - Maxillary | Foramen rotundum | Cheek, lower eyelid, upper lip, upper teeth, nasal mucosa |
| V3 - Mandibular | Foramen ovale | Chin, lower lip, lower teeth, anterior 2/3 of tongue (general sensation), jaw muscles |
The motor root originates in the trigeminal motor nucleus in the mid-pons and joins V3 to supply the muscles of mastication (masseter, temporalis, medial and lateral pterygoids), plus tensor tympani, tensor veli palatini, mylohyoid, and anterior digastric.
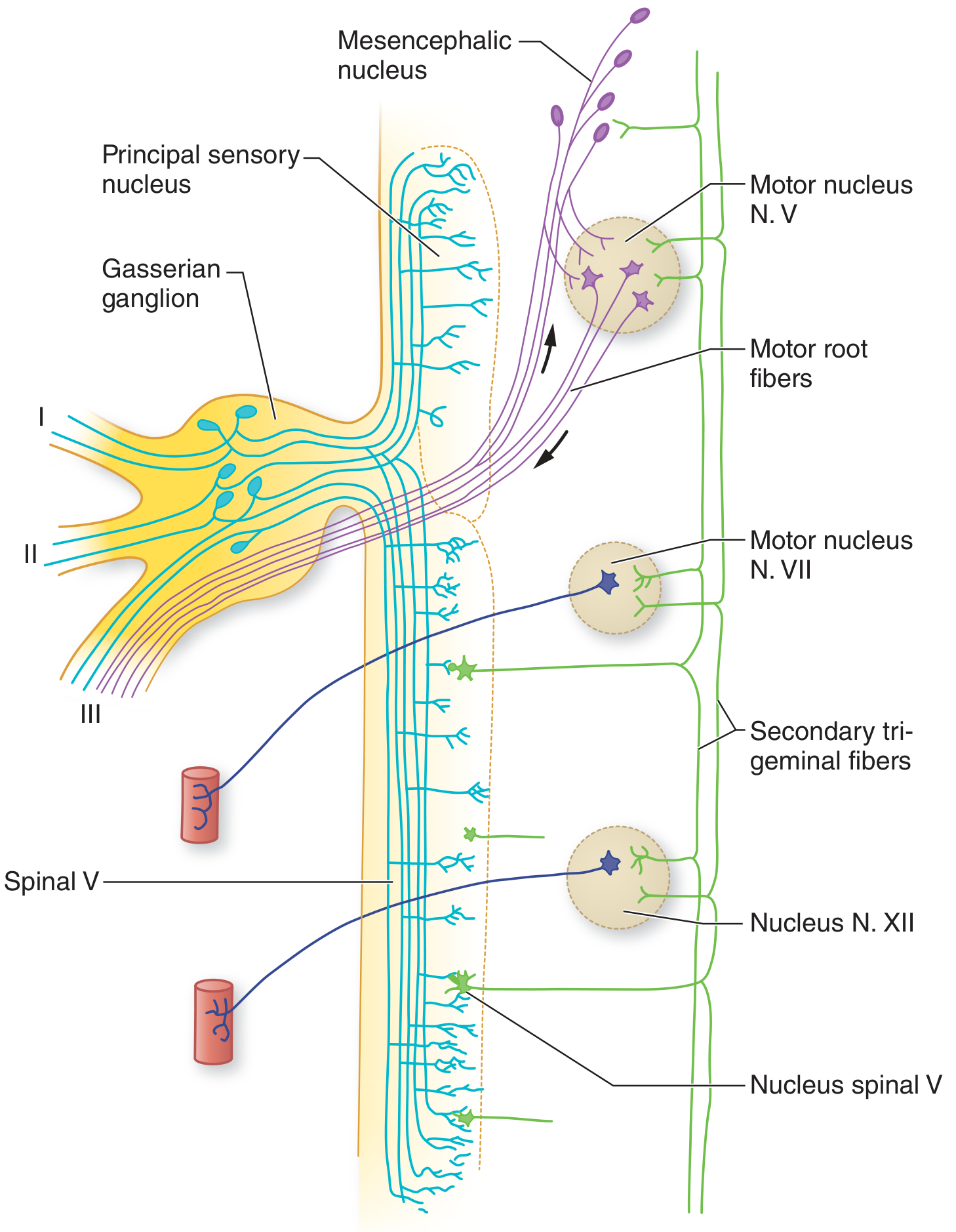
Scheme of the trigeminal nuclei and reflex arcs. I = ophthalmic, II = maxillary, III = mandibular divisions. - Adams and Victor's Principles of Neurology, 12e
Examination Components
1. Motor Function
Muscles to test: masseter, temporalis, pterygoids
Steps:
- Masseter and temporalis: Ask the patient to clench their teeth firmly. Palpate both muscles simultaneously - compare bulk and strength side-to-side.
- Pterygoids (jaw opening): Ask the patient to open their mouth. In unilateral pterygoid weakness, the jaw deviates toward the weak (affected) side due to the unopposed action of the contralateral pterygoid.
- Lateral pterygoid (jaw protrusion): Ask the patient to push the jaw forward and side to side; resist the movement to assess strength.
Note: The upper motor neuron control to the trigeminal motor nucleus is predominantly bilateral, so a unilateral corticobulbar lesion usually causes no jaw weakness. However, bilateral upper motor neuron lesions (e.g., ALS, diffuse white matter disease) cause a brisk jaw jerk and possible spastic jaw. - Neuroanatomy through Clinical Cases, 3e
2. Sensory Function
Test each of the three divisions on both sides of the face, comparing left vs. right. Use at least two modalities that travel via different anatomic pathways (e.g., light touch + temperature/pain).
Areas to test:
- V1: Forehead (above eyebrows)
- V2: Cheek (malar eminence / below the eye)
- V3: Chin and lower jaw
Modalities:
| Modality | Pathway | How to Test |
|---|---|---|
| Light touch | Principal sensory nucleus (pons) | Cotton wisp, lightly stroked |
| Pain | Spinal trigeminal nucleus (pons - C2/C3) | Sterile pin - "sharp or dull?" |
| Temperature | Spinal trigeminal nucleus | Warm/cold tubes or tuning fork |
| Proprioception | Mesencephalic nucleus | N/A - usually tested via jaw jerk |
Additional sensory areas to remember:
- Mucous membranes of nose, mouth, and paranasal sinuses
- Anterior 2/3 of tongue (general sensation, not taste - taste is CN VII)
- Conjunctiva
Testing of two sensory modalities derived from different anatomic pathways (e.g., light touch and temperature) is sufficient for a screening examination. - Harrison's Principles of Internal Medicine, 22e
3. Corneal Reflex
The corneal reflex is one of the most sensitive tests of trigeminal nerve integrity.

Eliciting the corneal reflex with a cotton swab. - Neuroanatomy through Clinical Cases, 3e
Technique: Approach from the side (outside the patient's visual field) and gently touch the lower/lateral cornea with a wisp of cotton or saline drop. Do not touch the sclera or conjunctiva - only the cornea. The normal response is bilateral eye closure.
Reflex arc:
- Afferent limb: Ophthalmic division (V1) → chief sensory nucleus + spinal trigeminal nucleus
- Efferent limb: Facial nerve (CN VII) → orbicularis oculi → eye closure
Responses to record:
- Direct reflex: closure of the ipsilateral eye
- Consensual reflex: closure of the contralateral eye
Interpretation:
| Finding | Lesion |
|---|---|
| Absent direct + absent consensual (ipsilateral stimulation) | V1 afferent lesion (trigeminal) |
| Absent direct only (ipsilateral) | CN VII efferent lesion on that side |
| Absent corneal reflex contralateral to a parietal lesion | Suprasegmental cortical modulation deficit |
Lesions of the trigeminal sensory pathways, the facial nerve, or their connections causes a decreased corneal reflex in the ipsilateral eye. - Neuroanatomy through Clinical Cases, 3e
4. Jaw Jerk Reflex (Masseter Reflex)
Technique: Ask the patient to let the mouth hang slightly open and relax the jaw. Place your index finger on the patient's chin horizontally, then tap your finger with a tendon hammer. The response is a brief upward jerk of the jaw (masseter contraction).
Reflex arc:
- Afferent limb: Ia fibers in the mandibular division (V3) → mesencephalic trigeminal nucleus
- Efferent limb: Motor nucleus of CN V → masseter and temporalis
Interpretation:
| Finding | Significance |
|---|---|
| Absent or minimal jaw jerk | Normal finding |
| Brisk / hyperactive jaw jerk | Bilateral upper motor neuron lesion (e.g., pseudobulbar palsy, ALS, bilateral corticospinal disease) |
| Depressed jaw jerk | Lower motor neuron lesion of V3 or trigeminal motor nucleus |
In normal individuals, the jaw jerk reflex is minimal or absent. In bilateral upper motor neuron lesions, the jaw jerk reflex may be brisk. - Neuroanatomy through Clinical Cases, 3e
5. Sneezing Reflex (Additional)
Tickling the nasal mucosa normally produces reflex sneezing. Absence suggests trigeminal dysfunction. This is typically tested only when a peripheral V lesion is suspected. - S. Das Manual of Clinical Surgery, 13e
Interpretation Summary
| Examination Finding | Implication |
|---|---|
| Facial numbness in V1-V3 territory | Peripheral trigeminal nerve lesion |
| Jaw deviates to one side on opening | Ipsilateral pterygoid weakness (LMN) |
| Absent corneal reflex (afferent defect) | V1 or trigeminal pathway lesion |
| Absent corneal reflex (efferent defect) | CN VII (facial nerve) lesion |
| Brisk jaw jerk | Bilateral UMN lesion above pons |
| Absent jaw jerk | LMN lesion (V3 or motor nucleus) |
| V2/V3 numbness, paroxysmal severe pain | Trigeminal neuralgia (tic douloureux) |
| Isolated chin numbness | Metastatic neoplasm until proven otherwise |
Clinical Localization Pearls
- Gasserian ganglion lesion (e.g., herpes zoster, schwannoma): all three divisions affected + motor weakness
- Cavernous sinus lesion: V1 and V2 affected (V3 exits separately at foramen ovale and is spared)
- Brainstem lesion (spinal trigeminal tract): ipsilateral facial pain/temperature loss with contralateral body sensory loss = lateral medullary (Wallenberg) syndrome
- Supranuclear lesion: unilateral cortical lesion usually spares jaw movement (bilateral representation); bilateral lesions cause pseudobulbar palsy with brisk jaw jerk
- Mental nerve (branch of V3) neuropathy presenting as isolated chin/lower lip numbness is a red flag for mandibular metastasis
Sources:
- Harrison's Principles of Internal Medicine, 22e
- Adams and Victor's Principles of Neurology, 12e
- Neuroanatomy through Clinical Cases, 3e
- Localization in Clinical Neurology, 8e
- S. Das Manual of Clinical Surgery, 13e
notes of topic transverse myelitis
Reading File
Finding Sources
Searching the Web
transverse myelitis diagnosis treatment guidelines 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching PubMed
"transverse myelitis" AND diagnosis AND treatment
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Here are complete, well-structured notes on transverse myelitis.
Transverse Myelitis - Complete Notes
1. Definition
Transverse myelitis (TM) is an acute or subacute inflammatory demyelinating disorder of the spinal cord that interrupts ascending and descending pathways, producing a clinical triad of:
- Motor deficits (paraparesis/paraplegia)
- Sensory deficits (with a sensory level)
- Autonomic dysfunction (bladder, bowel, sexual)
The word "transverse" implies involvement across the full cross-section of the cord at a given level, though this is not always complete.
2. Epidemiology
- Incidence: approximately 1-8 per million per year
- Bimodal age distribution: peaks at 10-19 years and 30-39 years
- No strong sex predilection in idiopathic TM, but NMOSD-related TM is more common in women
- Thoracic cord is most commonly affected (60-70% of cases); cervical cord involvement is less common
3. Etiology and Classification
TM is heterogeneous. No cause is identified in ~30% of cases (idiopathic).
Primary Categories:
| Category | Examples |
|---|---|
| Idiopathic / Isolated TM | No identifiable cause (~30%) |
| Demyelinating disease | Multiple sclerosis (MS), NMOSD |
| Parainfectious / Post-infectious | Follows viral illness in ~30% of patients |
| Infectious (direct) | HSV, VZV, CMV, EBV, enterovirus, rabies, TB, Lyme, syphilis |
| Post-vaccinal | Rabies, polio vaccines |
| Autoimmune / Connective tissue disease | SLE, Sjögren syndrome, antiphospholipid syndrome, mixed CTD, sarcoidosis |
| Vascular | Spinal cord ischemia, dural AV fistula |
| Paraneoplastic | Associated with systemic malignancy |
Key Subtypes:
Longitudinally Extensive Transverse Myelitis (LETM):
- Signal abnormality extending >3 vertebral segments on MRI
- Hallmark of NMOSD (NMO spectrum disorder)
- Associated with anti-AQP4 (aquaporin-4) antibodies
Acute Partial TM (APTM):
- Signal abnormality extending <2 vertebral segments
- More characteristic of MS involvement
4. Pathophysiology
- Underlying mechanism varies by etiology
- Common pathway: inflammatory infiltration of the spinal cord → demyelination ± axonal damage → disruption of motor, sensory, and autonomic tracts
- In NMOSD: antibodies target aquaporin-4 water channels on astrocytic end-feet → astrocyte destruction → secondary oligodendrocyte death and demyelination
- In post-infectious TM: molecular mimicry or bystander activation of immune response
- Lesions in TM tend to involve >2/3 of the cross-sectional area of the cord (vs. MS lesions which involve <1/2)
5. Clinical Features
Onset
- Usually rapid: 66% reach maximal deficit within 24 hours; may progress over days to weeks
- Often preceded by back pain or radicular pain at the level of the lesion
- Low-grade fever may be present (post-infectious)
Classic Triad:
A. Motor Deficits
- Acute phase (spinal shock): flaccid paralysis, hypotonia, hyporeflexia below the lesion
- Subacute/chronic phase: spastic paraplegia, hyperreflexia, clonus, bilateral Babinski signs
- Loss of superficial abdominal and cremasteric reflexes
- Extension posturing with incomplete/high lesions; flexion posturing with complete lower cord lesions
B. Sensory Deficits
- Sensory level on the trunk - most valuable localizing sign
- All modalities impaired below the lesion
- Band-like radicular pain or paresthesias at the level of the lesion
- With extramedullary compression, sensory level may be several segments below the actual lesion (due to somatotopic organization of spinothalamic tract - sacral fibers are most superficial)
C. Autonomic Dysfunction
- Bladder: urinary retention, overflow incontinence, or urgency
- Bowel: constipation or incontinence
- Sexual dysfunction
- Cardiovascular: hypo- or hypertension, brady- or tachycardia (in high cervical lesions)
6. Investigations
A. MRI Spine (with and without gadolinium) - Investigation of Choice
- T2-weighted: intramedullary high signal (hyperintensity) with cord swelling
- Gadolinium enhancement: present in active inflammation
- TM lesions: involve >2/3 of cord cross-section on axial views
- LETM (>3 segments): points toward NMOSD
- Short lesion (<2 segments, peripheral, dorsal): points toward MS
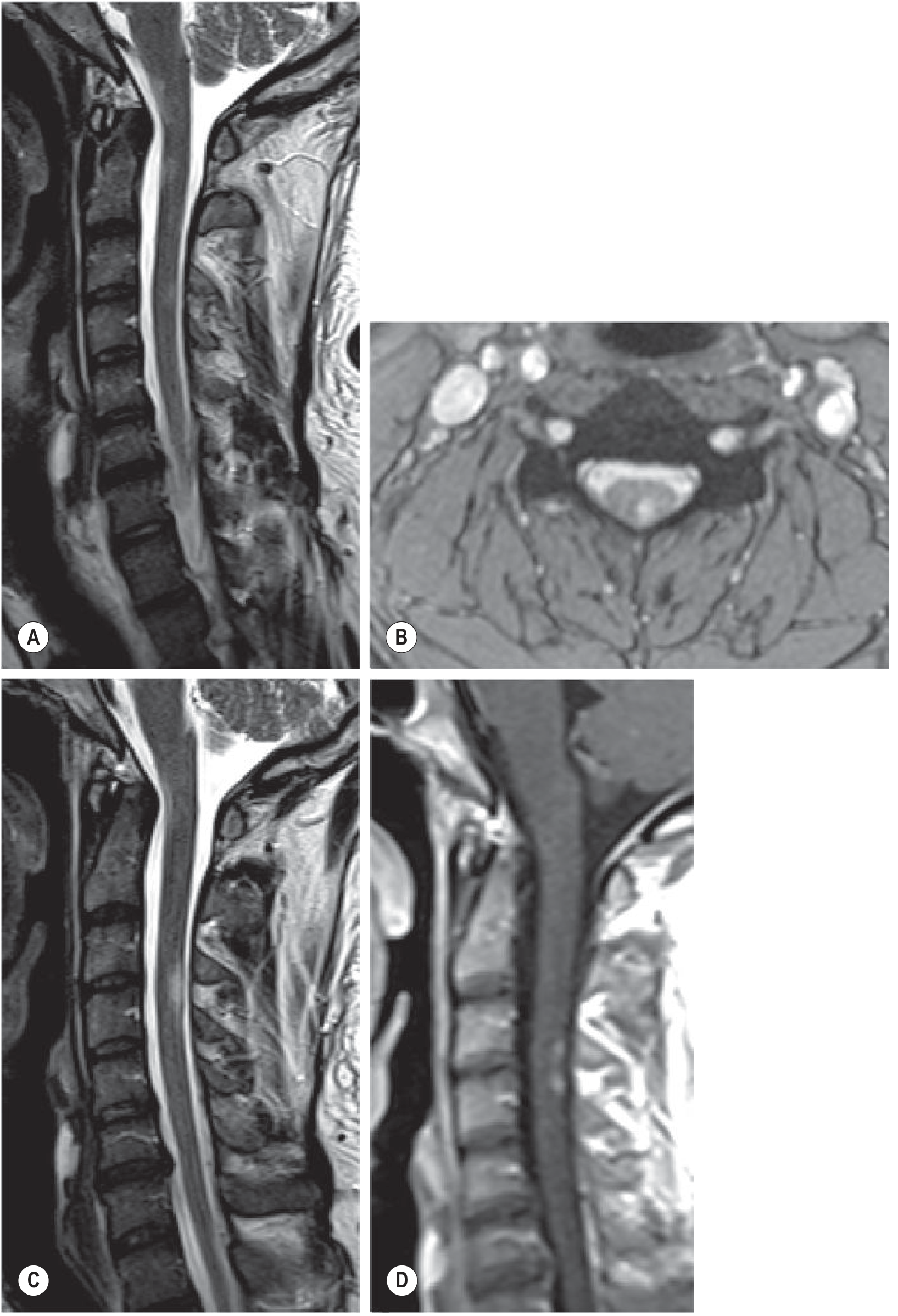
MRI of cervical spine: sagittal T2 images showing intramedullary hyperintense lesions with cord swelling and contrast enhancement - Grainger & Allison's Diagnostic Radiology
If MS is suspected: also obtain brain MRI - cerebral white matter lesions support diagnosis of MS even if asymptomatic.
B. CSF Analysis (Lumbar Puncture)
- Normal in 40% of cases
- Abnormal (60%): mild lymphocytic pleocytosis + elevated protein
- Oligoclonal bands (IgG): suggest MS
- CSF is not diagnostic but helps exclude infection and support inflammation
C. Blood Tests
- Anti-AQP4 (anti-aquaporin-4) antibodies / NMO-IgG - key test for NMOSD
- Anti-MOG (myelin oligodendrocyte glycoprotein) antibodies - seronegative NMOSD variant
- ANA, anti-dsDNA, antiphospholipid antibodies - screen for SLE and autoimmune CTD
- Vitamin B12, folate
- Infectious workup (viral serology, TB, Lyme, syphilis) as clinically indicated
D. Other
- Somatosensory and motor evoked potentials: demonstrate conduction delay across the lesion
- Nerve conduction studies / EMG: to rule out peripheral nerve or neuromuscular disease
7. Diagnostic Criteria (Transverse Myelitis Consortium Working Group)
Inclusion Criteria:
- Sensory, motor, or autonomic dysfunction attributable to the spinal cord
- Bilateral signs/symptoms (not necessarily symmetrical)
- Clearly defined sensory level
- Inflammation demonstrated by CSF pleocytosis, elevated IgG index, or MRI gadolinium enhancement (if none present, repeat MRI in 2-7 days)
- Nadir between 4 hours and 21 days of onset
Exclusion Criteria:
- History of prior radiation to spine
- Clear arterial distribution of deficit (vascular)
- Extramedullary compressive etiology on MRI
- Abnormal flow voids suggesting AV malformation
- Connective tissue disease serologically negative (does not exclude)
8. Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Spinal cord compression (disc, tumor, abscess) | No CSF pleocytosis; structural lesion on MRI; often gradual |
| MS | Short cord lesion (<2 segments), asymmetric, brain lesions present |
| NMOSD | LETM (>3 segments), AQP4-Ab positive, often severe and bilateral |
| Spinal cord infarct | Sudden onset, anterior cord syndrome, DWI restriction on MRI |
| Spinal epidural abscess (SEA) | Fever, elevated CRP/ESR, bacteremia, epidural collection on MRI |
| Spinal epidural hematoma | History of anticoagulation/trauma; blood on MRI |
| Vitamin B12 deficiency (SACD) | Subacute combined degeneration; posterior + lateral columns; low B12 |
| Paraneoplastic myelopathy | Known malignancy; paraneoplastic antibodies |
9. Management
A. Acute Phase (First-line)
High-dose IV Corticosteroids:
- Methylprednisolone 1 g IV daily for 3-5 days
- Mechanism: reduces inflammation, stabilizes blood-brain/spinal cord barrier
- Standard of care especially for NMOSD-related TM
- Evidence is limited for idiopathic TM but widely used
B. Second-line (Steroid-refractory)
Plasma Exchange (Plasmapheresis):
- 5-7 exchanges over 10-14 days
- Used when patients fail to improve with steroids
- Removes pathogenic antibodies (especially useful in AQP4-Ab positive NMOSD)
IV Immunoglobulin (IVIG):
- Used in selected cases, especially post-infectious or MOG-Ab associated TM
C. Long-term / Preventive (NMOSD)
To prevent recurrent attacks in NMOSD:
- Azathioprine (with or without oral prednisolone)
- Mycophenolate mofetil
- Rituximab (anti-CD20)
- Newer biologics: Eculizumab, Inebilizumab, Satralizumab - FDA-approved for AQP4-Ab+ NMOSD
D. Symptomatic and Supportive
| Problem | Management |
|---|---|
| Spasticity | Baclofen, tizanidine; intrathecal baclofen for severe cases |
| Neuropathic pain | Gabapentin, pregabalin, amitriptyline |
| Bladder dysfunction | Intermittent catheterization, anticholinergics |
| Bowel dysfunction | Bowel training, laxatives |
| DVT prophylaxis | LMWH, compression stockings |
| Pressure ulcers | Regular turning, pressure-relieving mattress |
| Rehabilitation | Physiotherapy, occupational therapy, speech therapy (if bulbar involved) |
10. Prognosis
- Clinical course is highly variable
- Most patients with idiopathic TM show at least partial recovery beginning within 1-3 months
- Maximal improvement usually by 3-6 months
Outcome breakdown (idiopathic TM):
| Outcome | Percentage |
|---|---|
| Good recovery (near-normal function) | ~30% |
| Fair recovery (moderate disability) | ~25% |
| Poor outcome (severe disability) | ~30% |
| Mortality at 5 years | ~15% |
Poor Prognostic Factors:
- Rapid onset to nadir (<24 hours)
- Severe deficits at nadir (complete paraplegia)
- Back pain at onset
- Spinal shock at presentation
- NMOSD (high relapse rate, cumulative disability)
- AQP4-Ab positivity
Risk of MS:
- Up to one-third of patients do not have evidence of disseminated demyelination at 5 years (monophasic course)
- Those with brain MRI lesions + oligoclonal bands at presentation have higher risk of converting to MS
- Risk of MS progression after an isolated TM episode is similar to that after a first episode of optic neuritis
11. TM vs. MS vs. NMOSD - Comparison Table
| Feature | TM (idiopathic) | MS-associated TM | NMOSD-associated TM |
|---|---|---|---|
| Cord lesion length | Variable | <2 segments | >3 segments (LETM) |
| Cross-section involvement | >2/3 | <1/2 | >2/3, "bright spotty" |
| Enhancement | Variable | Common, short | "Shaggy ring" pattern |
| AQP4-Ab | Negative | Negative | Positive (~80%) |
| Brain lesions | Absent | Present (Dawson fingers, etc.) | Variable |
| Course | Usually monophasic | Relapsing-remitting | Relapsing (80%) |
| Severity | Moderate | Usually incomplete | Often severe/bilateral |
| Optic neuritis | Absent | May occur | Common (simultaneous or sequential) |
Sources:
- Rosen's Emergency Medicine, 10e
- Adams and Victor's Principles of Neurology, 12e
- Bradley and Daroff's Neurology in Clinical Practice
- Localization in Clinical Neurology, 8e
- Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.