My patient is 26 year old male comes with complain of ear pain right side with white discharge since two days'
Reading File
Finding Sources
Finding Sources
Searching PubMed
otitis externa management treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Let me compile the full clinical response.
Clinical Assessment: Right Ear Pain with White Discharge (2 days)
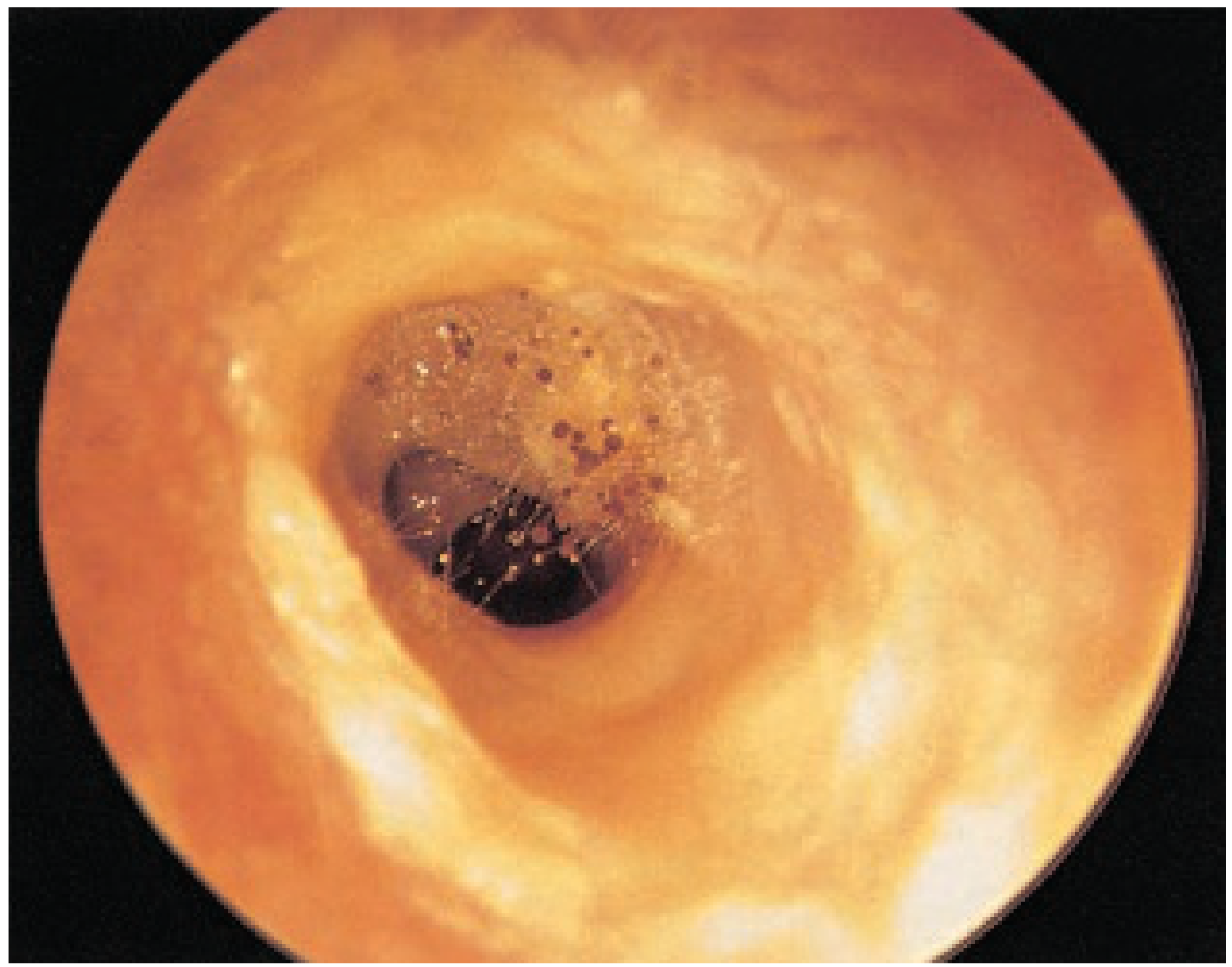
Most Likely Diagnosis: Otomycosis (Fungal Otitis Externa)
In a 26-year-old male presenting with otalgia + white discharge of 2 days' duration, the leading diagnosis is otomycosis - fungal infection of the external auditory canal. The white color of the discharge is the key differentiating feature.
"The commonest finding [in otomycosis] is a black, grey, green, yellow or white discharge with debris that is often said to resemble wet newspaper. Occasionally, debris is seen with visible fungal hyphae."
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2
Differential Diagnoses
| Condition | Features favoring | Features against |
|---|---|---|
| Otomycosis | White discharge, 2-day duration, young adult | - |
| Acute Diffuse Otitis Externa (bacterial) | Otalgia, discharge | Bacterial discharge is usually yellow/green/purulent |
| Acute Localized OE (furuncle) | Ear pain, young adult | Usually no significant discharge, S. aureus |
| Acute Otitis Media with perforation | Ear pain, discharge | AOM rare in 26-year-old without URI history, discharge typically pulsatile |
History to Elicit
- Swimming or water exposure recently (classic predisposing factor)?
- Prior use of antibiotic ear drops (prolonged topical antibiotics predispose to fungal OE)?
- Diabetes or immunocompromise?
- Ear itching (itching is very prominent in otomycosis)?
- Any recent ear manipulation/cotton bud use?
- Upper respiratory tract infection symptoms (points toward AOM)?
- Hearing loss (conductive loss common in OE due to canal oedema/debris)?
Examination
Otoscopy findings to look for:
- Otomycosis: white/grey/black fluffy debris in canal resembling "wet newspaper," edematous erythematous canal walls, visible fungal hyphae
- Bacterial OE: diffuse erythema and edema with purulent discharge
- Tympanic membrane (TM): assess integrity - if TM is intact and normal, favors OE over AOM; if perforated, it changes management
Other examination:
- Tragal tenderness on pressure (pathognomonic for OE - suggests external canal involvement)
- Preauricular/postauricular lymphadenopathy
- Periauricular erythema/swelling (rules out perichondritis)
Management
For Otomycosis (most likely)
1. Aural Toilet (most important single treatment)
- Thorough cleaning and removal of fungal debris under microscopy or with suction
- "Toilet remains the most effective single treatment for otitis externa" - Scott-Brown's
- Avoid syringing (risk of complications)
2. Topical Antifungal Drops
- Clotrimazole 1% ear drops - first-line; 3 drops TDS for 2-4 weeks
- Flumethasone with clioquinol - alternative
- Continue for at least 2 weeks after resolution to prevent recurrence
3. Analgesia
- NSAIDs (ibuprofen) are excellent analgesics for OE
- Paracetamol as alternative
4. Advice
- Keep ear dry - avoid swimming, use cotton wool with petroleum jelly when bathing
- Do not insert cotton buds or any objects into the ear
- Follow up in 1-2 weeks
If Bacterial OE is confirmed instead
- Topical antibiotic-steroid combination (e.g., ciprofloxacin + dexamethasone drops, or neomycin + polymyxin B + hydrocortisone)
- Fluoroquinolone drops (e.g., ciprofloxacin) are preferred if TM status is uncertain - they are safe even with TM perforation
- Aminoglycoside drops are contraindicated if TM is perforated (ototoxic) - Rosen's Emergency Medicine
- No systemic antibiotics for uncomplicated OE in an immunocompetent patient
- If canal is severely edematous (lumen obliterated): insert a Pope otowick soaked in antibiotic/steroid drops for 24-48 hours to allow drops to reach the canal
Red Flags - When to Escalate
Alert for Malignant (Necrotizing) Otitis Externa if:
- Patient is diabetic or immunocompromised
- Fails to respond to topical treatment after 2 weeks
- Severe unrelenting pain out of proportion
- Granulation tissue at the floor of canal (at bony-cartilaginous junction)
- Cranial nerve palsies (VII, IX, X, XII)
Necrotizing OE requires urgent CT scan (bony erosion), systemic ciprofloxacin (anti-Pseudomonal), and otolaryngology referral. - Rosen's Emergency Medicine
Summary of Management Plan
1. Otoscopy with careful TM assessment
2. Aural toilet (suction/dry mopping of debris)
3. Clotrimazole 1% ear drops TDS × 3-4 weeks (if otomycosis)
OR Ciprofloxacin/dexamethasone drops BD × 7-10 days (if bacterial OE)
4. NSAIDs for analgesia
5. Ear dry precautions
6. Review in 1-2 weeks
7. Swab only if resistant/high-risk case
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2 (Ch. 78); Rosen's Emergency Medicine; Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.