Exlajm brachia plesus
Reading File
Searching the Web
brachial plexus anatomy roots trunks cords branches
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Here is a complete explanation of the brachial plexus, based on Gray's Anatomy for Students.
Brachial Plexus (Plexus Brachialis)
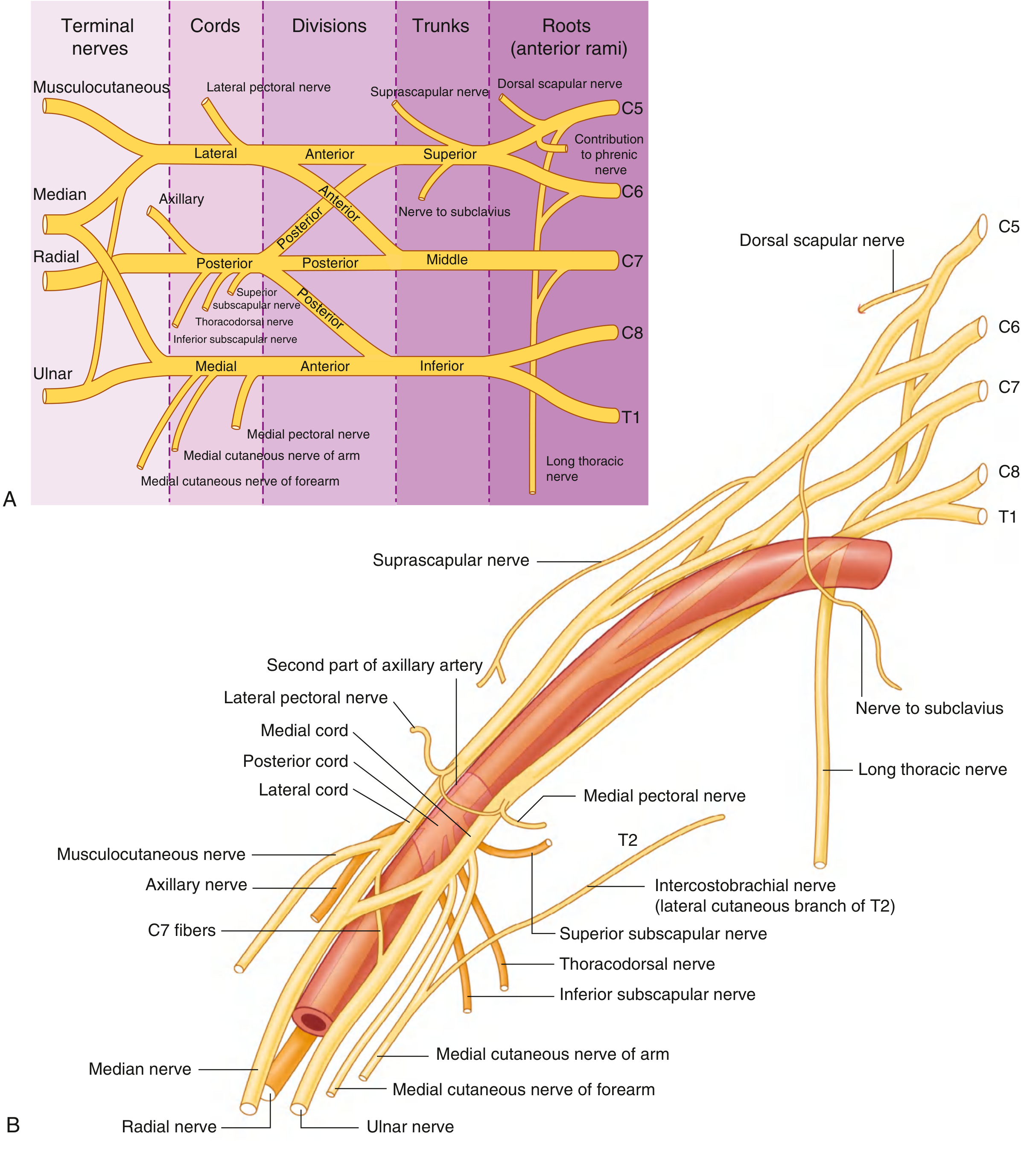
The brachial plexus is a somatic nerve plexus formed by the anterior rami of C5 to C8, and most of T1. It originates in the neck, passes laterally and inferiorly over rib I, and enters the axilla. All major nerves supplying the upper limb originate from it.
Its organization follows a fixed sequence: Roots → Trunks → Divisions → Cords → Branches
A useful mnemonic: Real Texans Drink Cold Beer
Anatomy Diagram

1. Roots (Anterior Rami)
The roots are the anterior rami of C5, C6, C7, C8, and T1. They pass between the anterior scalene and middle scalene muscles and lie posterior to the subclavian artery. Each root receives gray rami communicantes from the sympathetic trunk, carrying postganglionic sympathetic fibers.
2. Trunks
The three roots re-organize into three trunks as they cross the base of the posterior triangle:
| Trunk | Formation |
|---|---|
| Superior (Upper) | C5 + C6 |
| Middle | C7 alone |
| Inferior (Lower) | C8 + T1 |
The inferior trunk lies on rib I posterior to the subclavian artery.
3. Divisions
Each trunk splits into an anterior and a posterior division (6 divisions total). No peripheral nerves arise directly from the divisions.
- Anterior divisions - supply the anterior (flexor) compartments
- Posterior divisions - supply the posterior (extensor) compartments
4. Cords
The divisions recombine around the axillary artery to form 3 cords, named by their position relative to the second part of the axillary artery:
| Cord | Formation | Roots |
|---|---|---|
| Lateral cord | Anterior divisions of superior + middle trunks | C5-C7 |
| Medial cord | Anterior division of inferior trunk | C8-T1 |
| Posterior cord | All three posterior divisions | C5-T1 |
5. Branches
The full picture of branches is shown in the diagram below:
From the Roots
| Nerve | Root(s) | Supplies |
|---|---|---|
| Dorsal scapular nerve | C5 | Rhomboid major, rhomboid minor (+ levator scapulae) |
| Long thoracic nerve | C5, C6, C7 | Serratus anterior |
| Contribution to phrenic nerve | C5 | Diaphragm (small contribution) |
From the Superior Trunk
| Nerve | Supplies |
|---|---|
| Suprascapular nerve (C5, C6) | Supraspinatus, infraspinatus |
| Nerve to subclavius (C5, C6) | Subclavius muscle |
From the Lateral Cord
| Nerve | Supplies |
|---|---|
| Lateral pectoral nerve | Pectoralis major (clavicular head) |
| Musculocutaneous nerve | Coracobrachialis, biceps brachii, brachialis; skin of lateral forearm |
| Lateral root of median nerve | Forms part of median nerve |
From the Medial Cord
| Nerve | Supplies |
|---|---|
| Medial pectoral nerve | Pectoralis minor and major |
| Medial cutaneous nerve of arm | Skin of medial arm |
| Medial cutaneous nerve of forearm | Skin of medial forearm to wrist |
| Medial root of median nerve | Forms part of median nerve |
| Ulnar nerve | Intrinsic hand muscles, flexor carpi ulnaris, medial FDP; skin of little finger and medial ring finger |
From the Posterior Cord
| Nerve | Supplies |
|---|---|
| Upper subscapular nerve | Subscapularis (upper part) |
| Thoracodorsal nerve | Latissimus dorsi |
| Lower subscapular nerve | Subscapularis (lower part), teres major |
| Axillary nerve | Deltoid, teres minor; skin over deltoid region |
| Radial nerve | All posterior compartment muscles of arm and forearm; dorsal hand skin |
The Median Nerve
Formed anterior to the third part of the axillary artery by union of the lateral and medial roots from the lateral and medial cords respectively. It innervates most anterior forearm muscles, thenar muscles, and skin of the lateral 3.5 fingers on the palm.
Clinical Summary of Cord/Root Injuries
| Injury | Level | Classic Name | Features |
|---|---|---|---|
| C5-C6 avulsion | Upper trunk | Erb's palsy | "Waiter's tip" - arm adducted, medially rotated, forearm pronated |
| C8-T1 avulsion | Lower trunk | Klumpke's palsy | Claw hand + Horner's syndrome (if T1 preganglionic) |
| Long thoracic nerve injury | C5-C7 roots | - | Medial winging of scapula (serratus anterior paralysis) |
| Axillary nerve injury | Posterior cord | - | Deltoid weakness, loss of shoulder abduction, loss of sensation over deltoid |
| Radial nerve injury | Posterior cord | - | Wrist drop, loss of finger/thumb extension |
- Gray's Anatomy for Students, pp. 858-862
Digitalis
Finding Sources
Searching the Web
digitalis digoxin pharmacology mechanism clinical use toxicity
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
I now have everything needed for a thorough answer. Here is a complete pharmacology summary of Digitalis:
Digitalis (Cardiac Glycosides)
Source and Chemistry
Digitalis is the genus of plants (foxglove) from which most medically useful cardiac glycosides are derived. William Withering published the first systematic clinical description in 1785 using Digitalis purpurea (purple foxglove). Digoxin - the prototype and only cardiac glycoside used clinically in the USA - is obtained from Digitalis lanata (white foxglove).
Structurally, all cardiac glycosides (cardenolides) consist of:
- A steroid nucleus
- A lactone ring at position 17
- Sugar moieties at carbon 3
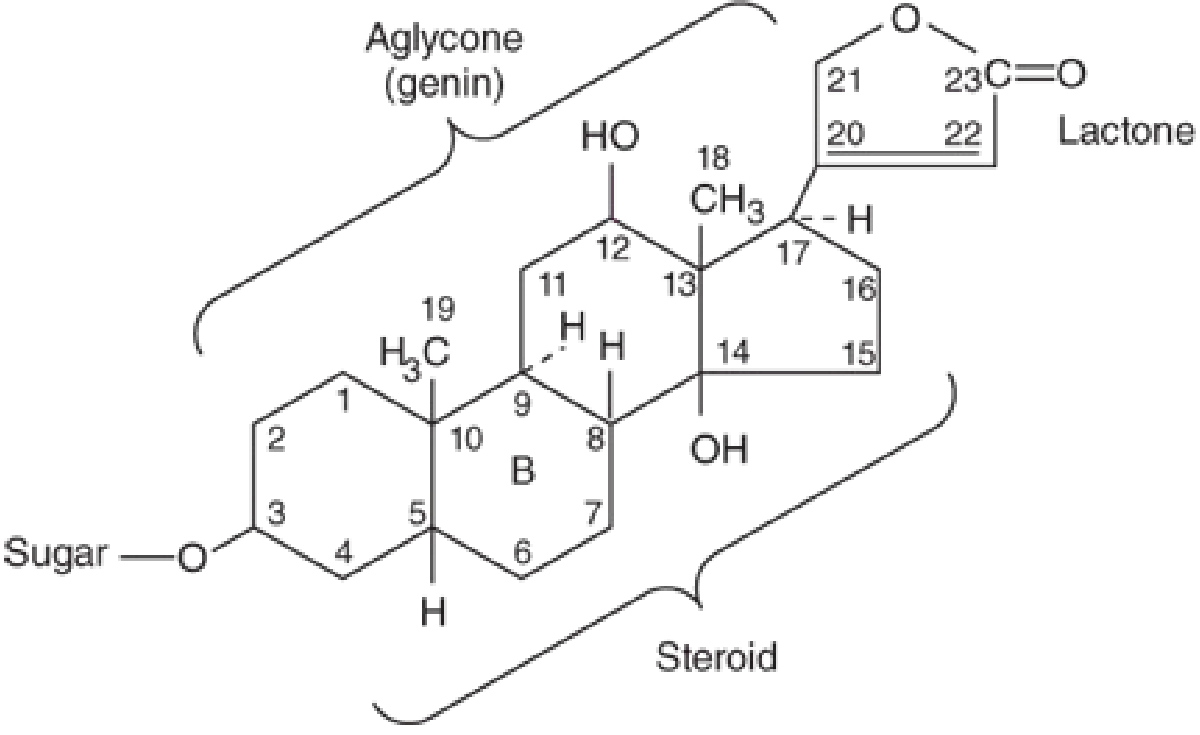
Other plant sources containing similar glycosides: oleander, lily of the valley, milkweed - ingestion can cause poisoning.
Pharmacokinetics
| Parameter | Details |
|---|---|
| Oral bioavailability | 65-80% |
| Distribution | Wide - including CNS |
| Metabolism | Minimal hepatic metabolism |
| Excretion | ~2/3 excreted unchanged by kidneys |
| Half-life | 36-40 hours (normal renal function) |
| Renal impairment | Dose adjustment mandatory - clearance proportional to creatinine clearance |
Mechanism of Action
Primary: Na⁺/K⁺-ATPase Inhibition
Digitalis inhibits the Na⁺/K⁺-ATPase (the "sodium pump") on cell membranes. This leads to a two-step cascade that increases contractility:
- ↓ Na⁺/K⁺-ATPase → intracellular Na⁺ accumulates
- ↑ Intracellular Na⁺ → Na⁺/Ca²⁺ exchanger (NCX) exports less Ca²⁺ → intracellular Ca²⁺ rises
- Ca²⁺ is stored in the sarcoplasmic reticulum (SR) via SERCA and released during systole → positive inotropy
Indirect (Autonomic) Effects
Digitalis has cardioselective parasympathomimetic (vagotonic) effects - it enhances vagal tone to the AV node, slowing conduction. This is the basis of its rate-control effect in atrial fibrillation.
Pharmacodynamic Effects
Mechanical Effects
- Positive inotropy - increased force and rate of development of tension
- Increased intracellular free Ca²⁺ during systole
- Occurs in both normal and failing myocardium
Electrical Effects
| Tissue | Therapeutic Dose | Toxic Dose |
|---|---|---|
| Sinus node | ↓ Rate | ↓ Rate |
| Atrial muscle | ↓ Refractory period | ↓ Refractory period, arrhythmias |
| AV node | ↓ Conduction velocity, ↑ refractory period | ↓ Refractory period, arrhythmias |
| Purkinje / ventricular muscle | ↓ Refractory period (slight) | Oscillatory depolarizations, arrhythmias |
At toxic concentrations, digitalis causes delayed afterdepolarizations (DADs) due to Ca²⁺ overload of the SR - leading to triggered activity and arrhythmias.
Clinical Uses
1. Heart Failure with Reduced Ejection Fraction (HFrEF)
- Used when diuretics and ACE inhibitors have failed to control symptoms
- Only ~50% of patients in sinus rhythm respond
- Reduces hospitalization and deaths from progressive HF
- Target serum level: ≤ 0.9 ng/mL (mortality increases at levels > 1.5 ng/mL)
- Typical dose: 0.125-0.25 mg/day orally
2. Atrial Fibrillation / Flutter (Rate Control)
- AV node slowing (vagotonic effect) reduces ventricular rate
- Higher serum levels may be needed than in HF
3. Paroxysmal SVT
- Largely replaced by calcium channel blockers and adenosine
Absolute contraindication: Wolff-Parkinson-White syndrome + atrial fibrillation (digitalis can accelerate accessory pathway conduction → ventricular fibrillation)
Toxicity
Digitalis has an extremely narrow therapeutic window - toxic effects may appear before therapeutic effects in some patients.
Factors that Precipitate Toxicity
| Factor | Mechanism |
|---|---|
| Hypokalemia | K⁺ and digitalis compete for Na⁺/K⁺-ATPase binding; low K⁺ → more enzyme inhibition |
| Hypercalcemia | Accelerates Ca²⁺ overload of SR → more automaticity |
| Hypomagnesemia | Mg²⁺ effects are opposite to Ca²⁺; low Mg²⁺ worsens toxicity |
| Renal failure | Reduced digoxin clearance → drug accumulation |
| Drug interactions | Amiodarone, verapamil, quinidine raise digoxin levels |
| Hypothyroidism | Increased sensitivity |
Features of Toxicity
Cardiac (most dangerous):
- AV junctional rhythm
- Premature ventricular contractions (PVCs)
- Bigeminal rhythm
- Ventricular tachycardia
- 2nd/3rd degree AV block
- "Digitalis can cause virtually any arrhythmia"
- Serum level > 2.0 ng/mL is associated with overt toxicity
- Important: Electrical cardioversion is contraindicated in digitalis-induced arrhythmias (except for VF)
GI (most common non-cardiac):
- Anorexia, nausea, vomiting, diarrhea
CNS:
- Visual disturbances (color vision aberrations - classic yellow-green halos)
- Disorientation and hallucinations (especially in elderly)
- Vagal/chemoreceptor trigger zone stimulation
Endocrine:
- Gynecomastia (structural similarity to estrogens)
Management of Toxicity
| Severity | Treatment |
|---|---|
| Mild (GI/visual) | Reduce dose, monitor ECG and electrolytes |
| Arrhythmias with normal K⁺ | Oral potassium supplementation |
| Bradycardia/AV block | Atropine; temporary pacing if needed |
| Severe/life-threatening | Digoxin immune Fab (antidigoxin antibody fragments) |
Digoxin immune Fab (Digibind/DigiFab):
- Purified Fab fragments from digoxin-specific antisera
- Effective against most plant-derived glycosides
- Dose calculated from estimated ingested dose or total body digoxin burden
- Given IV over 30-60 minutes
- Also potentially useful in eclampsia/preeclampsia
Note: In severe toxicity, serum K⁺ is often already elevated (efflux from intracellular compartment); additional potassium must be given cautiously.
Key Clinical Points
-
Serum digoxin level ≤ 0.9 ng/mL is the current target in HFrEF (AHA/ACC/HFSA 2022 guidelines); levels > 1.5 ng/mL increase mortality
-
Digoxin does not reduce overall mortality in HF - it reduces hospitalizations but may increase sudden death
-
Hypokalemia from loop diuretics (commonly co-prescribed) is a major precipitant of toxicity
-
Always check renal function before and during therapy
-
Katzung's Basic and Clinical Pharmacology, 16th Ed., pp. 338-346
-
Braunwald's Heart Disease, p. 164
This is a shared conversation. Sign in to Orris to start your own chat.