Difference between slow and fast adapting receptors
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a detailed comparison of slow- and fast-adapting receptors, drawn from Ganong's, Costanzo, and Kandel's Principles of Neural Science.
Slow-Adapting (SA) vs. Fast-Adapting (RA) Receptors
Core Concept: Receptor Adaptation
When a stimulus of constant strength is maintained on a sensory receptor, the frequency of action potentials in its sensory nerve declines over time. This is called receptor adaptation. Based on how quickly this decline occurs, receptors are classified as:
- Slowly adapting (SA) = tonic receptors
- Rapidly adapting (RA) = phasic receptors
Side-by-Side Comparison
| Feature | Slow-Adapting (SA/Tonic) | Fast-Adapting (RA/Phasic) |
|---|---|---|
| Firing pattern | Sustained discharge throughout the stimulus | Fires at onset (and often offset) only; silent during steady stimulus |
| What they detect | Stimulus intensity and duration | Stimulus change, velocity, and movement |
| Functional role | Signal that a stimulus is still present | Signal that a stimulus has started or stopped |
| Adaptation speed | Slow (continue firing for seconds to minutes) | Rapid (stop firing within milliseconds) |
| SA type 1 (SA1) | Merkel cells - superficial skin, small receptive field; encodes fine texture and sustained pressure | - |
| SA type 2 (SA2) | Ruffini endings - deep skin, large receptive field; encodes stretch and joint rotation | - |
| RA type 1 (RA1) | - | Meissner corpuscles - superficial skin, small receptive field; encodes flutter, tapping, point discrimination |
| RA type 2 (RA2) | - | Pacinian corpuscles - deepest (subcutaneous); the most rapidly adapting; encodes vibration |
| Also includes | Muscle spindles, nociceptors | Hair follicle receptors |
Spike Train Patterns (from Kandel)
The figure below illustrates the four mechanoreceptors of the hand and their neural spike trains in response to a ramp-and-hold stimulus:
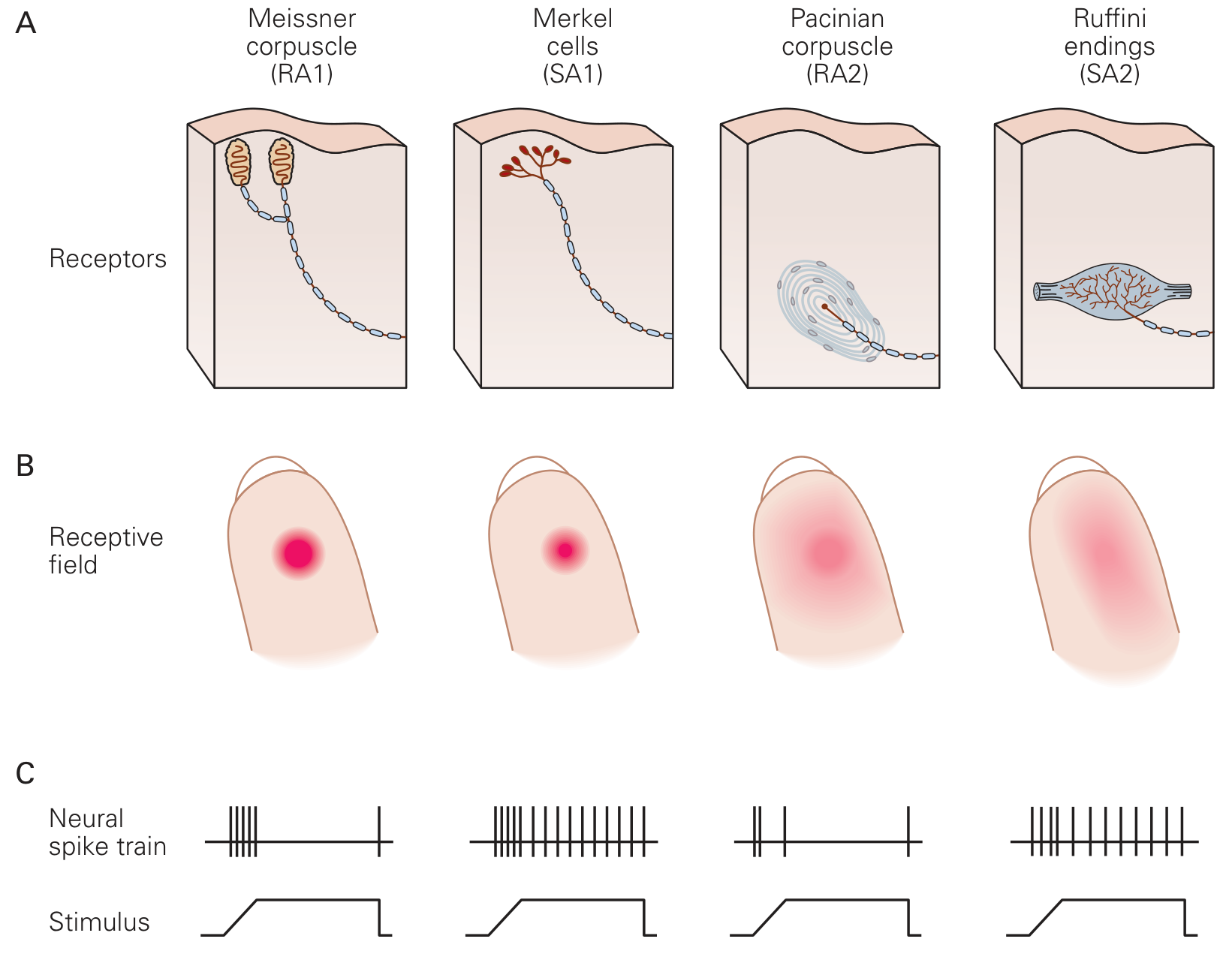
- RA fibers (Meissner, Pacinian): fire a burst at onset and offset of pressure, then go silent
- SA fibers (Merkel, Ruffini): fire continuously throughout the applied pressure
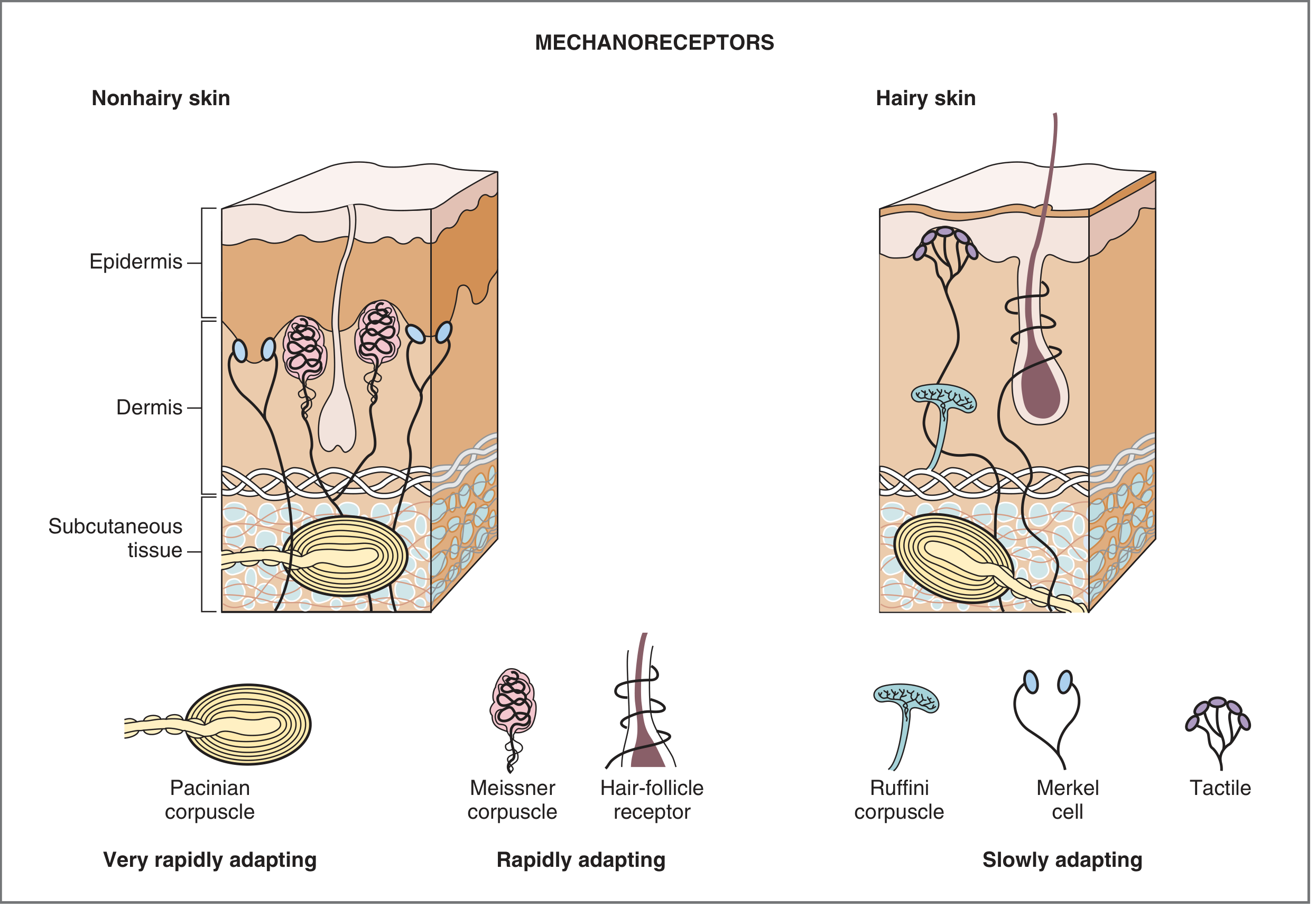
Mechanoreceptors Classified by Adaptation
Physiological Significance
The adaptive properties are not random - they serve specific functions:
- Why SA receptors are needed: Postural control depends on muscle spindle input remaining active as long as muscle length is unchanged. Nociceptors adapting slowly means pain persists as a warning as long as tissue damage is present. - Ganong's, p. 174
- Why RA receptors are needed: Light touch on skin would be constantly distracting if it persisted; phasic firing lets us focus on changes rather than constant background sensation. Pacinian corpuscles' extreme speed (firing to vibration at up to 300 Hz) allows detection of fine surface textures through tools held in the hand.
Beyond the Skin: Airways
Slow/fast adapting classification applies beyond cutaneous receptors. In the airways:
-
Slowly adapting pulmonary stretch receptors (PSRs): activated by lung inflation; mediate the Hering-Breuer reflex
-
Rapidly adapting receptors (irritant receptors): respond to chemical irritants (serotonin, prostaglandins, ammonia, cigarette smoke) and trigger cough/bronchoconstriction
-
Ganong's Review of Medical Physiology, 26th ed.; Costanzo Physiology, 7th ed.; Kandel Principles of Neural Science, 6th ed.
Law of projection in receptors
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching the Web
law of projection sensory receptors physiology definition examples
Finding Sources
Reading File
Reading Web Page
https://webweb.ams3.cdn.digitaloceanspaces.com/data/mgmunive…
Here is a complete explanation of the Law of Projection, contextualized within the broader properties of sensory receptors.
Law of Projection
Definition
The Law of Projection is a fundamental property of sensory coding that states:
Regardless of where along a sensory pathway a nerve fiber is stimulated, the resulting sensation is always consciously perceived (projected) at the location of the original receptor - the peripheral end of that fiber.
This is essentially the brain's positional sense - the ability to assign the origin of a stimulus in space or on the body surface, even when the actual point of stimulation is somewhere along the nerve pathway, not at the receptor itself.
The law is sometimes called the "doctrine of projection" and is listed as one of the five key properties of sensory receptors, alongside:
- Specificity (Law of Adequate Stimulus)
- Adaptation (tonic vs. phasic)
- Muller's Doctrine of Specific Nerve Energies
- Law of Projection
- Law of Intensity Discrimination
Why Does This Happen?
The brain has no direct access to the outside world. It only receives electrical signals traveling along labeled sensory lines. It has learned through experience that signals arriving via a particular afferent fiber always originate from the same peripheral location. So no matter where that fiber is excited - at its tip, its middle, or centrally - the brain interprets the signal as coming from the receptor end.
This is related to the concept of sensory coding for location: the receptive field of a sensory unit defines where in the body or space a stimulus appears to originate, and this mapping is fixed in the brain. - Ganong's Review of Medical Physiology, 26th ed.
Classic Examples
| Example | Explanation |
|---|---|
| "Funny bone" sensation | Tapping the ulnar nerve at the medial epicondyle of the elbow stimulates the nerve trunk mid-course, yet you feel tingling and numbness in the ring and little fingers - the peripheral territory of that nerve, not at the elbow |
| Phantom limb pain | After amputation, the residual nerve fibers or central reorganization generates signals in pathways that previously carried sensation from the missing limb. The brain projects the sensation to the amputated limb (which no longer exists). Between 50-80% of amputees experience phantom sensations - Ganong's, p. 179 |
| Referred pain | Visceral pain (e.g., cardiac ischemia felt in the left arm and jaw) occurs because afferents from viscera share central pathways with somatic afferents from the skin; the brain projects the pain to the body surface area whose receptors normally use that pathway |
| Pressing on the eyeball | Mechanical pressure on the eye stimulates retinal photoreceptor axons mid-pathway; you perceive flashes of light ("phosphenes"), not pressure - because the brain projects the signal to the visual field, not the finger pushing |
| Spinal cord stimulation | In phantom limb treatment, electrodes placed next to the spinal cord stimulate afferent pathways centrally; patients feel tingling in the phantom limb, not at the electrode site - Ganong's, p. 180 |
Relationship to Other Sensory Laws
The Law of Projection works hand-in-hand with Muller's Doctrine of Specific Nerve Energies: not only is the sensation projected to the receptor's peripheral location (projection), but the quality of sensation is also always that of the receptor's modality (specific energy). Together these explain why stimulating the optic nerve electrically produces light (not pain), and that light is perceived as coming from the visual field - not from inside the skull.
Clinical Relevance
- Referred pain in myocardial infarction (left arm/jaw), appendicitis (periumbilical then RIF), and diaphragmatic irritation (shoulder-tip pain) all operate on this principle
- Trigger points and radiculopathy - pressure on a nerve root (e.g., L4/L5 disc herniation) causes pain and tingling projected to the dermatome supplied by that root, not to the spine
- Tinel's sign - tapping a regenerating or compressed nerve produces tingling at the peripheral distribution, used clinically to track nerve regeneration
This is a shared conversation. Sign in to Orris to start your own chat.