Anemia
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Anemia - Comprehensive Medical Student Guide
Definition
Anemia is defined as blood counts below normal for a given population. In practical terms: Hb < 13.5 g/dL in adult males, < 12 g/dL in non-pregnant adult females.
Classification
There are two complementary schemes used in clinical practice.
Scheme 1: By MCV (Red Cell Size)
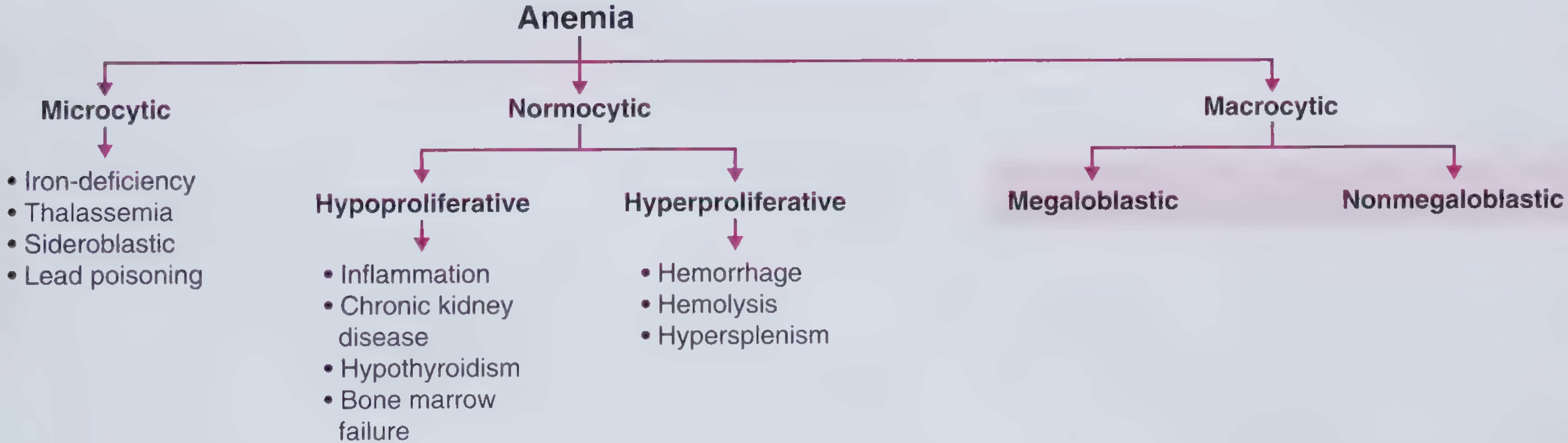
From Frameworks for Internal Medicine - Lippincott Williams & Wilkins
| MCV | Category | Key Causes |
|---|---|---|
| Low (<80 fL) | Microcytic | Iron deficiency, thalassemia, anemia of inflammation (sometimes), sideroblastic anemia, lead poisoning |
| Normal (80-100 fL) | Normocytic | Aplastic anemia, renal disease, endocrinopathies, acute blood loss, early iron deficiency, marrow invasion, myeloma |
| High (>100 fL) | Macrocytic | B12/folate deficiency (oval macrocytes), alcohol, hypothyroidism, liver disease, myelodysplasia (round macrocytes) |
Key principle: Microcytosis results from any process interfering with hemoglobin production (less Hb = smaller cell). Macrocytosis from megaloblastic causes results from defective DNA synthesis, while non-megaloblastic macrocytosis is from membrane defects. - Harrison's 22E
Scheme 2: By Mechanism (Reticulocyte-Based)
- Elevated reticulocyte count → Hyperproliferative = increased RBC loss or destruction (hemolysis, hemorrhage)
- Low/normal reticulocyte count → Hypoproliferative = impaired production
At least 75% of all anemias are hypoproliferative. The most common cause is mild-to-moderate iron deficiency or inflammation. - Harrison's 22E
1. Iron Deficiency Anemia (IDA)
Most common anemia worldwide - affects ~1.2 billion people.
Pathophysiology
Iron is needed for heme synthesis (4 iron atoms per hemoglobin molecule, ~1 billion per RBC). Deficiency develops in stages:
- Depleted stores - serum ferritin falls (<15-30 µg/L), no anemia yet
- Iron-restricted erythropoiesis - transferrin saturation <15-20%, RBCs become hypochromic and microcytic
- Overt IDA - frank microcytic hypochromic anemia
Hepcidin is low in IDA, maximizing absorption. In inflammation, hepcidin rises, trapping iron in macrophages (functional iron deficiency).
Causes
- Blood loss (GI bleed, menstrual - most common in adults)
- Increased demand (pregnancy, infancy, adolescence)
- Poor intake / absorption (vegetarian diet, celiac disease, post-gastrectomy)
Lab Findings
| Test | IDA | Anemia of Inflammation |
|---|---|---|
| Serum iron | ↓ | ↓ |
| TIBC | ↑ | Normal or ↓ |
| Transferrin saturation | ↓ | ↓ |
| Ferritin | ↓ (<30 µg/L) | Normal or ↑ |
| Reticulocytes | Low | Low |
Ferritin is an acute-phase reactant - a ferritin >200 µg/L generally means adequate iron stores even in the face of low serum iron. - Harrison's 22E
Treatment
Oral iron (ferrous sulfate 325 mg TID); IV iron for malabsorption or intolerance. Treat the underlying cause.
2. Megaloblastic Anemia (B12 / Folate Deficiency)
Pathophysiology
Impaired DNA synthesis prevents normal nuclear maturation while cytoplasm continues to grow - nuclear-cytoplasmic dyssynchrony. All cell lines are affected, often causing pancytopenia. Intramedullary destruction leads to elevated LDH and indirect bilirubin.
Blood Smear (Classic Exam Image)
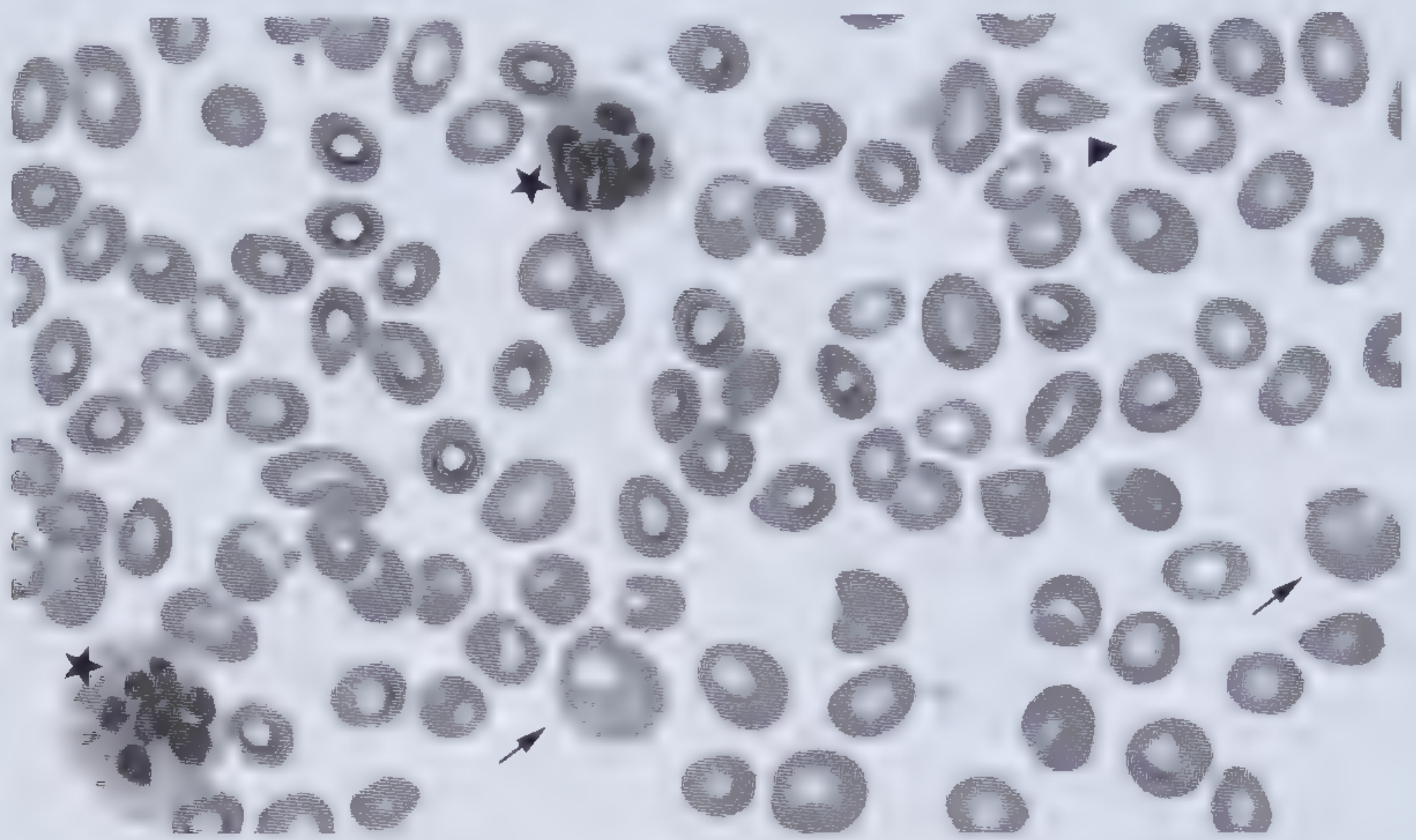
Peripheral smear from B12-deficient patient: macro-ovalocytes (arrows), hypersegmented neutrophils (stars), teardrop-shaped RBCs (arrowhead). MCV often >115 fL. - Frameworks for Internal Medicine
Key Features
- Macro-ovalocytes (oval-shaped large RBCs)
- Hypersegmented neutrophils (>5% with ≥5 lobes, or any with ≥6 lobes)
- MCV often >115 fL
- Hypercellular marrow with maturation arrest
B12 vs. Folate Deficiency
| Feature | B12 Deficiency | Folate Deficiency |
|---|---|---|
| Neurological symptoms | YES (subacute combined degeneration of cord) | NO |
| Serum B12 | Low (<100 pg/mL) | Normal |
| Serum folate | Normal or high | Low |
| Red cell folate | Low | Low |
| Causes | Pernicious anemia, strict veganism, gastric surgery, terminal ileum disease | Poor diet, alcohol, pregnancy, methotrexate, phenytoin |
Never treat B12 deficiency with folate alone - it can mask the hematologic picture while neurological damage progresses irreversibly.
3. Hemolytic Anemias
Characterized by: elevated LDH, low/absent haptoglobin, elevated indirect bilirubin, reticulocytosis, and evidence of RBC fragmentation on smear.
Classification
Intrinsic (Red cell defect):
| Type | Disease | Mechanism |
|---|---|---|
| Membrane disorder | Hereditary spherocytosis | Mutations in ankyrin, band 3, spectrin, or band 4.2 → membrane fragments shed → spherocytes trapped in spleen |
| Enzyme deficiency | G6PD deficiency | Oxidative stress-triggered hemolysis; triggered by infections, fava beans, oxidant drugs |
| Enzyme deficiency | Pyruvate kinase deficiency | Glycolytic failure → rigid cells |
| Hemoglobin defect | Sickle cell disease | HbS polymerization → sickling |
| Hemoglobin defect | Thalassemia | Imbalanced globin chain production |
| Acquired (membrane) | PNH (paroxysmal nocturnal hemoglobinuria) | Loss of GPI-anchored complement regulators |
Extrinsic (External to red cell):
| Type | Examples |
|---|---|
| Immune-mediated | Autoimmune hemolytic anemia (warm IgG / cold IgM), transfusion reactions, drug-induced |
| Microangiopathic (MAHA) | TTP, HUS, DIC - schistocytes on smear |
| Mechanical | Defective cardiac valves, marathon running |
| Infection | Malaria, babesiosis |
Hereditary Spherocytosis key points:
- Spherocytes (small, dark, no central pallor) on smear
- Negative Coombs test (distinguishes from autoimmune HA)
- Splenomegaly (500-1000 g), pigment gallstones in 40-50% adults
- Splenectomy corrects anemia but spherocytes persist
4. Aplastic Anemia
Definition: Pancytopenia with hypocellular bone marrow. Diagnosis requires: bone marrow cellularity <25% of normal, OR <50% with <30% hematopoietic cells.
Pathophysiology
Acquired aplastic anemia is primarily an autoimmune disease - cytotoxic T cells attack hematopoietic stem cells, causing apoptosis and hematopoietic failure.
Causes
- Primary (idiopathic) - majority of acquired cases
- Drugs - chloramphenicol, NSAIDs, sulfonamides, gold, chemotherapy
- Viruses - EBV, CMV, hepatitis A/B/C (post-hepatitis aplasia)
- Radiation
- Autoimmune disorders
- PNH (classical form)
- Inherited - Fanconi anemia (chromosomal fragility), dyskeratosis congenita (telomerase mutations)
Clinical Features
- Fatigue, pallor, weakness (anemia)
- Petechiae, epistaxis, gum bleeding (thrombocytopenia)
- Recurrent infections (neutropenia)
- Bimodal age distribution: children/young adults + elderly (>60 years)
Severity Grading
| Grade | Criteria |
|---|---|
| Severe (SAA) | Marrow cellularity <25% + 2 of 3: neutrophils <0.5×10⁹/L, platelets <20×10⁹/L, reticulocytes <20×10⁹/L |
| Very severe (VSAA) | SAA criteria + neutrophils <0.2×10⁹/L |
Treatment
- Young patients (<40): Allogeneic HSCT (hematopoietic stem cell transplant) from matched sibling donor
- Older/no donor: Immunosuppression - anti-thymocyte globulin (ATG) + cyclosporine
5. Anemia of Inflammation / Chronic Disease (AI/ACD)
Most common anemia in hospitalized patients; second most common overall.
Pathophysiology
Cytokines (TNF-α, IL-1, IFN-γ) in chronic infection, inflammation, or malignancy:
- Raise hepcidin → iron trapped in macrophages → functional iron deficiency despite adequate stores
- Directly inhibit erythroid progenitor (BFU-E, CFU-E) proliferation
- Suppress EPO secretion
- Reduce RBC survival
Characteristics
- Mild-to-moderate anemia (Hb rarely <8 g/dL)
- Usually normocytic, normochromic (microcytic in 20-50% of cases)
- Low serum iron, low/normal TIBC, normal-to-high ferritin
- Low reticulocytes
- Storage iron normal or increased (key distinction from IDA)
- Conditions: chronic infection, rheumatoid arthritis, malignancy, CKD, IBD, HIV
Distinguishing AI from IDA
| Lab | IDA | AI/ACD |
|---|---|---|
| Serum iron | ↓ | ↓ |
| TIBC | ↑ | ↓ or normal |
| Ferritin | ↓ | ↑ or normal |
| Soluble transferrin receptor | ↑ | Normal |
Treatment
Treat the underlying disease. Consider IV iron or EPO stimulating agents (e.g., in CKD).
Summary Table: Quick Comparison
| IDA | Megaloblastic | Aplastic | Hemolytic | AI/ACD | |
|---|---|---|---|---|---|
| MCV | ↓ (micro) | ↑ (macro) | Normal | Variable | Normal |
| Retic count | ↓ | ↓ | ↓ | ↑ | ↓ |
| LDH | Normal | ↑ (intramedullary) | Normal | ↑↑ | Normal |
| Ferritin | ↓ | Normal | Normal | Normal/↑ | ↑ |
| Smear | Microcytes, target cells | Macro-ovalocytes, hyperseg neuts | Normal/pancytopenia | Spherocytes / schistocytes | Normal |
| BM | Normal/↓ iron stores | Hypercellular, megaloblasts | Hypocellular | Hyperplastic | Normal |
Diagnostic Approach
Low Hb/Hct → Check MCV
MCV LOW (microcytic)
→ Ferritin low: Iron deficiency anemia
→ Ferritin normal/high + low TIBC: Anemia of inflammation
→ Hb electrophoresis abnormal: Thalassemia
→ Ring sideroblasts on BM: Sideroblastic anemia
MCV HIGH (macrocytic)
→ Oval macrocytes + hyperseg neutrophils:
- Check B12 and folate
- Schilling test if pernicious anemia suspected
→ Round macrocytes: Alcohol, hypothyroidism, liver disease, drugs
MCV NORMAL (normocytic)
→ Reticulocyte count HIGH: Hemolysis or acute blood loss
- Check LDH, haptoglobin, Coombs test, smear
→ Reticulocyte count LOW: Hypoproliferative
- Bone marrow biopsy to differentiate aplastic anemia,
infiltration, myelodysplasia vs. EPO deficiency
Sources: Harrison's Principles of Internal Medicine 22E (2025), Robbins & Cotran Pathologic Basis of Disease 10E, Frameworks for Internal Medicine, Henry's Clinical Diagnosis & Management by Laboratory Methods, Goldman-Cecil Medicine, Sleisenger & Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.