Ak amputation in full detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full detailed response.
Above-Knee (Transfemoral) Amputation - Full Detail
Definition & Overview
Above-knee amputation (AKA), formally termed transfemoral amputation, is amputation of the lower extremity through the femoral shaft, proximal to the knee joint. It is the second most common major lower limb amputation level (after transtibial). The loss of the knee joint significantly increases the energy cost of walking and reduces the likelihood of successful prosthetic ambulation, especially in elderly dysvascular patients.
Levels of Transfemoral Amputation
Amputation through the thigh is classified into four levels based on the site of femoral transection:
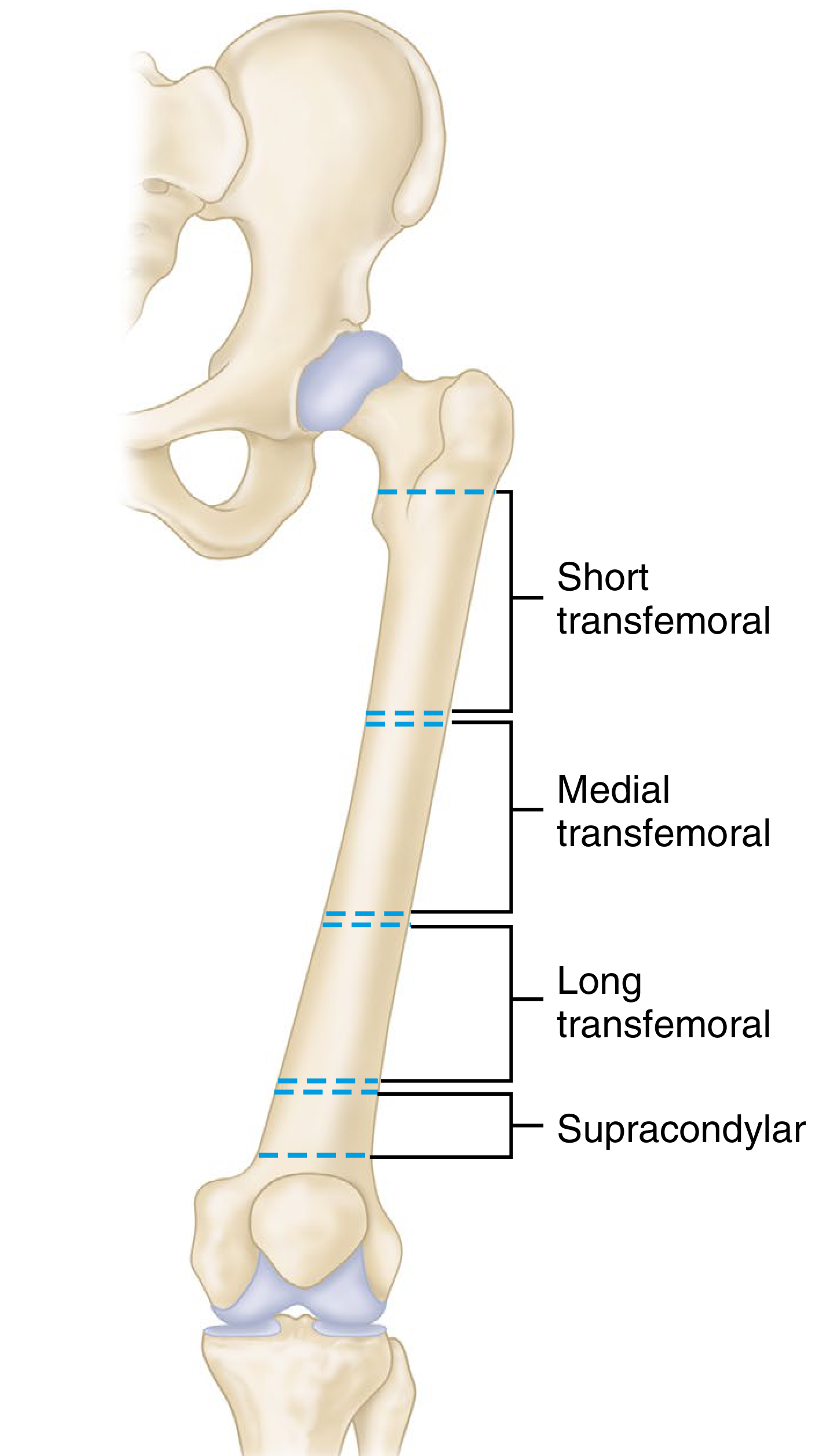
| Level | Description |
|---|---|
| Short transfemoral | Bone section within 5 cm distal to lesser trochanter - prosthetically managed as hip disarticulation |
| Medial transfemoral | Mid-femoral shaft level |
| Long transfemoral | Distal third of femur |
| Supracondylar | Just above the femoral condyles |
Key principle: The longer the residual femur, the better the lever arm for prosthetic control, suspension, and limb advancement. The optimum transfemoral bone length is 12 cm above the knee joint to accommodate the prosthetic knee unit.
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 886
- Miller's Review of Orthopaedics 9th Edition, p. 875
Indications
- Peripheral vascular disease (PVD) / ischemia - when ischemia extends too proximally for adequate soft tissue coverage of a below-knee stump
- Diabetic foot gangrene with proximal spread - wet, dry, or gas gangrene not amenable to distal amputation
- Failed below-knee amputation - wound breakdown, infection, or non-healing stump
- Severe trauma with irreparable neurovascular injury, unsalvageable limb
- Malignancy - soft tissue or bone tumors of the distal thigh/knee
- Severe infection - osteomyelitis, necrotizing fasciitis, gas gangrene
- Refractory infected total knee arthroplasty - when arthrodesis is not possible due to massive bone loss or life-threatening infection
- Non-ambulatory patients with severe tissue loss - bed-bound patients where healing at a lower level is not feasible
- Congenital deformity - when limb salvage is not functional
Relative indication: Patients with pre-existing non-ambulatory status, dementia, severe hip/knee contractures, or stroke with paralysis are often better served by an AKA rather than BKA, as prosthetic use is unlikely regardless.
- Fischer's Mastery of Surgery 8th Ed, p. 6626-6627
- Current Surgical Therapy 14e, p. 1195
Contraindications / When to Choose a Lower Level
Knee disarticulation or transtibial amputation is preferred over AKA whenever possible because:
- Every centimeter of limb length preserved reduces energy expenditure of ambulation
- Patients with transfemoral amputations and PVD are unlikely to become efficient prosthetic walkers
- The energy cost of bilateral AKA prosthetic ambulation is 4-7 times normal oxygen consumption
A through-knee (knee disarticulation) level is preferred over AKA because it:
- Causes minimal muscle transection and less intraoperative bleeding
- Preserves a longer lever arm for transfers
- Creates an end-weight-bearing stump
- Avoids knee flexion contracture seen at BKA level
- Reduces metabolic cost of ambulation compared with transfemoral amputation
Relevant Anatomy
Thigh Compartments (at AKA level)
Anterior compartment:
- Bounded by lateral and anteromedial intermuscular septa (attached to fascia lata and linea aspera)
- Contains: quadriceps femoris (vastus lateralis, medialis, intermedius, rectus femoris), sartorius
- Innervated by the femoral nerve
Medial (adductor) compartment:
- Contains: adductor longus, adductor brevis, adductor magnus, gracilis
- Innervated by the obturator nerve
- Contains the adductor canal (femoral artery, femoral vein, saphenous nerve/nerve to vastus medialis at mid-thigh and above)
Posterior compartment:
- Contains: semimembranosus, semitendinosus, biceps femoris (long and short heads)
- Innervated by the sciatic nerve (posteromedial at distal thigh - may present as medial tibial nerve + lateral common peroneal nerve)
- At distal thigh: sciatic nerve is posterolateral to biceps femoris
Superficial fascia:
- Greater saphenous vein runs from 8-10 cm posterior to medial patella toward pubic tubercle
- Large communicating branch between small and great saphenous veins may ascend around medial thigh
- Duplication of great saphenous vein may occur in distal thigh
Deep fascia (fascia lata):
- Thicker proximally and laterally (reinforced by iliotibial tract - tensor fascia lata + gluteus maximus)
- Reinforced distally by fibrous expansions from biceps femoris, sartorius, and quadriceps
Vascular structures:
-
Superficial femoral artery and femoral vein travel between vastus medialis and sartorius
-
At/above adductor hiatus: popliteal artery and vein encountered posteriorly
-
Profunda femoris (deep femoral artery): terminal perforating branches posteromedial to femur; main terminal profunda may require suture ligation if SFA is occluded
-
Fischer's Mastery of Surgery 8th Ed, p. 6657-6659
Preoperative Considerations
- Vascular assessment - confirm level of viable tissue; Doppler/ABI, angiography if revascularization is possible
- Nutritional optimization - albumin, pre-albumin; malnutrition impairs wound healing
- Glycaemic control in diabetics
- Antibiotic prophylaxis - for infection/gangrene cases
- Assess rehabilitation potential - determines whether adductor myodesis (adds operative time) is worthwhile; not recommended for frail, elderly dysvascular patients unlikely to use a prosthesis
- Patient counseling on prosthetics, rehabilitation, and energy demands
- Tourniquet - can be used in nonischemic limbs; not appropriate in dysvascular disease
Surgical Technique (Transfemoral Amputation)
Patient Positioning
- Supine on the operating table
- Tourniquet applied proximally for non-ischemic limbs
Skin Incision - Fishmouth (Anterior and Posterior Flaps)
The classic incision is a fish-mouth creating roughly equal anterior and posterior flaps:
- Mark the distal aspect of the anterior flap ~2 cm proximal to the patella
- The corners (where the two flaps meet at 3 o'clock and 9 o'clock positions) are placed ~10 cm from the knee joint
- The femur will be transected approximately 12 cm from the knee joint
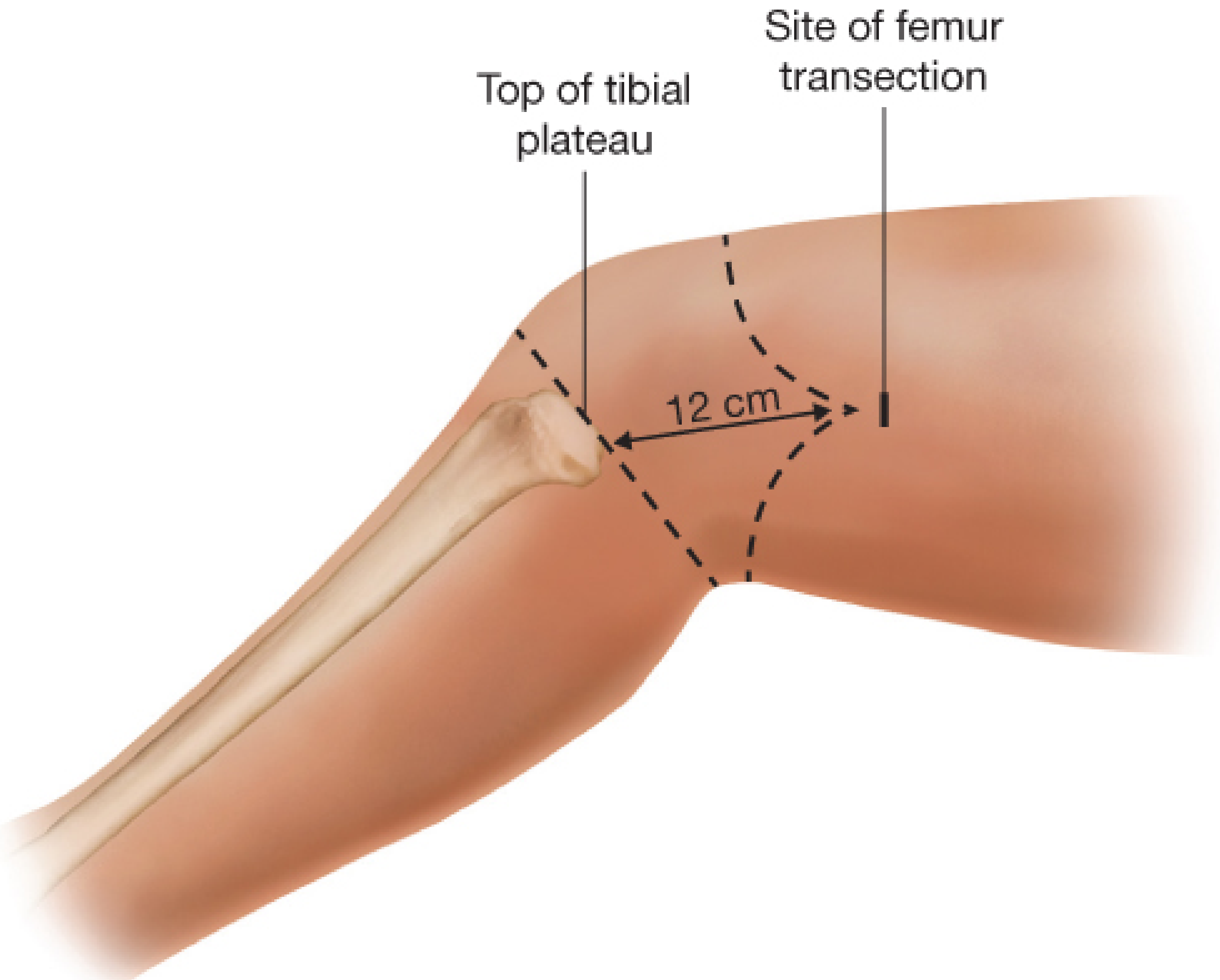
- The posterior flap can be made slightly longer (1-2 cm) if needed - particularly if the patient has a large lower extremity - to move the scar line away from the dependent/posterior position and to ensure tension-free closure
- In dysvascular patients: the femur may be transected as proximal as needed for skin closure (typically in the distal one-third of the femur, but more proximal if required)
- In ambulatory candidates: preserving maximum femoral length is the priority
Step-by-Step Operative Technique (Campbell's Technique 18.5)
- Outline equal anterior and posterior skin flaps beginning proximally at the predicted bone section level. Each flap length should be at least one-half the anteroposterior diameter of the thigh at that level.
- Fashion the anterior flap with an incision starting at the midpoint of the medial aspect of the thigh at the bone section level, curving distally and laterally across the anterior thigh, then curving proximally to the lateral aspect.
- Fashion the posterior flap in a comparable manner.
- Deepen skin incisions through subcutaneous tissue and deep fascia; reflect flaps proximally to the bone section level.
- Divide the quadriceps muscle and overlying fascia along the anterior incision and reflect proximally as a myofascial flap. Leave the four muscle bellies at least three-quarters of the femoral diameter longer than the planned femoral transection level to support myodesis.
- Be mindful of the greater saphenous vein medially - suture ligate it.
- The superficial femoral artery and femoral vein are identified between the vastus medialis and sartorius and suture ligated separately. If the femoral artery is diseased or contains a stent, it can be divided with heavy scissors or wire cutters.
- Identify and divide the saphenous nerve (or femoral nerve if proximal amputation) under tension.
- Release posterior femoral attachments with electrocautery to prepare the posterior flap.
- Clear the femur periosteum ~2 cm proximal to the flap corners (approximately 12 cm from knee joint) using a periosteal elevator.
- Protect surrounding soft tissue with large skin hooks anteriorly and malleable retractors/laparotomy pad posteriorly.
- Transect the femur with a power saw or Gigli saw.
- Elevate the femur end with a bone hook and divide the posterior compartment muscles along the contour of the posterior incision using an amputation knife.
- If medial hamstring myodesis is planned: leave medial hamstring long enough to cover the entire distal femur; otherwise leave both hamstrings ~three-quarters of the femoral diameter longer than the femur.
- Ligate any arterial/large venous bleeding; secure muscular hemostasis.
- Identify the sciatic nerve: place on tension, ligate proximally with absorbable suture, and sharply transect, allowing it to retract proximally (prevents painful neuroma at stump end).
- Ligate the tertiary perforating branches of the deep femoral artery posteromedially; suture ligate the terminal profunda if well-developed.
- Contour the femoral edges with a rasp or saw to smooth all sharp edges.
- Fischer's Mastery of Surgery 8th Ed, p. 6641-6644
- Sabiston Textbook of Surgery, p. 2345
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 886
Adductor Myodesis (Key Step for Ambulatory Patients)
Why it matters:
- Without myodesis of the adductor magnus, most transfemoral amputations result in at least 70% loss of adduction power
- The adductor magnus inserts at the adductor tubercle just proximal to the medial epicondyle; transecting it leaves the hip abductors unopposed, creating abduction deformity and inefficient widened gait
- Adductor myodesis maintains femoral adduction during stance phase, enabling optimal prosthetic function
Technique (Fischer's method):
- Dissect the adductor muscle off its femoral attachment, preserving length
- Drill four holes from the anterior midline to the lateral edge of the femur:
- For right AKA: 12 o'clock, 10:45, 9:30, 8 o'clock positions
- For left AKA: 12 o'clock, 1:15, 2:30, 4 o'clock positions
- Pass three #2 Ticron sutures through the four holes
- The lateral suture secures the adductor magnus to the femur
- The anterior suture secures the medial hamstring
- The anterolateral suture reinforces both adductor magnus and medial hamstring myodesis
- Locking suture technique within muscle and tendon is preferred
Note: Adductor myodesis requires additional operative time and may not be worthwhile in frail, elderly, dysvascular patients unlikely to ambulate with a prosthesis.
- Miller's Review of Orthopaedics 9th Edition, p. 875
- Fischer's Mastery of Surgery 8th Ed, p. 6644
Wound Closure
- Approximate the deep fascia of the distal anterior and posterior flaps with interrupted 2-0 Vicryl sutures over the femoral shaft (myoplasty layer)
- Perform interrupted Vicryl sutures to fully approximate both fascial flaps
- Close the skin with vertical mattress interrupted nylon sutures (or deep dermal absorbable sutures + staples)
- A closed suction drain may be placed at the surgeon's discretion
- Apply a gauze dressing with compression ace bandage
Nerve Handling - General Principles
All major nerves (sciatic, saphenous/femoral) must be:
- Put on tension before division
- Ligated proximally with absorbable suture (prevents neuroma formation)
- Sharply transected under tension, allowing the nerve to retract proximally
This technique allows the nerve ending to retract away from the prosthetic-bearing surface, preventing painful neuromas at the residual limb end.
Postoperative Management
Dressing & Stump Care
| Patient Type | Recommended Dressing |
|---|---|
| Elderly dysvascular | Soft dressing (elastic compression); rigid dressing difficult to maintain at this level |
| Young, non-ischemic | Rigid immediate postoperative dressing + early weight-bearing with locked-knee pylon |
- Elastic compression dressings may be suspended about the opposite iliac crest for suspension
- Rigid dressings are difficult to apply and maintain at transfemoral level
Complications to Monitor
- Wound dehiscence/breakdown - most common complication, especially in dysvascular patients
- Wound infection / hematoma - drained if needed; closed suction drain helps
- Phantom limb pain - pain perceived in the amputated limb; common, managed with medications, mirror therapy, targeted muscle reinnervation (TMR)
- Stump neuroma - from inadequate nerve retraction
- Hip flexion contracture - major complication; mitigated by:
- Hip extension exercises
- Formal physical therapy
- Prone positioning postoperatively
- Avoiding prolonged sitting/wheelchair positioning
- Abduction deformity - from inadequate adductor myodesis (unopposed abductors)
- Skin breakdown over bony prominences - especially prominent distal femur if anterior femur not covered by soft tissue; adductor myodesis helps here
- Reamputation - for non-healing or proximal spread of infection
Rehabilitation After Transfemoral Amputation
The loss of the knee joint exponentially increases energy expenditure for locomotion with a prosthesis. This has major consequences for:
- Cardiac patients
- Patients with ischemic contralateral limbs
- Bilateral AKA patients (O₂ consumption is 4-7 times normal)
Key facts:
- Many transfemoral amputees with vascular disease never use a prosthesis consistently
- Patients with bilateral transfemoral amputations often choose wheelchair use for speed
- Younger patients with non-ischemic amputations progress more rapidly
Rehabilitation Protocol
| Phase | Activity |
|---|---|
| Immediate post-op | Soft dressing (dysvascular); rigid dressing + pylon (young/non-ischemic) |
| Early | Hip extension exercises to prevent flexion contracture; formal PT |
| Weight-bearing | Best delayed until sutures/staples removed for comfort |
| Progression | Ambulation with unlocked prosthetic knee; reduce upper extremity support |
| Definitive prosthesis | Fitted after stump maturation (typically 6-12 weeks) |
Prosthetic Options
A variety of prosthetic knee units are now available:
-
Conventional constant-friction knee - extends 9-10 cm distal to socket end; requires femur transected ≥9-10 cm proximal to knee
-
Computer-assisted (microprocessor) knee - uses hydraulic or magnetic units; sensitive sensors allow more natural knee motion, especially deceleration during swing phase; accommodates shorter distal femoral segments
-
Osseointegrated implants - emerging technique for select transfemoral amputees
-
Campbell's Operative Orthopaedics 15th Ed 2026, p. 886-888
-
Miller's Review of Orthopaedics 9th Edition, p. 875
Special Situations
Guillotine Amputation (Emergency)
In emergent cases (e.g., rapidly spreading gas gangrene, septic shock), a guillotine amputation can be performed:
- Done as quickly as possible and as distally as possible
- Goal: remove necrotic/infected tissue rapidly without wound closure
- Bleeding vessels ligated; vacuum or gauze dressing placed
- This is temporary and lifesaving; formal amputation follows in days when the patient is stabilized
Cryoamputation (Critically Ill)
For patients in septic shock on multiple vasopressors unfit for OR:
- A Styrofoam cooler filled with dry ice is placed around the infected extremity
- A warming pack is applied proximal to the cooler to protect proximal tissue
- Isolates infected limb from the circulation by extreme cold
- Bridge therapy until the patient is stable enough for formal OR amputation
Short Transfemoral Stump (<5 cm from lesser trochanter)
- Functions and is prosthetically fitted as a hip disarticulation
- Standard above-knee prosthesis cannot be effectively used
Comparison: AKA vs. Adjacent Levels
| Feature | BKA | Knee Disarticulation | AKA |
|---|---|---|---|
| Knee preserved | Yes | No (but end-bearing) | No |
| Energy cost of walking | Lowest | Intermediate | Highest |
| Prosthetic walking (vascular) | Reasonable | Possible | Often not achieved |
| Prosthetic fitting | Easiest | Moderate (improved with Mazet technique) | More complex |
| Stump stability | Good | Excellent (end-bearing) | Requires myodesis |
| Hip flexion contracture risk | Moderate | Lower | Higher |
Sources
- Fischer's Mastery of Surgery 8th Ed, pp. 6626-6644 (detailed AKA surgical technique, anatomy, myodesis)
- Campbell's Operative Orthopaedics 15th Ed 2026, pp. 886-888 (technique 18.5, rehabilitation)
- Miller's Review of Orthopaedics 9th Edition, p. 875 (adductor myodesis, prosthetics)
- Sabiston Textbook of Surgery, p. 2345 (AKA principles)
- Current Surgical Therapy 14e, pp. 1195-1196 (transfemoral amputation, cryoamputation)
This is a shared conversation. Sign in to Orris to start your own chat.