45 years old male with bilateral pedal edema with diffuse body swelling with generalized body pain tell me differentials diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative data from multiple major textbooks. Here is the full clinical answer:
Differential Diagnosis: 45-Year-Old Male with Bilateral Pedal Edema, Diffuse Body Swelling, and Generalized Body Pain
The combination of bilateral pedal edema + diffuse/generalized swelling (anasarca) points toward a systemic cause rather than a local venous or lymphatic problem. The added feature of generalized body pain narrows and expands the list simultaneously - pointing toward inflammatory, endocrine, or musculoskeletal etiologies in addition to the classic triad.
Robbins & Kumar: Pathologic Basis of Disease - mechanisms of systemic edema
Pathophysiologic Framework
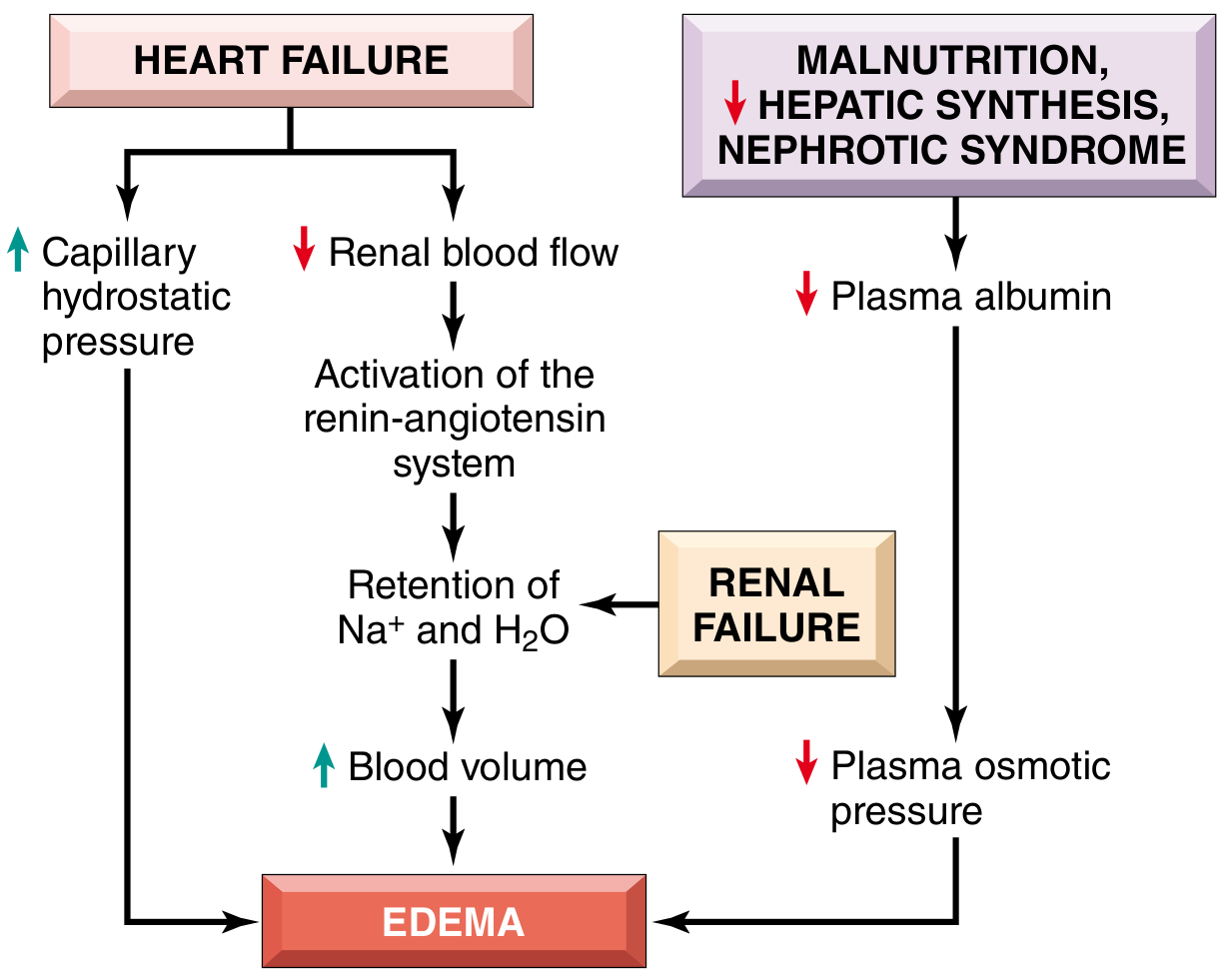
Generalized edema results from four main mechanisms (Robbins & Kumar):
| Mechanism | Key Examples |
|---|---|
| Increased hydrostatic pressure | Congestive heart failure, constrictive pericarditis, cirrhosis |
| Reduced plasma oncotic pressure | Nephrotic syndrome, cirrhosis, malnutrition |
| Sodium and water retention | Renal failure, hyperaldosteronism |
| Increased vascular permeability | Inflammation, sepsis, angioedema |
Priority Differentials (Most Common - "Big 3")
1. Congestive Heart Failure (CHF)
- Most common cause of bilateral pedal edema + anasarca in middle-aged males
- Bilateral pedal edema, exertional dyspnea, orthopnea, PND, raised JVP, S3 gallop
- Body pain may reflect poor cardiac output and skeletal muscle fatigue/hypoperfusion
- Types: Heart failure with reduced EF (HFrEF) and preserved EF (HFpEF)
- Constrictive pericarditis should also be considered
2. Nephrotic Syndrome
- Hallmark: massive proteinuria (>3.5 g/day) → hypoalbuminemia → generalized edema, including periorbital edema
- Frothy urine, hypoalbuminemia, hyperlipidemia, lipiduria
- Causes include: minimal change disease, membranous nephropathy, focal segmental glomerulosclerosis, diabetic nephropathy
- Generalized body pain may be due to associated muscle wasting or thromboembolic complications
3. Hepatic Cirrhosis
- Portal hypertension + hypoalbuminemia (reduced hepatic synthesis) → ascites + peripheral edema
- Look for: jaundice, spider angiomas, palmar erythema, gynecomastia, caput medusae, splenomegaly
- Often associated with coagulopathy, encephalopathy
- Body pain from muscle cramps (hypomagnesemia, hypokalemia) or musculoskeletal wasting
Secondary / Important Differentials
4. Chronic Kidney Disease (CKD) / Renal Failure
- Sodium and water retention → diffuse edema
- Associated uremic symptoms: generalized body aches, pruritus, fatigue, nausea
- Hypertension, oliguria, elevated creatinine/BUN
- Uremic myopathy and neuropathy can cause body pain directly
5. Hypothyroidism (Myxedema)
- Non-pitting edema (myxedema) from glycosaminoglycan deposition in tissues
- Fatigue, weight gain, cold intolerance, constipation, bradycardia
- Generalized myalgia and body aches are a classic feature
- In severe cases: pericardial/pleural effusions, ascites, anasarca
6. Hypoalbuminemia from Nutritional Causes / Malabsorption
- Protein-energy malnutrition or protein-losing enteropathy
- Reduced plasma oncotic pressure → dependent edema
- Body pain may reflect cachexia, vitamin deficiencies (e.g., thiamine deficiency causing wet beriberi)
7. Sepsis / Systemic Inflammatory Response
- Capillary leak syndrome → generalized edema
- Fever, tachycardia, altered sensorium, focal source of infection
- Diffuse myalgia and body pain are prominent presenting features
- Can be associated with SIADH and hyponatremia
8. Filariasis (Parasitic - important in endemic regions)
- Lymphatic obstruction by Wuchereria bancrofti → lymphedema of legs
- Recurrent fever, lymphangitis, generalized myalgia
9. Drug-Induced Edema
- Calcium channel blockers (amlodipine, nifedipine) - most common drug cause
- NSAIDs, corticosteroids, thiazolidinediones, minoxidil, testosterone
- Some cause myalgia as well (e.g., corticosteroids - steroid myopathy)
10. Advanced Malignancy / Paraneoplastic Syndrome
- Bilateral pelvic/retroperitoneal lymphadenopathy causing bilateral lower extremity edema
- Hypoalbuminemia from cachexia
- Generalized bone pain, weight loss, constitutional symptoms
Additional Differentials to Consider (with Body Pain as a Key Feature)
| Diagnosis | Edema Mechanism | Body Pain Mechanism |
|---|---|---|
| Polymyositis / Dermatomyositis | Inflammatory, capillary leak | Proximal muscle inflammation |
| Rheumatoid arthritis (systemic) | Inflammatory | Joint and systemic pain |
| Systemic Lupus Erythematosus (SLE) | Lupus nephritis/hypoalbuminemia | Polyarthralgia, serositis |
| Amyloidosis | Nephrotic pattern OR cardiac infiltration | Peripheral neuropathy, myopathy |
| Wet Beriberi (Thiamine deficiency) | High-output cardiac failure | Peripheral neuropathy, myalgia |
| Hypervolemia (IV fluid overload / SIADH) | Sodium/water excess | Hyponatremic muscle cramps |
| Chronic venous insufficiency | Venous hypertension | Leg heaviness, aching pain |
Recommended Initial Workup
To narrow the differentials, the following are essential:
Basic panel:
- CBC, ESR, CRP
- Serum albumin, total protein
- LFTs (AST, ALT, ALP, bilirubin, PT/INR)
- Renal function (creatinine, BUN, eGFR), electrolytes
- Urine routine + microscopy + urine protein:creatinine ratio (or 24-hr urine protein)
- Serum TSH, Free T4
Cardiac:
- ECG
- Chest X-ray (cardiomegaly, pleural effusions)
- Echocardiogram (EF, wall motion, pericardial effusion)
Additional:
- Serum lipid profile (if nephrotic syndrome suspected)
- Serum protein electrophoresis (SPEP) if amyloidosis/myeloma suspected
- ANA, anti-dsDNA if SLE is in the differential
- Serum CK, aldolase if inflammatory myopathy suspected
Clinical Prioritization for This 45-Year-Old Male
Given the age, sex, and combination of bilateral pedal edema + diffuse swelling + generalized body pain, the top 5 must-rule-out diagnoses are:
- Congestive Heart Failure - most common, high morbidity
- Nephrotic Syndrome - silent until anasarca
- Hepatic Cirrhosis - especially if alcohol history
- CKD - progressive and often asymptomatic until late
- Hypothyroidism - highly treatable, often missed; body pain is a hallmark clue
Sources: Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed. | Robbins & Kumar: Basic Pathology | Robbins, Cotran & Kumar: Pathologic Basis of Disease | Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.